Article Text

Statistics from Altmetric.com
Introduction
Barrett’s oesophagus (BE) is a condition where the normal stratified squamous epithelium is replaced by columnar epithelium. This process of replacement of one normal tissue with another is called metaplasia.1 An estimated 5.6% of adults in the USA have BE.2 The incidence of BE in the UK was found to be 27.7/100 000 person-years and in the Netherlands 31.4/100 000 person-years.3 The pathogenesis of Barrett metaplasia begins with an insult due to gastro-oesophageal reflux of acid and bile that damage oesophageal squamous cells. It is not entirely known why the body repairs through the process of columnar metaplasia rather than by regeneration of squamous epithelium.4 BE is a strong risk factor for oesophageal adenocarcinoma (EAC), with the absolute annual risk of 0.09%–0.33%.3 5–7
Screening patients with long-standing GERD symptoms for BE and surveilling patients with BE with a regular endoscopic evaluation to detect curable neoplasia has been the usual practice.8 Studies have shown that patients who underwent surveillance had earlier-stage tumours and higher survival rates than those whose tumours are discovered later after the development of symptoms such as dysphagia or weight loss.9 10 Current society guidelines recommend endoscopic screening for BE in patients with chronic GERD symptoms who have at least one additional risk factor such as age >50 years, Caucasian race, male sex, hiatal hernia, elevated body mass index or tobacco use.8 11–13
Currently, the screening is done by random four-quadrant biopsies which are taken every 1–2 cm throughout the BE segment.12 This technique may miss early lesions14 along with being time-consuming. It obtains samples only from ~5% of the total area of BE.15 Wide-area transepithelial sampling (WATS) with computer-assisted three-dimensional (3D) analysis (WATS3D; CDx Diagnostics, Suffern, New York, USA) is a novel technique that combines an abrasive brush biopsy sampling, followed by computer-assisted pathology analysis. Recent studies have evaluated WATS3D as an adjunctive tool to Seattle protocol biopsies and found that there was an incremental yield in detection rates of both BE and oesophageal dysplasia (ED).16–19 Although it has been gaining popularity, it is still not widely incorporated across the USA. We decided to do a meta-analysis to compare the detection rates of BE and ED between forceps biopsy (FB) and WATS in adjunct to FB in patients who underwent endoscopy.
Methods
Search strategy
A comprehensive search of databases, including EMBASE, PubMed, SCOPUS, CINAHL and Cochrane databases from inception to 26 April 2020, was conducted. An expert medical librarian helped conduct the literature search with inputs from the study authors. Keywords used in the search included a combination of “wide area transepithelial sampling” OR “WATS” OR “Transepithelial sampling” AND “Barrett’s esophagus.” Our study was registered in OSF and we used the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and a predefined protocol, to identify studies reporting usage of WATS in BE. We restricted our search to studies published in peer-reviewed journals or presented as abstracts at national society meetings. Based on preset inclusion and exclusion criteria, three authors (VCSK, AS and PH) independently reviewed the studies, and all studies that did not address this topic were excluded. The selected articles were reviewed to ascertain if they contained the necessary relevant data. The bibliographic sections were searched for similar studies. Any discrepancy in including studies was resolved by a coauthor (VSP).
Study selection
We included studies that met our inclusion criteria, which included (1) patients with BE (2) age >18 years (3) use of WATS as an adjunct to FB (4) data on the diagnostic yield of both FB and WATS. We only included studies that were in English and met all our inclusion criteria. Our exclusion criteria included (1) no data on diagnostic yield, (2) age <18 years, (3) no data on additional yield of WATS and (4) case reports. Studies that had any one of these were excluded.
Data abstraction and quality assessment
A data extraction sheet was created, and the study characteristics, data on intended outcomes and patient characteristics were collected. VCSK and AS independently extracted data. All the data were reviewed by a coauthor (VSP) for potential discrepancies and were resolved.
The quality of included studies was determined objectively using a scale based on the Newcastle-Ottawa scale for meta-analysis. The scale consisted of six questions, and each received 0, 1 or 2 points if the study had adequately met the criteria. We considered a total score of ≥6, 3–5 and <2 as high, fair and poor quality, respectively. Two authors (VCSK and AS) independently assessed the quality of the studies. The senior author (BS) reviewed the final quality assessment table and resolved any discrepancies.
