Article Text

Abstract
We present a case of haemorrhagic enterocolitis in a patient with SARS-CoV-2 who recovered from respiratory failure after support with venovenous extracorporeal membrane oxygenation. We describe clinicopathological features consistent with the systemic coinfection/reactivation of cytomegalovirus (CMV) concurrent with COVID-19 infection and the protracted clinical course of resolution of gastrointestinal inflammation after the treatment of CMV infection. Stool PCR, abdominal CT perfusion scan and histological examination of ileal and colonic tissues excluded enterocolitis secondary to other causes of infection (common viral, bacterial and protozoal gastrointestinal pathogens), macrovascular and microvascular ischaemia and classic inflammatory bowel disease, respectively. We propose possible synergistic pathophysiologic mechanisms for enterocolitis complicating severe COVID-19 infection: (1) T lymphocyte depletion and immune response dysregulation, (2) use of immunomodulators in the management of severe COVID-19 infection and (3) high concentration of ACE-2 receptors for COVID-19 virus in the gastrointestinal tract.
- enteric infections
- gut inflammation
- histopathology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The SARS-CoV-2 virus, also known as COVID-19, was first discovered in the Wuhan province of the People’s Republic of China on 31 December 2019 after a media statement describing a ‘viral pneumonia’.1 This novel coronavirus, SARS-CoV-2, rapidly spread around the globe in the ensuing months. On 13 January 2020, there was a case of COVID-19 reported in Thailand, the first documented case outside of the Wuhan province of the People’s Republic of China.2 As of the most recent WHO situation report (21 December 2020), there were 75 704 857 confirmed cases of COVID-19 with 1 690 061 confirmed deaths.3
We present a case of persistent diarrhoea and haematochezia in a patient with severe acute respiratory syndrome secondary to SARS-CoV-2 who recovered from respiratory failure after support with venovenous extracorporeal membrane oxygenation. We describe clinicopathological features consistent with the systemic coinfection/reactivation of cytomegalovirus (CMV) concurrent with COVID-19 infection and related haemorrhagic enterocolitis and the protracted clinical course for the resolution of gastrointestinal inflammation after the treatment of CMV infection.
The case
A middle-aged woman with no medical history presented as a transfer from an outside hospital to Mayo Clinic Arizona for venovenous extracorporeal membranous oxygenation (ECMO) due to refractory hypoxaemia on day 0 (9 May 2020). On arrival to the outside hospital, patient had endorsed 10 days of worsening fever, dyspnoea, cough, fatigue, malaise and diarrhoea. Both of her parents and her sister were also positive for COVID-19. Both parents died from COVID-19.
On arrival, the patient was severely hypoxaemic, requiring 100% oxygen on invasive mechanical ventilation. CT scan of chest demonstrated diffuse ground glass opacities, along with posterior consolidation and consistent with severe viral pneumonia and acute respiratory distress syndrome (not shown). Laboratory studies confirmed severe COVID-19 illness with elevated troponin-T, lymphocytopenia and markedly elevated d-dimer, C reactive protein and lactate dehydrogenase. The patient was treated with remdesivir, 200 mg on day 1, followed by 100 mg daily for 5 days, two units of SARS-CoV-2 convalescent plasma and systemic hydrocortisone 200 mg/day. Plasma interleukin (IL)-6 was 14.1 on admission, and subsequently increased to >400 pg/mL on day 2. The patient was given two doses of IL-6 antagonist tocilizumab (a total of 8 mg/kg). Venovenous ECMO was initiated on day 4 through cannulation of bilateral common femoral veins for drainage and return of oxygenated blood and systemic anticoagulation was maintained with bivalirudin.
