Article Text

Abstract
Inflammatory bowel diseases such as ulcerative colitis (UC) may be complicated by several extraintestinal manifestations. These involve joints, skin, eyes and less commonly lungs and heart. Myocarditis may result from the toxic effect of drugs (ie, mesalazine) commonly used for the treatment of UC or due to infections (eg, Coxsackieviruses, enteroviruses, adenovirus). Here, we report a case of a 26-year old man affected by UC and complicated by two episodes of myocarditis. Both episodes occurred during two severe exacerbations of UC. However, in both cases the aetiology of myocarditis remains uncertain being ascribable to extraintestinal manifestation, drug toxicity or both.
- ulcerative colitis
- IBD
- drug toxicity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Inflammatory bowel diseases (IBD), such as ulcerative colitis (UC) and Crohn’s disease, are chronic inflammatory intestinal disorders, characterised by alternating periods of remission and relapse. It is well known that many factors including genetics, immune system, environment and gut microbiome may contribute to the onset of IBD.1–4 The incidence of IBD is increasing worldwide with 6,8 million cases in 2017.5
Moreover, IBD can be associated with several extra-intestinal manifestations, mainly during acute exacerbations, in up to 30% of patients.6 Extraintestinal complications of IBD include joints (ankylosing spondylitis and spondyloarthropathies), eyes (uveitis), skin (pyoderma gangrenosum and erythema nodosum) and less commonly lugs (pleuritis) and heart (pericarditis and myocarditis) disorders.6 Myocarditis is a rare extraintestinal complication of IBD with a reported incidence of 6 cases over 15 000 patients.7 Interestingly, the incidence of myocarditis was slightly higher among patients with IBD compared with the general population.2 Despite rare, cardiac extraintestinal manifestations, such as pericarditis and myocarditis, are more commonly reported to occur in UC than Crohn’s disease patients.7 In addition, in patients with IBD myocarditis could be triggered by drugs currently used to treat this condition8–19 such as mesalazine (MSZ) or biological agents,20 and in newly diagnosed IBD.21 Last but not least, Coxackie viruses, Parvovirus B19, Adenoviruses and enteroviruses can be aetiological agents for myocarditis.
Here, we report a clinical case of a young man affected by UC who had two episodes of myocarditis.
Case report