Outcomes
The primary outcome of the study was to analyse the incremental yield in the detection rates of BE and ED by WATS when used as an adjunct to FB. This was done by calculating the absolute and relative increase in detection rates of BE and ED, respectively, while using WATS with FB as compared with using FB alone. The relative increase in reduction rate is defined as the relative odds of detecting BE and ED by using WATS in conjunction to FB versus FB alone; while the absolute increase in detection rate is defined as the absolute difference of detection rates between WATS with FB and FB alone.
Statistical analysis
We performed a meta-analysis to calculate the absolute and relative increase in detection rate separately for BE and ED using Mantel-Haenszel statistical method with a random-effects model in all screening and/or surveillance endoscopies. For all practical purposes, the relative increase in detection rate is shown as risk ratio (RR) and absolute increase in detection rate was shown as risk difference (RD) in the Forrest plots generated using RevMan V.5.3 software. We assessed the heterogeneity between studies-specific estimates using the I2 statistic calculated. Publication bias was determined qualitatively by visually inspecting the funnel plot. Egger’s test was performed for objective evidence of publication bias for BE but not for ED as the number of studies were small (<10).
Results
Search results and population characteristics
A total of 267 studies were identified using our search strategy, of which 99 studies were removed after initial screening for duplicates, review articles, and surveys. A further 141 studies were removed after reviewing the title and abstract. Of the total 27 studies assessed in their entirety, 15 were excluded and 12 were included in the final analysis based on our exclusion and inclusion criteria (figure 1). Eleven studies (excluding study no.12) and nine studies (excluding study nos. 3,7,11) were included in the analysis for BE and ED, respectively. The excluded studies did not have adequate data for the respective analysis. The study characteristics are shown in table 1.
Study characteristics

Study flow diagram.
Analysis of diagnostic yield of WATS as an adjunct to FB
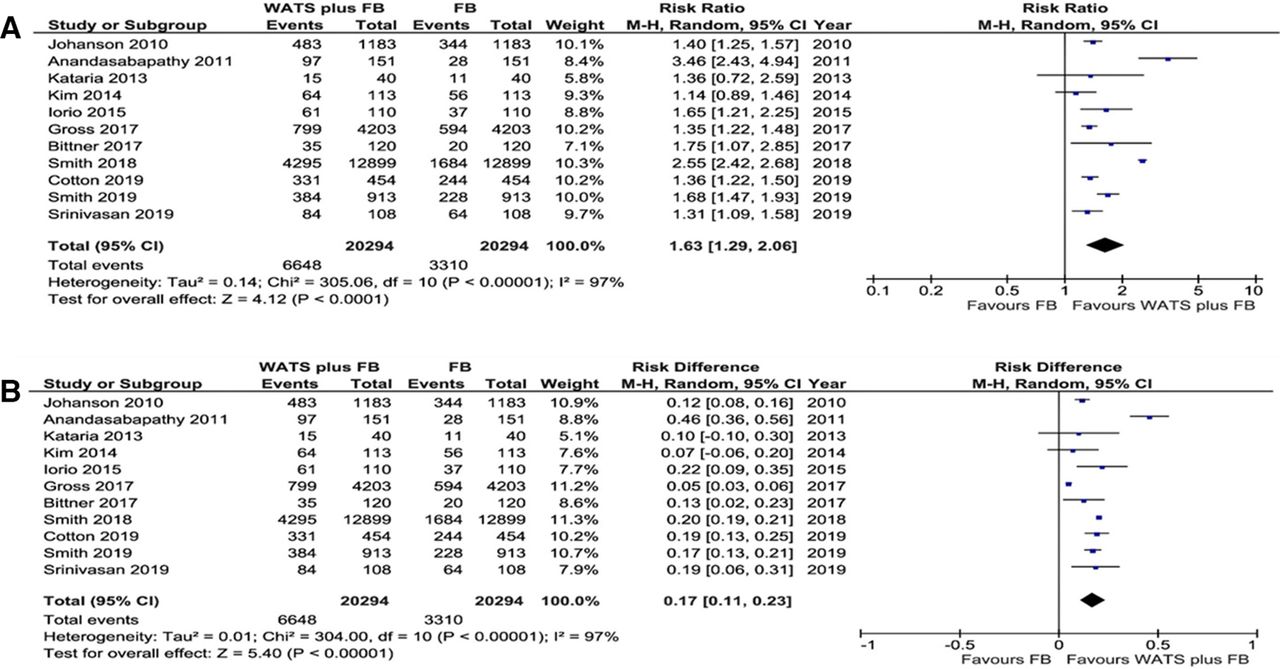
For BE, combined data from 20 392 screening endoscopies across 11 studies showed a significant increase in the absolute and relative detection rates. A total of 6643 lesions (intestinal metaplasia) were identified when WATS was used with FB versus 3310 with FB alone; an additional 3333 lesions identified. The absolute increase in detection was 16% (measured as RD −0.16, 95% CI 0.10 to 0.22, p<0.00001) and a 1.62 times relative increase in detection rates of BE (measured as RR −1.62, 95% CI 1.28 to 2.05, p<0.0001) with a number needed to test (NNT) of 6.1 when WATS was used in adjunct with FB (figure 2).