On day 10, the patient developed rectal bleeding that was initially attributed to insertion of a faecal management device and systemic anticoagulation. On day 13, CT perfusion scan of the abdomen and pelvis with intravenous contrast demonstrated thickening and marked mural oedema of the distal jejunum, ileum and colon and all mesenteric arteries and veins were well visualised and patent (figure 1). The initial diagnosis was acute haemorrhagic enterocolitis possibly related to COVID-19 infection because the nasopharyngeal PCR was positive for this virus. On day 20, the patient was successfully weaned from venovenous ECMO support and was continued on invasive mechanical ventilation through tracheostomy. Blood cultures were positive for Enterobacter cloacae and plasma CMV PCR was undetectable at the onset of gastrointestinal symptoms (table 1). On day 26, colonoscopy revealed friable ulcerated bleeding mucosa (figure 2A) and colonic and ileal biopsies demonstrated near complete loss of epithelium and rare CMV infected cells by immunohistochemistry (see online supplemental file). Nasopharyngeal SARS-CoV-2 PCR was negative. Stool PCR testing excluded other common gastrointestinal bacterial, protozoal and viral pathogens causing enterocolitis (Campylobacter, Plesiomonas shigelloides, Salmonella species, Vibrio species, V. cholerae, Yersinia species, Clostridium difficile toxin, Enteroaggregative Escherichia coli, Enteropathogenic E. coli, Enterotoxigenic E. coli, Shiga toxin producing E. coli; Shigella/Enteroinvasive E. coli; Cryptosporidium species, Cyclospora cayetanensis, Entamoeba histolytica, Giardia, Adenovirus, Astrovirus, Norovirus, Rotavirus and Sapovirus). Serology for human immune deficiency, hepatitis B and C viruses were negative.
Supplemental material

Abdomen CT with intravenous contrast. CT scan of the abdomen and pelvis with intravenous contrast demonstrated thickening and marked mural oedema of the distal jejunum, ileum and colon and all mesenteric arteries and veins were well visualised and patent on day 13. Day 0 is the day of admission (9 May 2020).

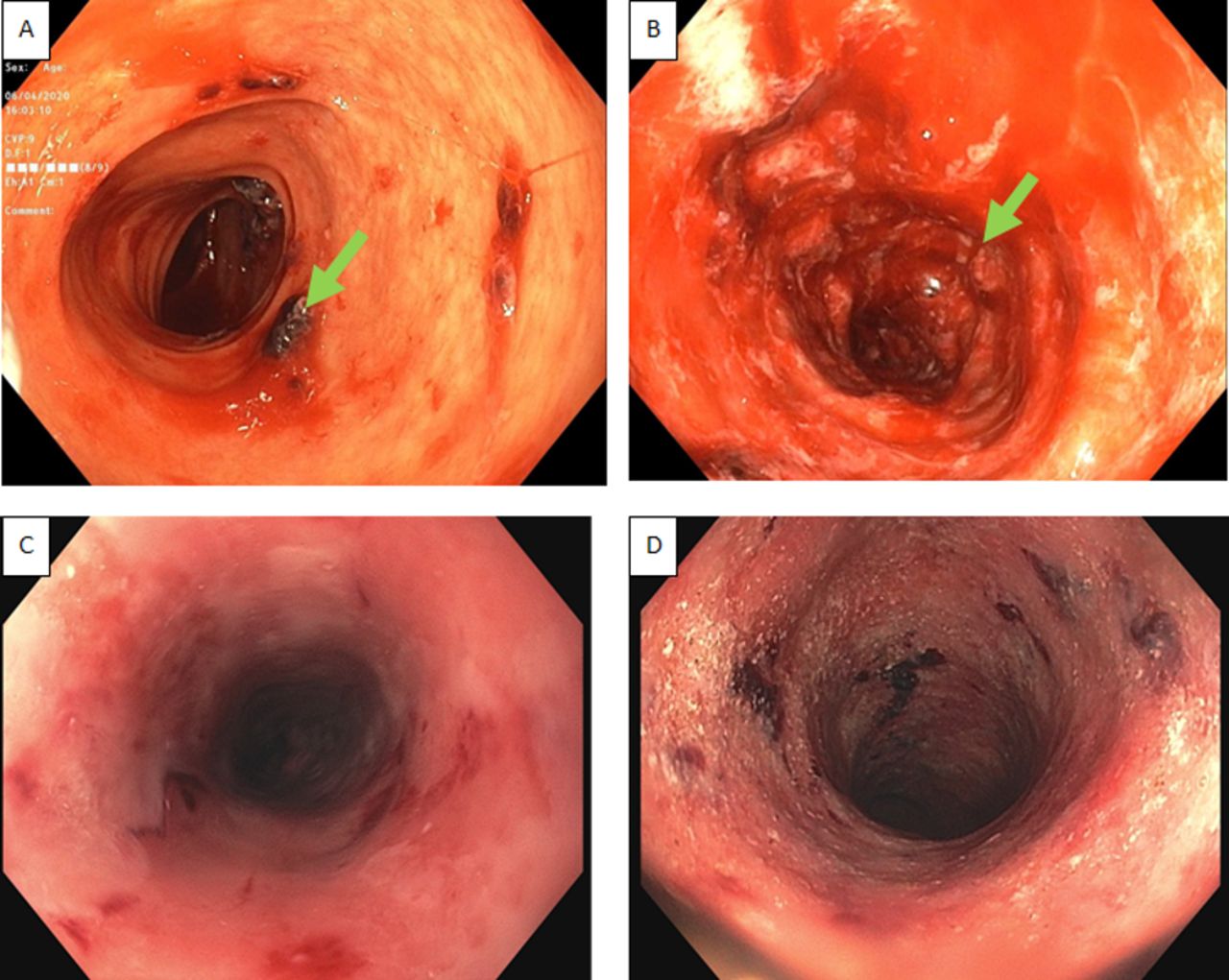