A 26-year-old male patient was admitted to our Internal Medicine Unit of SS Annunziata Hospital in Cento (Ferrara, Italy) in July 2018 because of fever, bloody diarrhoea (up to 10 bowel movements per day) and abdominal pain. His medical history reported a previous diagnosis of pancolitis in July 2017 successfully treated with oral MSZ (4.8 g/day) and beclomethasone (5 mg/day). The patient had no cardiovascular risk factors. On admission, laboratory tests showed an increase in white cell count (WCC) (18.28×109/L; normal value (n.v.): 4.00–11.00 x 109/L), C reactive protein (CRP) (8.51 mg/dL; n.v.:<0.5 mg/dL) and faecal calprotectin (4763 mg/kg; n.v.: <50 mg/kg). During the hospitalisation, the patient reported several episodes of severe chest pain associated with dyspnoea with no ECG abnormalities. Due to the persistence of these episodes, the patient was tested for troponin I (TnI) that turned to be positive (0.24 ng/mL; n.v.: <0.04 ng/mL). Echocardiography showed a hypokinetic area of the apical anterior aspect of the myocardium with a reduced ejection fraction (50%). Thus, a cardiac MRI was performed. According to Lake Louis Criterion, cardiac MRI, with at least 2 (oedema and necrosis) positive criteria, confirmed a diagnosis of myocarditis (figure 1A). The patient was tested for common infective causes of myocarditis. Stool examination for Adenovirus and bacteria (Shigella, Salmonella, Campylobacter, Escherichia coli O157h7, and Yersinia enterocolitica) resulted negative. Specific viral serological antibodies resulted negative: IgG anti-Coxackie B virus was 2.4 U/mL (n.v.: <11 U/mL; positive >15 U/mL), and IgM anti-Coxackie B virus 6.3 U/mL (n.v.:<10 U/mL; positive >15 U/mL), IgM anti-Herpes simplex 1 and 2 was 0.53 (n.v.: <0.9; positive >1.1), and IgM anti-Herpes zoster 0.26 (n.v.: <0.9; positive >1.1). Thus, these data led us to think that myocarditis was attributed to MSZ and the treatment was shifted to azathioprine (AZA) 150 mg/day associated with methylprednisolone 1 mg/kg/day for 7 days, tapered down until discontinuation. This therapeutic approach promoted remission of UC and troponin I (TnI) normalisation within 7 days. The clinical picture and the lab tests improved (WCC: 16.98×103/µL; CRP: 0.21 mg/dL; TnI: 0.01 ng/L; faecal calprotectin: 3213 mg/kg) and the patient was discharged. One month later (September 2018), a colonoscopy revealed a sub-acute ulcerative pancolitis with Mayo score 1.5 22–24 In December 2018, a follow-up cardiac MRI documented the resolution of myocarditis (figure 1B), and the echocardiography revealed the normalisation of the ventricular ejection fraction (68%).
{kind=link}
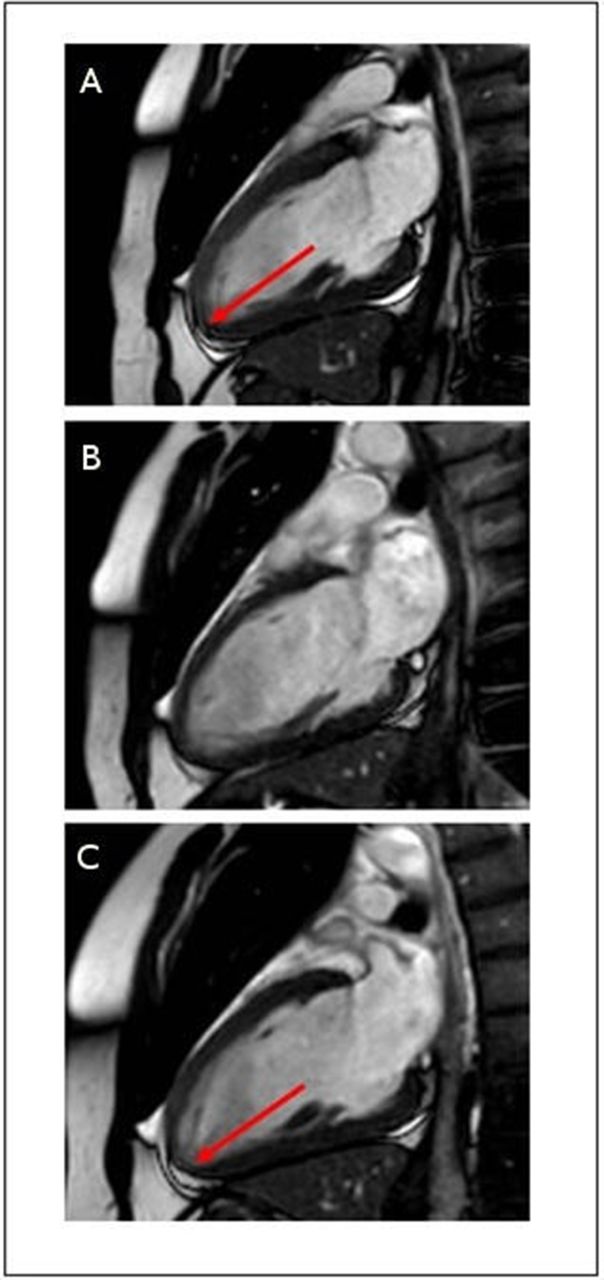
(A) Cardiac MRI showing myocardial oedema of the apical anterior and septal site compatible with myocarditis (red arrow); (B) the oedema previously reported in the left ventricle was no longer detectable. Some interstitium/myocellular abnormalities, compatible with myocarditis, are present in the apical lateral site; (C) picture illustrating a small and nuanced area of oedema in the apical lateral site with subepicardial localisation (red arrow), compatible with a recent inflammation.