Forest plots comparing WATS+FB versus FB for Barrett’s oesophagus. (A) Relative increase in detection rate. (B) Absolute increase in detection rate. FB, forceps biopsy; M-H, Mantel-Haenszel Equation; WATS, wide-area transepithelial sampling.
There is a significant increase in absolute and relative detection rates for ED as well. Out of the 19 950 screening and surveillance endoscopies done in dysplasia naïve patients across nine studies, 533 lesions (dysplasia) were identified with WATS combined with FB vs 213 lesions with FB alone. With 320 more lesions identified, it translates to a marginal 2% but significant absolute increase (measured as RD 0.02, 95% CI 0.01 to 0.03, p=0.001) in additional diagnostic yield from WATS. There is a 2.05 times relative increase in the detection rate of ED (measured as RR 2.05, 95% CI 1.42 to 2.98, p=0.0001) yielding an NNT of 50 patients (figure 3).

Forest plots comparing WATS+FB versus FB for oesophageal dysplasia. (A) Relative increase in detection rate. (B) Absolute increase in detection rate. FB, forceps biopsy; M-H, Mantel-Haenszel Equation; WATS, wide-area transepithelial sampling.
Study quality assessment
We have used published data from both peer-reviewed articles and abstracts presented at national conferences. For BE, data extracted from fourarticles and seven abstracts were used. Three studies have at least sample sizes >1000, seven studies have sample sizes between 100 and 1000 and 1 study <100. For ED, data extracted from five articles and four abstracts were used. Three studies have at least sample sizes >1000, with the largest study having a sample size of 12 899, six studies have sample sizes between 100 and 1000. Based on the quality assessment scale, seven studies were of high and five were of fair quality. No study was poor in quality. Smith et al19 contributed approximately greater than 60% of the data in this study19 (table 2).
Study quality assessment based on Newcastle-Ottawa scale
Validation of meta-analysis results
We validated the meta-analysis results using sensitivity analysis, a test of heterogeneity and the assessment of publication bias.