Timeline of colonoscopic imaging of macroscopic appearance of gastrointestinal mucosal injury before and after initiation of treatment of cytomegalovirus haemorrhagic enterocolitis. Serial colonoscopic images illustrate the spectrum of macroscopic appearance of the gastrointestinal tract mucosa injury as seen in the colon. (A) (day 26) and (B) (day 41) indicate interval progression of mucosal injury with ulceration (green arrows) and bleeding before initiation of treatment for cytomegalovirus. (C) (day 107) and (D) (day 122) indicate partial resolution and incomplete healing of the mucosal injury with hyperaemia after the completion of an initial treatment with ganciclovir and then with foscarnet. Day 0 is the admission (9 May 2020).
Quantitative plasma cytomegalovirus DNA
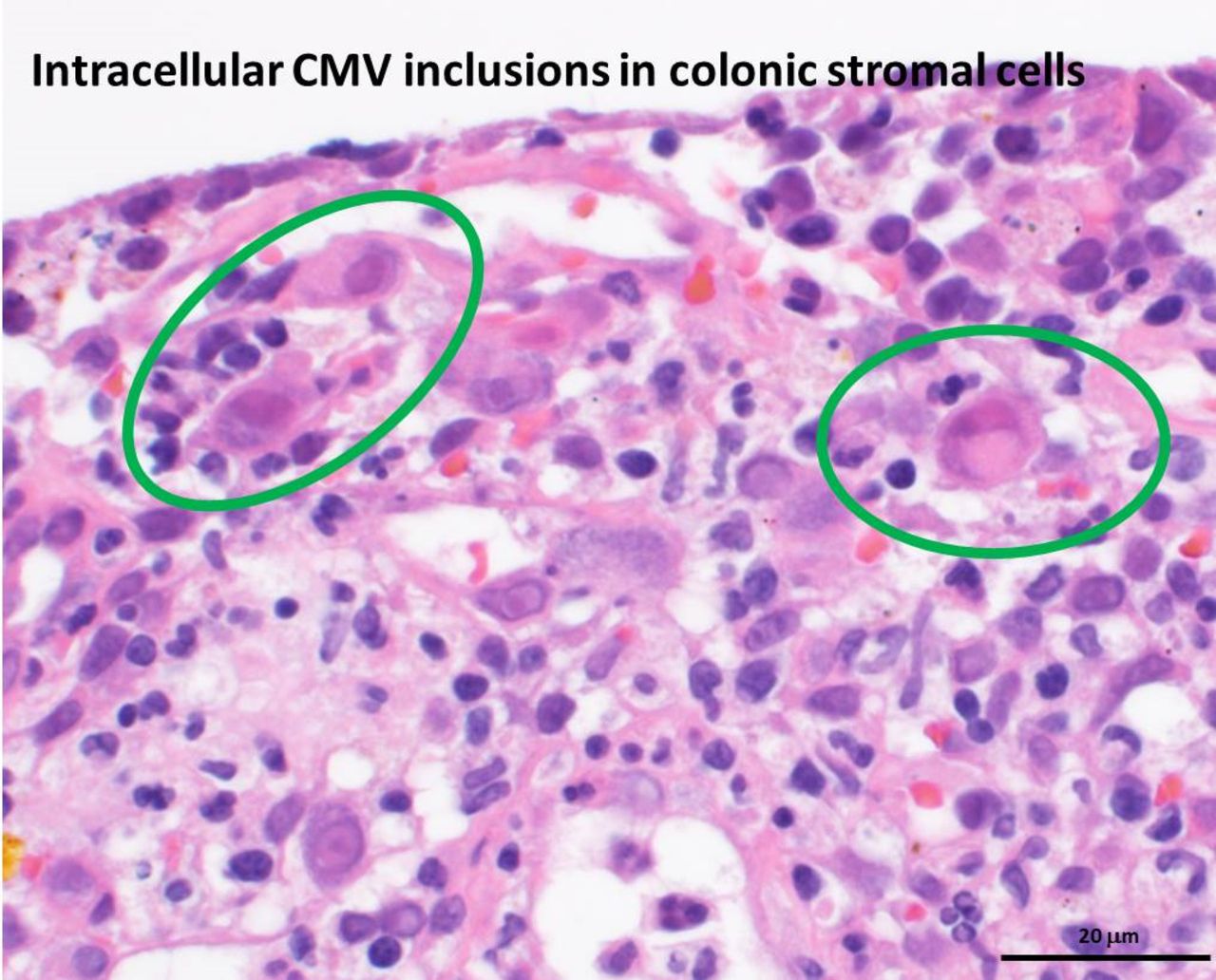
On day 41, colonoscopy was repeated because of persistent haematochezia and high volume diarrhoea and demonstrated worsening of colitis with ulceration and bleeding mucosa through the entire colon into the terminal ileum (figure 2B). Pathology demonstrated numerous intracellular CMV inclusion bodies readily identifiable on routine stains (figure 3). Repeat plasma CMV DNA viral load was significantly elevated at 9900 IU/mL (table 1). Ganciclovir was started because of worsening enterocolitis and CMV viraemia with subsequent decrease in CMV viraemia and partial resolution of symptoms (table 1). The patient was liberated from mechanical ventilation successfully on day 72. Total parental nutrition was continued because of persistent high output (approximately 2 L/day) diarrhoea and haematochezia after completion of treatment with ganciclovir on day 81. On day 91, foscarnet was started because of persistent symptoms and concern for ganciclovir-resistant CMV (table 1). On day 107, colonoscopy (figure 2C) and biopsy indicated residual CMV enterocolitis, but partial re-epithelisation was noted (see online supplemental file). On day 108, immunophenotyping of plasma lymphocytes indicated relative depletion of certain cellular subsets: CD45 total lymph count 0.71 (reference range 0.82–2.84 thou/μL), CD3 (T Cells) 509 (reference range 550–2202 cells/μL), CD4 (T Cells) 368 cells/μL (reference range: 365–1437 cells/μL) CD8 (T Cells) 147 (reference range 145–846 