Article Text

Abstract
Objective COVID-19 has disrupted the normal way of life in the UK, but for some patients with inflammatory bowel disease (IBD), the impact of this unprecedented global emergency was far greater. We aimed to assess the experience of patients with IBD during the COVID-19 lockdown.
Design We designed a survey focused on the impact of COVID-19 on IBD healthcare, social and psychological well-being and quality of life. To capture those most likely to be affected we targeted survey invitations at our British Society of Gastroenterology (BSG) defined high and moderate-risk IBD population. Access to the survey was also available via our trust’s social media pages.
Results 685 responses were received. 76% of respondents categorised themselves in BSG defined moderate or high-risk groups, requiring stringent social distancing or shielding. 87% did not change their IBD medication, with most reported changes initiated by the IBD team. 39% were worried about their IBD care, but most services were largely uninterrupted. 90% received ‘at-risk’ notification often from multiple sources, but 17% not until May. The majority reported a negative impact of COVID-19 on their quality of life and significantly increased perceived stress. Patients expressed a strong wish of having future care delivered remotely.
Conclusion COVID-19 has had a significant negative impact on psychological well-being of patients with IBD. Local IBD services must have a robust data set of vulnerable patients and be designated future responsibility for prompt communication of advice to avoid delayed and sometimes conflicting information. Remote patient management systems should be further developed and embedded in clinical practice.
- inflammatory bowel disease
- crohn's disease
- ulcerative colitis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
COVID-19 had a significant impact on inflammatory bowel disease (IBD) services, but effects on care and well-being as perceived by patients with IBD are unknown.
What are the new findings?
While many patients were concerned about the effect of COVID-19 on their IBD care, few reported services being affected; the effect of COVID-19 on psychological well-being, however, was profound.
Information regarding social distancing and shielding was often delayed, received from multiple sources and sometimes conflicting.
There is a preference for future care to be delivered remotely, even during IBD flares.
How might it impact on clinical practice in the foreseeable future?
It is essential for IBD services to hold accurate and accessible databases of their patient population and have timely methods of contacting them when required.
Systems for remote patient management should be further developed and embedded in clinical services to facilitate remote patient care and monitoring.
Introduction
SARS-CoV-2 has been identified as the causative pathogen in the ongoing global coronavirus (COVID-19) pandemic which started in Wuhan, China in December 2019.1 2 Due to rising infection numbers the British government introduced the concept of shielding on 22 March 2020 and announced measures to protect clinically vulnerable patients, including those on immunosuppressants.3 More specific guidance for the inflammatory bowel disease (IBD) population was published the same day by a British Society of Gastroenterology (BSG) working group and publicised through the national Crohn’s and Colitis UK (CCUK) charity.4 Patients were asked to follow strict social distancing or shielding if in moderate or high-risk groups, respectively. This risk stratification relied on extrapolated data and expert opinion due to a lack of available clinical evidence of the risks of COVID-19 infection in patients with IBD at that time. IBD-specific factors including active disease, combined immunosuppression and corticosteroid therapy together with other comorbidities such as age, high BMI, diabetes, hypertension, cardiac and respiratory disease have been identified as potential risk factors for a poor outcome in COVID-19 infection.4 There, however, remains a lack of robust data on the impact of COVID-19 infection on patients with IBD and in particular those who are immunosuppressed. Ongoing studies, including the Surveillance Epidemiology of Coronavirus Under Research Exclusion (SECURE-IBD) and Physician Responses to Disease Flares and Patient Adaptation in Relation to Events in Inflammatory Bowel Disease During COVID-19 Pandemic (PREPARE-IBD).
Physician Responses to Disease Flares and Patient Adaptation in Relation to Events in Inflammatory Bowel Disease During COVID-19 Pandemic (PREPARE IBD)
Patients with IBD were left in an uncertain position and had to quickly adapt to a rapidly changing environment in relation to their illness and medication. The economic and social disruption of the COVID-19 pandemic severely impacted lives of many patients with IBD with added uncertainty regarding healthcare delivery, employment, education and housing with an unknown effect on their psychological well-being and quality of life. The aim of this study was to understand the experience of lockdown, social distancing and shielding of patients with IBD at University Hospital Southampton (UHS) to help the IBD team deliver better care in the event of a second wave.