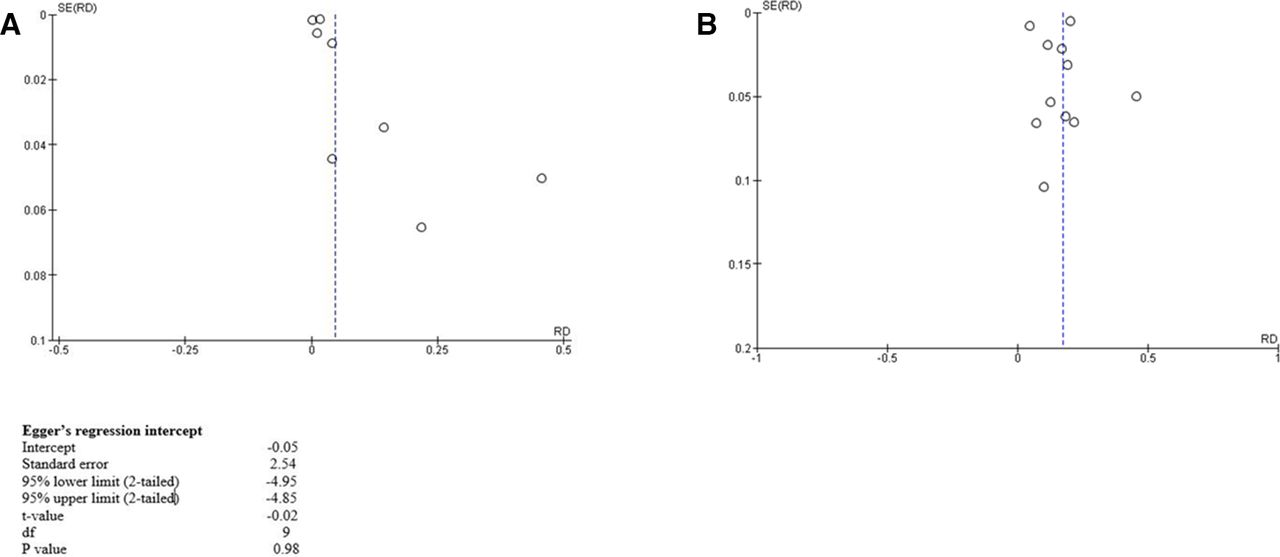
For sensitivity analysis, the effect on the summary estimate was analysed by excluding one study at a time iteratively. No one study had a major impact on the outcome or heterogeneity. Based on I2 analysis, there was considerable heterogeneity of >75% in all four meta-analyses as noted in our forest plots. There was some evidence of a publication bias based on the inspection of the funnel plots which can be attributed to the benefit of using WATS in conjunction with FB (figure 4A,B). Egger’s test for BE studies showed that there was no evidence of bias (p-0.98).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plots for assessment of publication bias. (A) Barrett’s oesophagus. (B) Oesophageal dysplasia.
Discussion
Our meta-analysis showed that WATS performed along with FB significantly increased the diagnostic yield of both BE as well as ED. This was found to be true in both the patients who underwent screening and those who underwent surveillance endoscopies. This is in line with studies that have been done so far. Our results indicate a minimum of 16% increase (construed from RD) and a maximum of 62% increase (construed from RR) in the detection rate of BE. However, it is also important to note that there is only a marginal 2% absolute increase in the detection of ED. This marginal increase in the detection rate for ED can be attributed to the relatively fewer proportion of ED cases with respect to the total number of BE cases. Nevertheless, there is a 105% increase (construed from RR) in the detection rate of ED indicating a strong likelihood of detection with the general usage of WATS with FB. If we presume that this modality is used on a standardised basis in community settings, we can extrapolate when WATS is used in conjunction with FB, there could be a substantial diagnostic benefit in earlier detection of metaplastic or dysplastic lesions. This translates to possible survival advantage due to the early detection of precancerous lesions of EAC.
Major professional organisations such as American College of Gastroenterology (ACG),20 American Gastroenterology Association (AGA),11 American Society for Gastrointestinal Endoscopy (ASGE),21 British Society of Gastroenterology (BSG)22 and Société Française d'Endoscopie Digestive23 currently do not recommend routine screening for detection of BE. ACG and AGA recommend an individualised approach for the patients involving discussion of potential risks, benefits and limitations of screening. ASGE and BSG recommend screening in select patients with risk factors such as frequent (several times per week), chronic and long-standing (greater than 5 years) GERD, males, white race with an age greater than 50 years, and those with nocturnal heartburn (grade C recommendation). Additionally, ASGE does not recommend any further screening if initial esophagogastroduodenoscopy (EGD) is negative. A combination of individual risk and a cost-effective minimally invasive test is key to unlocking population screening. Considering WATS requires endoscopy, it is unclear at present if there is a place for it in population screening pathways. Its usage is perhaps more suited for surveillance.
The current guidelines on the management of non-dysplastic BE, LGD and HGD have significant variations in treatment depending on the diagnosis and hence heavily rely on making an accurate diagnosis. The major societal guidelines (as cited above) recommend endoscopic surveillance every 3–5 years for non-dysplastic BE, if that is opted. However, for confirmed LGD and HGD cases, a therapeutic intervention in the form of endoscopic resection or ablation is preferred if the patient is agreeable. These management differences lay paramount importance on establishing accurate tissue diagnosis.