cells/μL). Colonoscopic biopsy demonstrated rare residual CMV-positive cells by immunohistochemistry; persistent terminal ileum and colonic loss of epithelium with slight improvement in epithelial regeneration on day 122 (figure 2D and online supplemental file). Plasma CMV PCR was undetected from day 129. Foscarnet was discontinued on day 136 and ganciclovir was restarted as CMV prophylaxis after viral drug-resistance was excluded. Stool calprotectin, a cellular protein released from inflammatory neutrophils in the gastrointestinal tract, were elevated on days 18 and 180 (470, 556 with normal range ≤50.0 μg/g, respectively) indicating persistent gastrointestinal inflammation. In addition to systemic corticosteroids, 390 mg of Ustekinumab was administered intravenously on days 137, 166 and 180 as a therapeutic trial. Ustekinumab has been used for treating severe active inflammatory bowel disease and its mechanism of action is through the inhibition of IL-12 and IL-23 and of dysregulated immune response in the gastrointestinal tract.4 On days 150 and 180, the histopathological features of colonic tissue biopsies were unchanged from the previous findings of incomplete re-epithelialisation with granulation tissues and no viral cytopathic features as well as negative immunohistochemical stains for adenovirus, CMV and herpes simplex virus 1 and 2 (not shown). After receiving an additional dose of ustekinumab on day 209, the patient was discharged to an inpatient skilled nursing facility on total parental nutritional support and supplemental enteral nutrition through percutaneous gastrostomy tube. Over the last 30 days before hospital discharge, the daily frequency of continent and incontinent liquid stool output decreased from as high as 20 to 4 with occasional mucus and blood.
{kind=link}
{kind=link}
{kind=link}
Colonic biopsy with intracellular cytomegalovirus inclusions. Colonic biopsy from colonoscopy performed on day 41 demonstrating numerous stromal cells containing CMV inclusions (circles) in patient with severe COVID-19 respiratory distress syndrome and haemorrhagic enterocolitis. Day 0 is the day of admission (9 May 2020). (H&E stain, ×400 magnification). CMV, cytomegalovirus.