Methods
We conducted an online single point in time survey collecting anonymised data including demographic details, IBD medication, COVID-19 risk factors and symptoms as well as the psychological and socioeconomic impact of the COVID-19 lockdown period. The survey was distributed electronically to all patients with IBD registered on our online patient portal My Medical Record, by post to all patients with IBD who received ‘at-risk’ letters from UHS and also via the UHS social media pages. Patients who were non-IT users were able to complete paper copies of the survey. In-patients under the IBD team or patients attending for biological infusions or outpatient appointments were also asked to complete the survey. Approximately 2700 patients with IBD were contacted. It was not mandatory to complete all survey questions and percentages were calculated from the number of responses to each individual question. Self-rated, subjective level of stress was assessed using a visual 10 point analogue score, adapted from the subjective units of distress scale.5 Statistical analysis was performed using R V.4.0.
Results
Demographics
A total of 685 patients responded to the survey with 98% of responses received online through our in-house survey tool ‘gather’ and only 2% via a paper survey. A total of 443 had a diagnosis of Crohn’s disease, 211 ulcerative colitis and 31 IBD-undifferentiated. 57.5% of respondents were female. Age distribution, disease duration and ethnicity were representative for our local IBD population with predominantly white British patients with IBD with only 3.0% from ethnic minorities. The most common comorbidity was anxiety or depression, self-reported by 14.9% of patients. Other commonly reported comorbidities included hypertension (12.8%), diabetes (3.6%), cardiac disease (3.1%) and morbid obesity with body mass index >40 (2.2%). See table 1 for demographics and online supplemental table 1 for full demographic breakdown and comorbidity list.
Supplemental material
IBD medication prior to March 2020 and the start of lockdown was recorded. 71.5% (490/685) were either on immunomodulators or biological medication. 26.3% (180/685) were on immunomodulator monotherapy, 28.5% (195/685) biological/small molecule monotherapy and 16.8% (115/685) on dual immunosuppression. Steroid use was limited in our population with 6.0% (41/685) receiving either oral prednisolone or budesonide.
Demographics of survey respondents
IBD management during COVID-19
During the lockdown period, 87.0% (596/685) of patients reported their medication had remained unchanged. For those stopping medication, the majority of these decisions were taken on the advice of the IBD team (77/104 medication changes). Oral steroids were the most commonly discontinued medications with 41% (12/29) stopping prednisolone and 50% (6/12) stopping budesonide. Immunomodulators were stopped in 11.2% (33/294) with 12/33 patients choosing to stop themselves. Biological treatments were continued in 90% (279/310) of patients; 15/31 switched agents, 13 were stopped by the IBD team and 3 patients chose to discontinue their biological medication themselves.
New medication was started in 6.2% (43/685) of patients during the lockdown period. With the exception of oral prednisolone and mesalazine, the majority of these decisions were via the IBD team. Oral prednisolone was started in 9/48 patients with 4 of these prescriptions originating in primary care and with 1/9 patients self-medicating. Three patients started oral budesonide all initiated by the IBD team. Mesalazine was started in 6/48 patients and immunomodulators in 4/48. Including the 15 patients who switched agents, there were 22 new biological prescriptions. Ustekinumab was the most common biologic started accounting for 50% (11/22) of the new biologics.
A total of 323/685 patients reported contacting the IBD team during the COVID-19 period for one or more reasons. A total of 110/323 reported requiring information about COVID-19. A total of 132/323 had medication queries, 110 contacted to discuss symptoms of a flare, 57 investigations and 48 results. 45.4% of contacts were made via the IBD telephone helpline, 34.9% via our online My Medical Record patient portal, 16.0% via secretaries and 3.7% either via their general practitioner (GP) or in writing. 43.9% (301/685) of patients reported actively trying to avoid coming to hospital.
Thirty-seven per cent (251/685) reported having a flare of IBD symptoms between March and August 2020. In addition to the 110 contacting the IBD helpline, 121 reported self-managing their symptoms without contacting either their GP or the IBD helpline. Twelve contacted their GP only, 15 contacted both the IBD team and their GP and 8 patients presented to the emergency department.