The Seattle Protocol recommends four quadrant biopsies every 1–2 cm throughout the complete length of the columnar-lined oesophagus along with separate biopsies from areas of mucosal abnormalities such as ulcers and nodules.24 Using this FB technique, a 4%–6% of the area of BE is sampled leading to an error in sampling the appropriate area and obtaining adequate samples. ACG guidelines acknowledge that the accuracy of this protocol ranges from 35% to 68%.1 This comes at a great cost of missing ED which might later develop into cancer and it is known through established trials that in patients with EAC, the survival significantly correlates with the stage at which it is diagnosed. Authors like Fountoulakis et al9 and Bhardwaj et al25 in their studies comment on how only a few patients with EAC are diagnosed with BE prior to the diagnosis of cancer, questioning the thoroughness of the currently employed techniques. A study showed that within the first year of follow-up of 11 028 patients who were newly diagnosed with BE, around 131 new cases of EAC were identified.5 The risk of death from EAC was not found to be lower in patients who underwent surveillance for BE. This calls into question our current surveillance methods and techniques for BE as well as emphasises the need for much larger prospective RCTs on the subject to potentially eliminate lead time bias.26
Docimo et al commented on the safety profile of the WATS procedure by conducting a retrospective analysis in March 2019 with no adverse event reported secondary to WATS.27
Currently, there are no large-scale studies that have analysed cost-effectiveness of WATS. Singer et al described an analytical model which suggested screening with WATS when used with the Seattle protocol was more cost-effective as compared with the Seattle protocol alone. However, multicentred international studies on the cost-effectiveness are warranted in order to establish its feasibility at a larger scale.28
Recent guidelines by ASGE state that WATS can be used as an adjunct to FB in patients with known BE or suspected BE when compared with white light endoscopy and FB. This was a conditional recommendation based on low-quality evidence.21
WATS as a stand-alone tool has not been studied in great lengths. A recent multicentre prospective trial conducted by DeMeester et al29 comparing WATS with standard FB reported similar frequency of detecting intestinal metaplasia overall which was published as an abstract only. Further research into WATS as an independent screening and diagnostic modality is warranted to validate its use as a stand-alone procedure. While there is suggestive evidence regarding increased diagnostic yield with HGD,30 31 similar data for LGD is lacking and so is their comparison. Additionally, there seem to be lack of concurrent data in these studies on the Prague classification which can help define the area of BE and prevent false positives.
To the best of our knowledge, this is the largest and most comprehensive meta-analysis done on this topic to date. Our study is also the first meta-analysis to compare the usage of WATS as an adjunct to FB as compared with FB alone in the diagnosis of BE.
There are limitations to our study. All the studies were from the USA. Lack of studies from other countries means that generalisability outside the USA is still not known until further studies are done involving non-USA population groups. We did not include studies published in other languages and this might have led to omittance of certain studies. Most of the studies were done at tertiary-level centres by expert gastroenterologists. So, we cannot generalise the result to general practice yet. Also, interuser variability needs to be assessed before adopting this technique universally. Lastly, all the studies included were non-randomised and open-labelled studies.
Conclusion
Our study shows that WATS, as an adjunct to FB, improves both the absolute detection rate and relative detection rate of both BE and ED as compared with FB alone. Although current data are promising, further multicentre, international, prospective studies are required before widespread usage of WATS is adopted.
Acknowledgments
We would like to acknowledge our librarian Rebecca Kindon for her help with the literature search.
References
Footnotes
Contributors VCSK (Conceptualisation: Lead; Data curation: Lead; Methodology: Equal; Project administration: Equal; Resources: Lead; Writing—original draft: Lead; Writing—review and editing: Lead). PH (Resources: Equal; Writing—original draft: Lead; Writing—review and editing: Lead). VSP (Formal analysis: Lead; Validation: Lead; Writing—original draft: Equal; Writing—review and editing: Equal). AS (Data curation: Lead; Methodology: Equal; Resources: Equal). UM (Conceptualisation: Supporting; Resources: Supporting; Writing—review and editing: Supporting). AS (Resources: Supporting; Supervision: Supporting; Writing—review and editing: Supporting). FG (Formal analysis: Support, Validation: support). NA (Formal analysis: Support, Validation: support). BS (Conceptualisation: Equal; Methodology: Equal; Project administration: Lead; Resources: Lead; Supervision: Lead; Validation: Equal; Writing—original draft: Supporting; Writing—review and editing: Equal).
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.