Article Text

Abstract
Post-transplant lymphoproliferative disorder (PTLD) of the oesophagus is a rare complication of solid organ transplant that requires a high index of suspicion to diagnose. A literature review conducted on Ovid Medline database retrieved 24 articles, among which five previous cases of oesophageal PTLD were identified. Development of oesophageal strictures related to PTLD has not been reported in the literature. We report a case of oesophageal PTLD following lung transplant, presenting with extensive, circumferential ulceration in the oesophagus. PTLD was successfully treated with chemotherapy but subsequently, this patient developed a severe oesophageal stricture at the site of her PTLD. She presented with an episode of food bolus impaction requiring endoscopic retrieval. In the following years, our patient required multiple endoscopic dilatations of this PTLD-related oesophageal stricture.
- oesophageal cancer
- oesophageal strictures
- gastrointestinal lymphoma
- lymphoma
- oesophagitis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Post-transplant lymphoproliferative disorder (PTLD) is one of many serious complications that follow transplantation of solid organs or haematologic stem cells. Development of PTLD is commonly a result of uncontrolled B cell proliferation in the context of Epstein-Barr virus (EBV) infection.1
The clinical presentation of PTLD is variable, with some patients being completely asymptomatic and others presenting in critical condition with multiorgan involvement. Common organ involvement in PTLD includes lymph nodes, the central nervous system and gastrointestinal system.2
Although gastric, colonic and small bowel involvement with PTLD have been reported in the literature with an estimated prevalence of 25% of all PTLD in paediatric patients,2 isolated oesophageal PTLD is exceedingly rare.
A literature review has discovered five reported cases1–5 of isolated oesophageal PTLD. We present a case of oesophageal PTLD that was complicated by stricture formation which required multiple endoscopic dilations over the follow-up period.
Case
A 35-year-old woman with a history of mixed connective tissue disease, Raynaud’s phenomenon, arthritis, progressive interstitial lung disease resulted in respiratory compromise that required a double lung transplant. One year following her transplant, she was referred to the gastroenterology service with a 2-week history of worsening odynophagia and dysphagia.
Her symptoms were predominantly caused by solids with the need to over-chew or to drink large quantities of liquids to push food down the oesophagus. She lost 4 kg. She reported occasional nausea and regurgitation of food and pills, but no vomiting. There were no other gastrointestinal symptoms. She reported no fever or night sweats.
Her immunosuppressive medications included prednisone, tacrolimus and mycophenolate.
She had no allergies. There was no history of smoking, excessive alcohol consumption or recreational drug use.
There was no family history of malignancies.
Physical examination did not reveal any skin rashes or lymphadenopathy. Abdominal examination was normal.
Investigation
A complete blood count revealed haemoglobin of 87 g/L (normal range: 120–160), low lymphocytes of 1.01×109/L (normal range: 1.50–4.00), high monocytes at 1.15×109/L (normal range: 0.20–0.80) and elevated platelet at 560×109/L (normal range: 150–400). Lactate dehydrogenase was elevated at 368 U/L (normal range: 120–220).