Patients were asked which aspects of their care had been affected by the pandemic. As expected, there was less clinical activity but overall this affected only small numbers of patients. Most affected were outpatient clinics, which were cancelled for 19% (n=127) and delayed for 16% (n=107). This mainly affected IBD registrar and IBD nurse clinics due to the redeployment of staff. Blood tests were the second most frequently affected hospital service with 22.4% (143) reporting delay or cancellation. Few patients reported disruption with other secondary care services including endoscopy. Home delivery of biologics and the biologics infusion service continued almost uninterrupted. The picture in primary care was similar with appointments, followed by blood monitoring most affected (table 2). Patients made the decision to delay blood test monitoring in over half of cases, while other appointments were delayed by the service provider.
Patients reporting affected services
Comorbidity and shielding
From the data entered on comorbidities, age and medication we identified 115/685 low-risk, 473/685 medium-risk and 97/685 high-risk patients. When asked whether they considered themselves in an at-risk category, 655 responded with 76.3% (500/655) placing themselves in an at-risk category. This included 51 patients who on the data provided were not assigned to be at risk, however, there may have been additional factors not captured to explain this. 23.7% (155/655) considered themselves not to be at risk, including 88/155 who we calculated to be at moderate risk and 9/155 who we calculated to be at high risk as per the BSG risk grid.
Following the introduction of measures to protect vulnerable patients 89.9% (616/685) indicated that they received notification they were in an at-risk group. All 97 patients we calculated to be in the highest risk group received notification and 93.0% (440/473) calculated to be in the moderate risk group. The majority of patients received these notifications by letter (601/616) with a smaller proportion (242/616) receiving a text message and a few by phone (97/616) or email (52/616). There was, however, a delay in patients receiving notification with only 36.3% (224/616) being notified in March. 45.7% (282/616) received their notification in April, but 17.3% (107/616) did not receive theirs until May or June, some 2–3 months after shielding started.
Most patients received more than one at risk notification with 88.9% (548/616) receiving at least 2% and 43.3% (267/616) at least four but in some cases up to eight notifications. Notifications were received from a variety of sources including the government (61.5%, 379/616) or local IBD team (73.4%, 452/616) or GP surgery (28.2%, 174/616). The majority (81.1%, 500/616) reported the information they received on shielding was clear and easy to follow, but 6.7% (41/616) report they found the information unclear. If further information was needed this was obtained from a variety of sources with government websites, CCUK and mainstream media being the most commonly accessed sources. The most helpful additional information was found via the local IBD team, or the CCUK or government websites with 75.1% and 79.2% and 69.0%, respectively, reporting they found the information from these sources useful. Mainstream media, social media and internet chat forums were reported as less helpful with only 34.4%, 24.2% and 30.7% respectfully reporting these as useful (see online supplemental figure 1).
Supplemental material
A total of 629 respondents answered a question about barriers to enhanced social distancing or shielding. 17.2% (108/629) reported they were not required to shield and 61.7% (388/629) reported no barriers to shielding or enhanced social distancing and 3.5% (22/629) reported that they chose not to follow the advice given. The remaining 17.6% (111/629) patients reported one or more barriers. Forty-one listed their housing situation, 66 listed dependents and 24 listed financial reasons.
Patient-reported COVID-19 symptoms
9.6% (66) reported symptoms commonly associated with COVID-19 infection such as fever, persistent cough and loss of sense of smell. A further 5.4% (37) reported symptoms in members of their household. Of those with symptoms; 3 tested positive for COVID-19, 17 tested negative, 41 were unable to get a test and 4 reported not wanting to be tested. Three patients were admitted to hospital with symptoms relating to COVID-19. Most patients with COVID-19 symptoms continued their IBD medication, with only five patients stopping temporarily and one permanently.