In July 2019, due to a new exacerbation (acute proctosigmoiditis; Mayo 3) AZA treatment was discontinued, and vedolizumab was started (300 mg intravenous every 8 weeks). A month later (August 2019), the patient was re-hospitalised because of the occurrence of symptom relapse characterised by bloody diarrhoea, tachycardia and chest pain with an increase of high-sensitive TnI (358 ng/L) without ECG abnormalities. The patient was investigated for the third time with a cardiac MRI showing a new inflammatory lesion suggestive of myocarditis (figure 1C). A second diagnosis of myocarditis was established, certainly unrelated to MSZ since this drug was discontinued 1 year before. During the hospitalisation the patient was treated with intravenous methylprednisolone 1 mg/kg/day for 7 days associated with vedolizumab. Intestinal symptoms improved along with a reduction of the inflammatory markers: WBC from 15.19 to 9.36 x 103/µL; CRP from 3.21 to 0.83 mg/dL; TnI from 358 to 27 ng/L. At discharge, the treatment regimen included intravenous vedolizumab 300 mg every 8 weeks, methylprednisolone 32 mg/day (tapered down until complete discontinuation), topical beclometasone 3 mg/day, bisoprolol 2.5 mg/day and ramipril 5 mg/day. A follow-up endoscopy (January 2020) showed ulcerative proctosigmoiditis with mild endoscopic activity, Mayo score 1. The patient is currently well and follows a therapy with intravenous vedolizumab 300 mg every 8 weeks, bisoprolol 2.5 mg and ramipril 5 mg, both on a daily basis.
Discussion
UC is often accompanied by extra-intestinal manifestations as anaemia, arthropathy, metabolic bone abnormalities, cutaneous diseases (erythema nodosum and pyoderma gangrenosum), ocular (episcleritis and uveitis), hepatobiliary diseases (primary sclerosing cholangitis, pericholangitis, steatosis, chronic hepatitis, cirrhosis and gallstone formation), and less commonly, cardiovascular complications.25 However, cardiac manifestations can occur with a higher frequency than what it is clinically documented, as they may remain undiagnosed.7 Up to one-third of patients with IBD, particularly those with UC,7 can develop myocarditis or pericarditis with a higher rate of complications, and fatal outcomes in comparison with patients affected by Crohn’s disease.26 Therefore, despite myocarditis has been considered a rare extra-intestinal manifestation of UC, this condition has been documented in many literature reports.1 27–29 Cardiac manifestations in UC may be overlooked because of non-specific symptoms (eg, fatigue, dyspnoea and chest pain), which either resolve without any specific treatment or rapidly progress up to more severe heart complications, for example, cardiogenic shock.30
MSZ is a 5-aminosalicylic acid agent usually prescribed as a first-line therapy in the treatment of UC.31 MSZ mechanism of action has not been completely understood. However, it is thought that it reduces inflammation by inhibiting the cyclooxygenase enzyme and the peroxisome proliferator-activated receptor gamma cascade, thus reducing the proinflammatory signalling pathway of the nuclear factor κB.10 12 Along with the most common MSZ-evoked side effects (eg, dyspepsia, pancreatitis, blood dyscrasias, nausea and headache), this drug can trigger the onset of cardiac inflammation, such as pericarditis, myocarditis and coronary vasculitis.9 The mechanisms leading to cardiotoxicity have not been elucidated yet; however, different theories have been proposed: (1) MSZ may increase the eosinophil-stimulating cytokines, promoting a hypersensitivity reaction; (2) a hypersensitivity reaction triggered by antibodies directed against the drug and a cross-reacting with the cardiac tissue; (3) an immunoglobulin E-mediated allergic reaction promoted by its toxicity on the myopericardium.12 MSZ induced myocarditis usually appears within 4 weeks from the beginning of the treatment, but concomitant corticosteroid use could delay the onset of the cardiotoxicity. MSZ-induced myocarditis has been reported in literature both in the treatment of UC,8–16 Crohn’s disease17–19 and in newly diagnosed IBD.21 Up to now, more than 51 cases of MSZ induced myocarditis have been reported.32