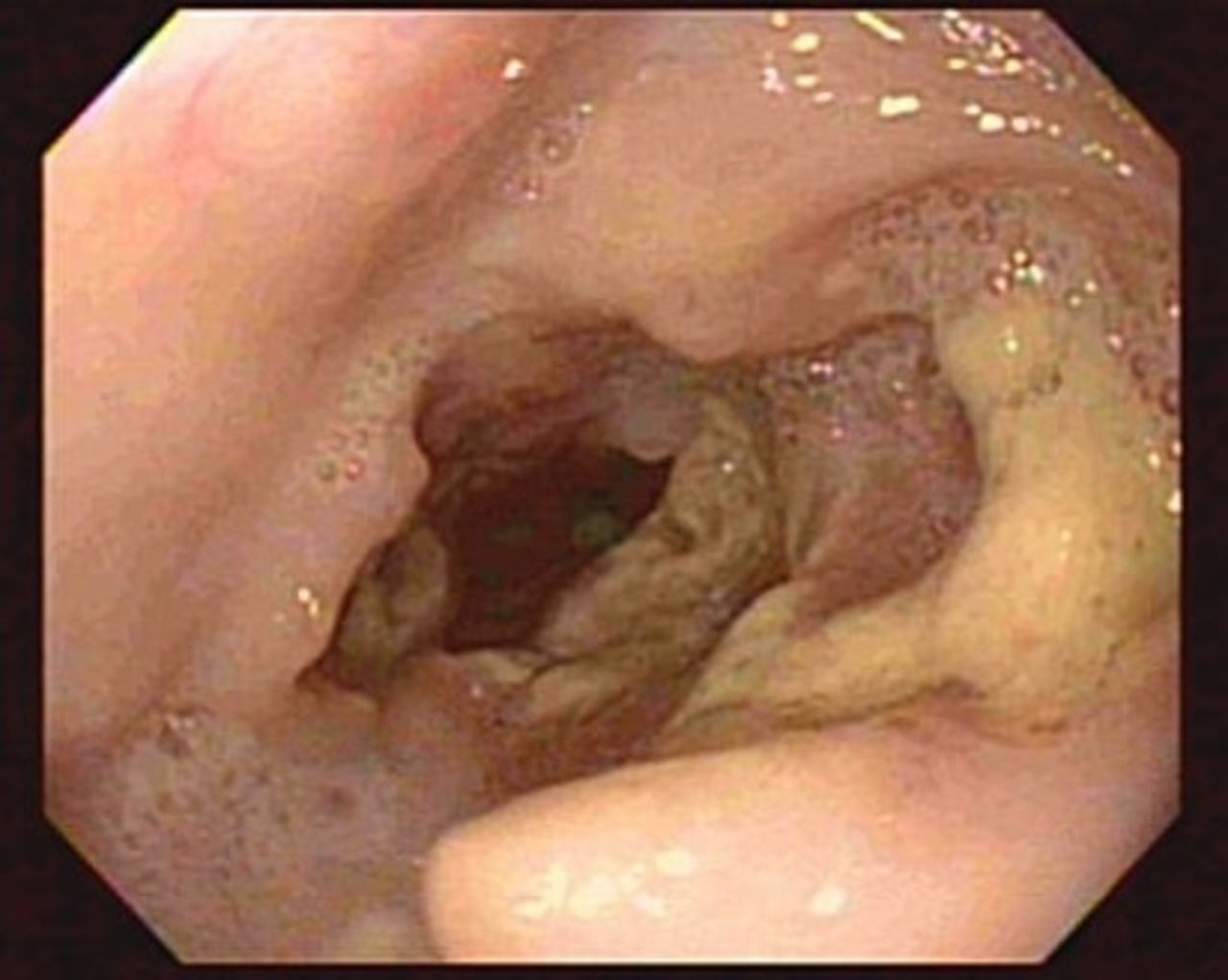
An upper endoscopy demonstrated extensive, ulcerations involving most of the oesophagus except the distal 3–4 cm, occupying at least 70% of the circumference, with minimal normal intervening mucosa. Oesophageal ulcers were wide and deep with rolled edges and a whitish base (figure 1). The distal 3–4 cm of the oesophagus was spared and showed no oesophagitis or Barret’s oesophagus. Endoscopic examination of the stomach and the duodenum was unremarkable.

Endoscopic image showing deep, extensive ulceration in the oesophagus.
Biopsies from the edges of the ulcers showed granulation tissue and inflammatory exudate with no evidence of viral cytopathic effects. Brushing was positive for Candida albicans.
Work-up for the differential diagnosis included Cytomegalo virus blood PCR which was negative. Blood PCR for EBV was detected at 7.88E+03 copies of DNA/mL (negative if less than 600 copies of DNA/mL).
A course of antifungal therapy for oesophageal candidiasis was completed but symptoms persisted. A repeat endoscopy revealed that the oesophagus was unchanged. Biopsies were obtained from the bases of ulcers and revealed EBV-positive large B cell lymphoproliferative disorder consistent with monomorphic PTLD. There was multifocal necrosis and high apoptotic rate. Duodenal and stomach biopsies were normal.