Discussion
This case of severe CMV enterocolitis was treated initially with ganciclovir and then Foscarnet with improvement of CMV viraemia but persistent haemorrhagical enterocolitis with extensive intestinal epithelial injury confirmed by histological evaluation. Stool PCR, abdominal CT perfusion scan and histological examination of ileal and colonic tissues excluded enterocolitis secondary to other causes of infection (common viral, bacterial and protozoal gastrointestinal pathogens), macrovascular and microvascular ischaemia and classic inflammatory bowel disease, respectively. D’Ardes described a fatal case of recent or likely active coinfection of CMV with SARS-COV-2.5 The diagnosis was based on high titres of CMV IgM and IgG antibodies, without confirmatory plasma CMV PCR or histopathological features. Meta-analysis of 2398 non-COVID-19 immunocompetent critically ill patients demonstrated a 27% CMV infection and 31% reactivation rate.6 To our knowledge, this is the first case of CMV viraemia and tissue invasive enterocolitis in an immunocompetent host with severe COVID-19 infection that was confirmed by both plasma CMV PCR and histopathology. It is also noteworthy that the gastrointestinal inflammation and histopathological abnormalities persisted after recovering from acute viral illness with SARS-COV-2 and treatment of CMV infection. We propose three possible hypotheses for the pathogenesis of CMV viraemia and persistent enterocolitis in this case of severe COVID-19 disease.
Our first hypothesis is severe lymphocytopenia likely led to impaired cellular immunity, which may have precipitated CMV coinfection/reactivation. Lymphocytopenia is common in more severe cases of COVID-19, and persists until death.7 This is thought to potentially be related to COVID-19 infection and subsequent apoptosis of T lymphocytes with resultant dysfunction of reticuloendothelial and haematological organs, for example, bone marrow, spleen, lymph nodes.8 9 Depletion and exhaustion of functional T cells and CD8 +T cells has been correlated with disease severity in COVID-19, along with possibly lowering host innate and adaptive immune defence against other viral infections.8 10 11 Additionally, the production of proinflammatory cytokines and T lymphocyte sequestration in tissues can contribute to transient loss of circulating CD4+ and CD8+T lymphocytes and cellular immunosuppression.11 12 This may result in reactivation of herpes simplex virus and CMV in severe COVID-19 disease.13 Immunophenotyping of plasma lymphocytes in this case confirmed the depletion of subset of T-lymphocytes necessary for adaptive immune response to viral infection. In addition to dysfunction of T-lymphocytes and of cell-mediated immune response to viral infection, other researchers have also indicated that concurrent excessive activation of B-lymphocytes and production of SARS-CoV-2 neutralising antibodies may be associated with an additional tissue injury similar to settings in autoimmune disorders.14 Dysregulated response of B-lymphocytes and production of autoantibodies would exacerbate tissue injury in severe COVID-19 infection. Immunophenotyping of B-lymphocytes and native antibody production in this patient may help to elucidate if an aberrant humoral immune response could have potentiated the gastrointestinal tract injury and delayed the resolution of enterocolitis.