Psychosocial impact
Our patient population with IBD reported a very negative or negative impact of the pandemic on their quality of life in 10.2% (70/685) and 42.8% (293/685), respectively. This is in stark contrast with only 4.0% (28/685) and 12.3% (84/685) citing a very positive or positive influence on their quality of life with the rest of the population describing a neutral impact. Patients aged over 55 years were more likely to report a positive impact on their life (OR 2.3, 95% CI 1.5 to 3.5, p 0.0002) (see table 3 for reported impact on specific areas).
Patient-reported impact of COVID-19 and subsequent restrictions
Mean stress score prelockdown was 4.0 (median 3), increasing significantly to 5.5 (median 6) during lockdown (p=2.2e-16, paired Wilcoxon). There was no significant change post easing of lockdown (mean 5.5, p=0.33, median 5), but a significant increase was seen when asking about concern for a rising infections or ‘second wave’ (mean 7.1, p=2.2e-16, median 8) (see figure 1). A self-reported history of anxiety or depression was correlated with a greater stress score prelockdown (p=0.0005, Fisher’s exact test), during lockdown (p=0.0005), at the time of survey (p=0.002) and concern for second wave (p=0.008).
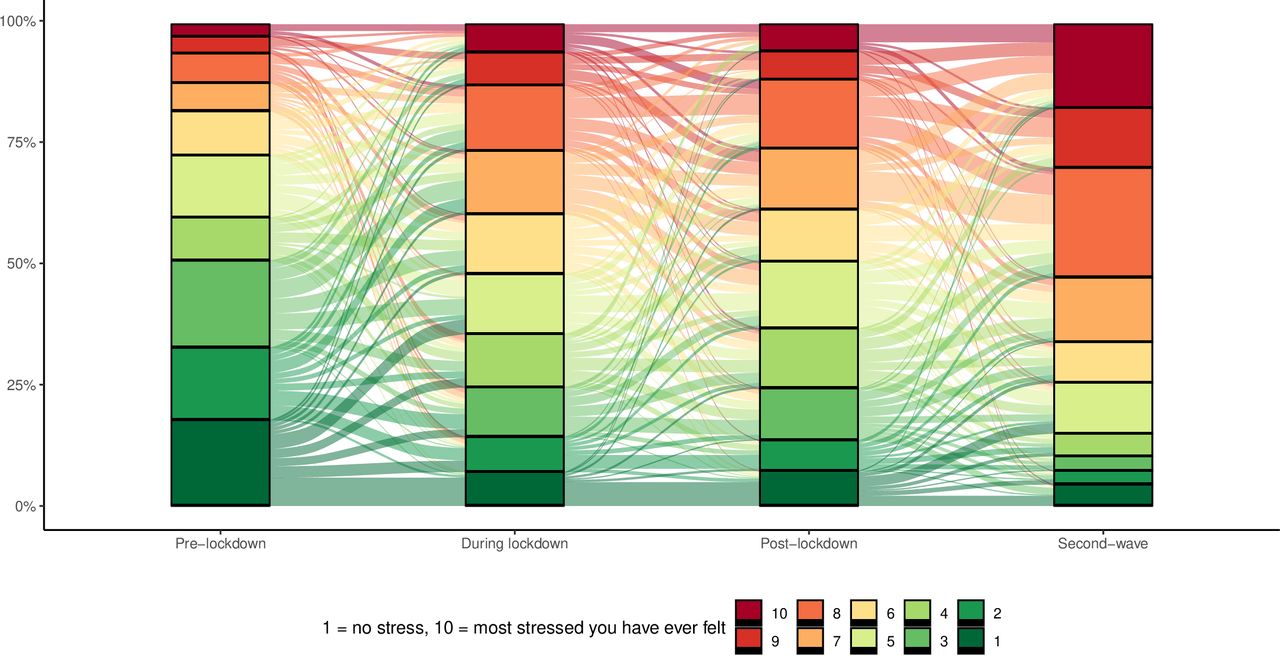
Stress score change over time.