CT of the thorax showed circumferential, irregular thickening of a long segment of the oesophagus associated with some mildly enlarged lymph nodes in the mediastinum. The remainder of the staging work-up including a bone marrow biopsy and CT scans of the head, neck, abdomen and pelvis showed no evidence of PTLD elsewhere. Colonoscopy was not indicated given lack of clinical symptoms of colonic PTLD and negative imaging.
Rituximab single agent treatment was started initially, but did not result in complete remission of PTLD. Therefore, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine/(oncovin) and prednisone) chemotherapy was initiated. Subsequent to that, the patient had resolution of dysphagia and odynophagia, negative blood EBV PCR, decreased oesophageal thickening on CT and confirmed healing oesophageal ulcers on endoscopy.
However, a few weeks after completion of chemotherapy, she developed sudden-onset dysphagia with sensation of food impaction in her oesophagus and presented to the hospital. A barium swallow showed a severe stricture in the mid-oesophagus for about 3.5 cm, with the narrowest part of the lumen measuring 4 mm (figure 2). Endoscopy revealed significant dilatation in the upper oesophagus with a food bolus noted. This bolus required endoscopic retrieval using a Roth net. Distal to this, there was a stenotic area which was non-traversable by the gastroscope and measured about 4.5 mm in diameter. CRE balloon dilation was performed (from 8 mm to 10 mm). Biopsies from the stenotic segment and from the dilated upper oesophagus were obtained and were negative for PTLD.

{kind=link}
{kind=link}
Barium study demonstrating severe stricture in the mid-thoracic oesophagus for about 3.5 cm, with the narrowest part of the lumen measuring 4 mm.
A 24-hour pH monitoring showed no episodes of acid reflux and no symptoms were recorded during the study.
Follow-up
Over the span of the following years, this patient required multiple endoscopic dilatations to allow for relief of dysphagia. Repeated oesophageal biopsies were negative for recurrent lymphoma. CT scans remained stable with no evidence of PTLD.
Learning points
Presence of oesophageal Candida and/or viral (Cytomegalo virus) infections have been co-incidentally reported in patients with oesophageal PTLD.
Maintain a high index of suspicion for PTLD in immunosuppressed patients with clinical symptoms refractory to treatment with antimicrobials.
Repeat endoscopy with deep biopsies from ulcer base may increase the yield for PTLD detection.
Discussion
The association between EBV infection, the cumulative burden of immunosuppressive treatment (specifically T cell depleting strategies) and the higher risk of PTLD is well established.1
A literature review conducted on Ovid Medline database retrieved 24 articles, among which five previous cases of oesophageal PTLD were identified (online supplemental material).1–5 There were four adult cases1 3–5 and one paediatric case.2 During the pre-transplant work-up, all of the adult recipients were EBV positive. Interestingly; however, the 8-year-old transplant recipient was EBV negative but developed acute tonsillitis 4 months after his transplant from an EBV-positive donor.2
Supplemental material
All of these oesophageal PTLD cases followed solid organ transplantation and were EBV-driven as confirmed by pathology and/or serology. The interval for PTLD development ranged from 6 months2 to 31 years5 following transplant.
In conclusion, we describe a case of PTLD primarily involving the oesophagus. After PTLD was treated, an oesophageal stricture occurred at the site of previous PTLD involvement, likely as a result of scar tissue formation after healing of circumferential ulcers. To the best of our knowledge, this is the first case in the literature with PTLD leading to an oesophageal stricture.
In our case, the initial endoscopic biopsies were non-specific and brushings were positive for oesophageal candidiasis; however, the endoscopic appearance was atypical for Candida infection and patient’s symptoms did not respond to antifungal therapy. Therefore, we elected to repeat endoscopy and obtain more biopsies from the ulcer base, and this eventually confirmed PTLD. This underlines the importance of maintaining a high index of suspicion and the value of repeat endoscopy and biopsies in cases where endoscopic findings are atypical and whenever there is no resolution of symptoms despite treatment.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MSM and SLW contributed to the planning of this case report, equally. MSM conducted the literature review and wrote the case report. SLW reviewed/edited the manuscript, and provided supervision. SLW arranged clinical follow-up with the patient and obtained consent. MSM submitted the report and edited the submission according to the review comments.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.