The Food and Drug Administration has approved tumour necrosis factor-alpha (TNF-α) blockers (such as infliximab, adalimumab and golimumab) for the treatment of UC, and the use of these drugs has been associated with worsening of congestive heart failure.20 Namely, cardiomyopathy has been reported as a severe adverse reaction of adalimumab,33 34 myocarditis and perimyocarditis have been ascribed to infliximab,35–37 and heart failure onset or worsening has been specified on the safety information of golimumab as new onset or worsening of congestive heart failure have been reported with this compound.38 Although a cardiac death has been reported in a 66-year-old male 14 days after the first induction dose of vedolizumab (an integrin receptor antagonist currently used to treat UC), it should be emphasised that this patient had a 2-year history of chronic ischaemic heart disease,39 making unlikely that this drug exerted a toxic effect. In this line, the safety of vedolizumab has been well documented both in naive or in patients previously treated with anti-TNF-α agent,40–43 and in studies with a long-term follow-up (up to 5 years).40 44–47
Based on the data emerged by our case report, the first episode of myocarditis could be attributable to MSZ therapy even though it is not possible to rule out a previously misdiagnosed extra-intestinal manifestation of UC perhaps triggered by MSZ. On the other hand, the second episode was likely an extraintestinal manifestation of UC, since vedolizumab treatment was not discontinued at time of the diagnosis of myocarditis, which progressively resolved with corticosteroid use and never relapsed.
This case reports a patient with recurrent extensive UC flares. On two independent situations separated by a period of more than 1 year, he presented with severe chest pain, elevated TnI levels and MRI changes typical of myocarditis. Treatment with steroids led to rapid resolution. The first episode appeared during a severe pancolitis exacerbation that was initially treated with MSZ. Because myocarditis has been attributed to MSZ, its use was terminated. Moreover, even the second episode of myocarditis occurred during a disease flare when endoscopic changes were severe and extensive. Complete resolution of cardiac and colonic findings with steroids suggested that immune factors played a role in both recurrent disorders. On the other hand, myocarditis could also occur during acute intestinal diseases due to increased intestinal permeability.48 This is the case of enteroviral infections, in which products of the enteroviral genome (eg, viral protease 2A) can spread systemically through the leaky gut and cleave host proteins, like dystrophin, causing cardiac dysfunction.48 49 Further studies to elucidate molecular mechanisms associated with these clinical phenomena are needed. We could speculate that even the very first episode of myocarditis was not drug related since the toxicity usually appears within 4 months from MSZ starting and the patient was at the twelfth month of therapy. From this point of view, the hypothesis of an extraintestinal manifestation related to disease flare and increased intestinal permeability is suggestive but cannot be proved.
Finally, it is worth noting that, regardless the aetiology of myocarditis in patients affected by UC, a timely diagnosis of cardiac complication is crucial to avoid life-threatening complications often aggravated by fatal outcome.29
Acknowledgments
We would like to acknowledge the Registered Nurse, Dr. Daniela Mazzoni, for her technical help.
References
Footnotes
GC and LL are joint first authors.
Contributors GC, LL and FC: drafting the manuscript, literature review and critical revision of the final manuscript. GC, GZ and RDG: conceptualisation and critical revision of the final manuscript. EZ, MM, MCM and UV: involved in patient care and critical revision of the final manuscript. All authors approved the final version of the article and are accountable for its content. RDG and GZ share last authorship.
Funding GC, GZ and RDG are supported by research (F.A.R.) funds from University of Ferrara.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.