Socioeconomic impact
Pre-COVID-19 employment rates were 57.2% (392/685) with a further 8.9% (61/685) self-employed, 18.4% (126/685) retired, 7.4% (51/685) unable to work due to disability and 2.7% (20/685) unemployed. 14 (2.9%) patients were in full time education. During lockdown 68.0% (466/685) reported their income was unaffected and 16.5% (113/685) were part of the furlough (85) or self employment support (28) schemes. 8.2% (56/685) reported reduced or no income following lockdown and 2.2% (15/685) reported having to rely on friends and family. Of those in employment who were not furloughed 15.1% (59/392) continued to work as usual, 6.4% (25) worked with workplace alterations, 40.6% (159) worked from home and 12.5% (49) reported being unable to work.
At the time of the survey postlockdown, 13 reported new unemployment, 2 had retired and 5 newly reported being unable to work due to illness or disability.
Future care
The COVID-19 pandemic has accelerated changes to how healthcare is delivered; with rapid introduction of telephone, video and online consultations. Patients were asked to select acceptable methods of follow-up during times of remission or during a flare. During a flare, acceptable follow-up methods were selected as follows; 65.8% (451/685) face-to-face consultation with an IBD physician or specialist nurse, 43.9% (301) telephone, 41.6% (285) video consultation and 29.1% (199) remote web or app-based follow-up. Preferences were reversed during remission with telephone follow-up being the most acceptable (67.3%, 461) and face to face being the least acceptable (36.6%, 251) (see figure 2). Excluding face-to-face appointments, patients over the age of 55 years showed a preference for telephone follow-up. Compared with younger patients those aged over 55 were less likely to report acceptability of app or video follow-up while either in remission (OR 0.28, 95% CI 0.20 to 0.39, p=2.2e-13) or flare (OR 0.38, 95% CI 0.27 to 0.53, p=1.0e-8).

Acceptability of different modalities of future appointments depending on patient condition. IBD, inflammatory bowel disease.
Patient comments
We invited all participants of the IBD COVID-19 lockdown survey to leave comments at the end of the survey with 200/685 patients taking this opportunity. Manual and computational natural language processing both categorised 58 comments to have a positive theme, all thanking the IBD team for their care during the pandemic. 64 comments were classified as having a negative theme, with the remainder neutral. The most common negative themes were; delays in receiving ‘at-risk’ notification (28/62); concern regarding communication between patient, GP, IBD team and other specialists, particularly in assigning risk (24/62) and concerns that the pandemic had negatively affected their IBD care (12/62) (see figure 3 for word clouds showing the most commonly used terms).

{kind=link}
{kind=link}
{kind=link}
Word clouds of positive (A) and negative (B) comments.
Discussion
In our IBD survey cohort, 72% were receiving biological/small molecule and/or immunomodulatory medications. This corresponds to our patients with IBD who were identified as vulnerable to COVID-19 infection via our electronic health record. This population was advised to follow stringent social distancing or shielding and therefore was targeted with our survey.
In line with BSG guidance, there were few changes in IBD medication. This is despite significant patient anxiety caused by the COVID-19 pandemic and caution from physicians due to a lack of data. Most mediation changes were initiated by our IBD team with only a few medications stopped or started by patients or their GP. Most commonly stopped medication were systemic steroids, followed by immunomodulators, which is supported by the emerging evidence from the SECURE-IBD database pointing towards poorer COVID-19 outcomes with these medications.6 Primary care involvement in IBD flare management was low at 5% but resulted in 44% (4/9) of all oral prednisolone prescriptions. GPs have a limited range of treatment options compared with IBD teams and it is unclear why these patients were not directed to the IBD team for investigation and management.
Of the three surveyed patients with IBD testing positive for COVID-19, only one was following stringent social distancing, with none in a high-risk group. With less than 0.5% of patients contracting PCR-proven COVID-19 infection, stringent social distancing and shielding clearly was beneficial in this IBD population surveyed, with lower infection rates compared with the national average in England of about 6%.7
In our survey population, we saw increasing levels of stress during the lockdown period, persisting despite easing of restrictions and even increasing when faced with the possibility of a second wave of COVID-19. However, the effects of a lockdown and quarantine on mental health should not be underestimated. In the H1N1 pandemic 30% of isolated adults experienced post traumatic stress disorder.8 Key factors contributing to this include fear of infection for themselves or others, lack of basic supplies, misinformation and the length of quarantine.9 10 The lockdown period in the UK lasted for 105 days, with adverse psychological effects of quarantine being reported after just 10 days.11 Our data are supported by a recent UK cross-sectional study of mental health during the pandemic which has reported significant levels of anxiety and depression in 24% of participants. When patients in the government defined vulnerable groups were evaluated, higher health anxiety levels and general anxiety levels were reported compared with the general population.12 This highlights the need for psychological support for vulnerable and shielding patients.