A second hypothesis is that the administration of immunomodulators, such tocilizumab in this case, may have increased the risk of coinfection with other pathogens. The patient in this case developed Enterobacter cloacae bacteraemia during the critical illness. Immunomodulators can mitigate the biological and pathological manifestations of haemophagocytosis secondary to cytokine release syndrome,15 both of which have been postulated to contribute to severe COVID-19 disease. IL-6 is released by a wide variety of cells, including B and T lymphocytes, macrophages, dendritic cells, fibroblasts and endothelial cells. Functional IL-6 deficiency has been associated with worse lung damage in H1N1 influenza.16 Additionally, IL-6 antagonism has also been associated with increased risk of other infections in COVID-19 patients.17–19 Systemically administered hydrocortisone is also an immunomodulator and can interfere with host innate and adaptive immune response to pathogens.20
A third hypothesis is that the ACE-2 receptor for SARS-CoV-2 entry into the cells is found in high concentrations in certain organs such as the vascular endothelium, lungs, cardiovascular system, kidneys, liver and gastrointestinal tract and therefore increasing the vulnerability of these target organs to viral cytopathic effects.9 21 22 SARS-CoV-2 can infect the gastrointestinal tract epithelium and the splanchnic vasculature endothelium. Gastric hypomotility, intestinal paralytic ileus, colonic pseudo-obstruction, ischaemia and necrosis of the small intestine and colon have been reported in patients with severe COVID-19 infection and was associated with an overall mortality of 14% and was as high as 40% in the subset of patients who developed bowel ischaemia and necrosis secondary to microvasculature thrombosis.23 In this patient, ischaemic bowel injury was unlikely because: (1) the patient was systemically anticoagulation during venovenous ECMO support, (2) the abdominal CT perfusion imaging excluded macrovascular thrombosis of the visceral vasculature and (3) the histopathological findings did not suggest microvascular thrombosis that would be consistent with COVID-19 induced microangiopathy. It is noteworthy that at the onset of haemorrhagic enterocolitis, quantitative plasma CMV DNA titre was extremely low and therefore implying that the gastrointestinal tract injury may have been initiated by COVID-19 viral infection of the gut epithelium. Histological examination of ileal and colonic tissues demonstrated delayed gastrointestinal re-epithelialisation in the small intestine and colon after CMV treatment and coincided with symptomatic high volume diarrhoea and haematochezia in this patient. It is unclear if persistent inflammation because of viral cytopathic effect and/or dysregulated immune response to SARS-COV-2 in the gastrointestinal tract may have adversely impeded re-epithelisation of the gastrointestinal tract and patient recovery after treatment of CMV infection. Unlike this patient, other case report of COVID-19 associated enterocolitis had self-limited illness and recovered primarily with supportive care without long-term gastrointestinal consequences.24 It is important to note that gastrointestinal symptoms have also been reported in association with past SARS-CoV-2 infection (SARS-CoV-2 positive serology and negative PCR) and characterised by acute systemic inflammation, one or more extrapulmonary organ system dysfunction and arterial/venous thromboembolism known as ‘adult multisystem inflammatory syndrome’.25 However, in this reported case, the gastrointestinal symptoms were unlikely to be manifestations of multisystem inflammatory syndrome when the patient became SARS-CoV-2 PCR negative because other classic characteristic features of this syndrome were not present in this patient.
Conclusion
The SARS-CoV-2 virus has the ability to affect multiple organ systems outside of the lungs, including the gastrointestinal tract. The optimal treatment and management of the short and long-term gastrointestinal complications related to COVID-19 disease is still being developed to date. Here, we presented a case of CMV and SARS-CoV-2 coinfection that manifested with haemorrhagical enterocolitis with persistent gastrointestinal inflammation after CMV treatment. This complication may have developed because of several synergistic pathophysiologic mechanisms related to severe COVID-19 infection: (1) T lymphocyte depletion and immune response dysregulation, (2) use of immunomodulators IL-6 inhibition and corticosteroids in the management of severe COVID-19 infection and (3) high concentration of ACE-2 receptors for COVD-19 virus in the gastrointestinal tract.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it published online to fix a spacing issue in abstract.
Contributors WCC participated in the concept or design of the work; or acquisition, analysis or interpretation of data; drafting the work or revising it critically for important intellectual content; approval of the version to be published and participated sufficiently in the work to take public responsibility for appropriate portions of the content. MYR participated in the concept or design of the work; or acquisition, analysis or interpretation of data; drafting the work or revising it critically for important intellectual content; approval of the version to be published and participated sufficiently in the work to take public responsibility for appropriate portions of the content. MAS participated in the concept or design of the work; or acquisition, analysis or interpretation of data; drafting the work or revising it critically for important intellectual content; approval of the version to be published and participated sufficiently in the work to take public responsibility for appropriate portions of the content. BP participated in the concept or design of the work; or acquisition, analysis or interpretation of data; drafting the work or revising it critically for important intellectual content; approval of the version to be published and participated sufficiently in the work to take public responsibility for appropriate portions of the content. VPS participated in the concept or design of the work; or acquisition, analysis or interpretation of data; drafting the work or revising it critically for important intellectual content; approval of the version to be published and participated sufficiently in the work to take public responsibility for appropriate portions of the content. AS participated in the concept or design of the work; or acquisition, analysis or interpretation of data; drafting the work or revising it critically for important intellectual content; approval of the version to be published and participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval Our Institutional Review Board does not require approval for reporting individual case or case series.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.