Ten per cent did not get their vulnerable notification from any source, while approximately one in five patients received notification late in May or June. A total of 135/180 patients on immunomodulator monotherapy received government letters informing them they must shield. For 102/135 with no additional risk factors, this information was incorrect as the BSG advised stringent social distancing only. The problem of delayed and mixed messaging was echoed by patients leaving negative free text comments who described heightened medical and work related uncertainty and anxiety. One of the lessons learnt from the COVID-19 pandemic is that it is paramount to have an up to date database of IBD patients to rapidly and completely distribute relevant information to patients in a timely fashion.
Overall, a quarter of our respondents reported that they could not or did not shield. Nationally the adherence to shielding is unreported. An insight may be drawn from a study of lockdown adherence, with recent open access data from a national survey suggesting that 25% of the general UK population broke lockdown restrictions at least once.13 The reasons for non-adherence are complex and multifactorial. The likelihood of adherence is related to an individual’s personal circumstances and their perception of risk.14 Despite government initiatives, 17.5% of our patients were unable to shield due to their housing, dependents or financial situation. In case of future similar events, efforts should be made to support this minority.
In the current climate, accelerated by the COVID-19 pandemic, there is a drive to move services to remote contact.15 This is in line with our patients wishes, with our survey population expressing a strong preference for remote outpatient contact or monitoring. Only 18.5% and 9.9% listed face-to-face appointments as their only acceptable follow-up option at times of flare or remission, respectively. The remainder of the population were willing to have follow-up via one or more remote methods, including patient-initiated contact. Whether these preferences will persist once the risk from COVID-19 has abated is unknown.
This study has limitations. The cohort demographics are not representative of the whole UK IBD population are so patients’ views may differ in other areas. There is also a gender bias in the cohort with more female respondents which may indicate a non-responder bias. We deliberately targeted written invitations to participate at patients who we assessed to be at-risk either by medication exposure, age or comorbidities; the views expressed may be different in a population with less severe disease or fewer comorbidities. Finally, this survey was a conducted at a single point in time, there is, therefore, likely to be recall bias when asking about events and perceived stress at prior time points.
The COVID-19 pandemic has disrupted the normal way of life in the UK, but for some of our patients with IBD the impact of this unprecedented global emergency was far greater. This survey shows that the shielding strategy was widely accepted and effective in reducing COVID-19-related infections in vulnerable populations. However, in the event of a second wave and further lockdown measures, there are clear areas for improvement. First, availability of a robust data set of vulnerable patients with IBD is key, but according to the recent IBD-benchmarking exercise comprehensive use of electronic clinical management systems by IBD centres is yet to be achieved in the UK.16 The responsibility for prompt communication of shielding advice to this vulnerable group should be designated to the local IBD team to avoid delayed and conflicting information from multiple sources. Second, remote patient management systems should be further developed and embedded in clinical care to facilitate remote patient care and monitoring. Finally, there is a clear need for psychological and social support for patients with IBD with high levels of anxiety or difficulties in being able to shield as both these needs are currently unmet.
Acknowledgments
We would like to thank our IBD patient panel for their critique of our questionnaire particularly Melissa Fletcher and Lee Robinson. We also would like to thank Laura White from the experience of care team at UHS for her help with the gather tool.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rich_j_h
Contributors LD, RF and MG created the survey. RJH provided the statistical analysis. RJH, LD, RF and MG wrote the manuscript which JRFC and TS critically appraised.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Southampton research and development department deemed this survey a service evaluation project and not research. It was approved by University Hospital Southampton gastroenterology clinical governance lead and clinical effectiveness panel.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information. All data relevant to the study are included in the article.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.