Article Text

Abstract
Background Current guidelines recommend bismuth-containing quadruple therapy (BQT) and quinolone-containing therapy after failure of first-line Helicobacter pylori eradication therapy. However, the optimum regimen of second-line eradication therapy remains elusive. We conducted a network meta-analysis to compare the relative efficacy of 16 second-line H. pylori eradication regimens.
Methods Three major bibliographic databases were reviewed to enrol relevant randomised controlled trials between January 2000 and September 2018. Network meta-analysis was conducted by STATA software and we performed subgroup analysis in countries with high clarithromycin resistance and high levofloxacin resistance, and in patients with documented failure of first-line triple therapy.
Results Fifty-four studies totalling 8752 participants who received 16 regimens were eligible for analysis. Compared with a 7-day BQT, use of probiotic add-on therapy during, before, and after second-line antibiotic regimens, quinolone-based sequential therapy for 10–14 days, quinolone-based bismuth quadruple therapy for 10–14 days, bismuth quadruple therapy for 10–14 days, and quinolone-based triple therapy for 10–14 days were significantly superior to the other regimens. Subgroup analysis of countries with high clarithromycin resistance and high levofloxacin resistance revealed that the ranking of second-line eradication regimens was distributed similarly in each group, as well as in patients with failure of first-line triple therapy.
Conclusion We conducted a detailed comparison of second-line H. pylori regimens according to different antibiotic resistance rates and the results suggest alternative treatment choices with potential benefits beyond those that could be achieved using salvage therapies recommended by guidelines.
- Helicobacter pylori infection
- Helicobacter pylori - treatment
- meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Helicobacter pylori (H. pylori) prevails worldwide with global infection rates ranging from 44.3% to 60.3%.1 H. pylori infection is a predominant risk factor for gastric cancer, which remains the third leading cause of cancer death in both genders globally,2 and lower prevalence of H. pylori infection could contribute to a decline in gastric cancer mortality.3 Therefore, successful eradication of H. pylori infection in clinical practice is an important component of disease prevention.
Recently, several reviews reported alarming levels of H. pylori resistance to clarithromycin, metronidazole, and levofloxacin,4–6 and the prevalence of resistance to clarithromycin and levofloxacin were ≥15% in the Asia-Pacific region, as well as in other WHO regions, indicating that the selection of appropriate eradication regimens should be adjusted according to local surveillance in different countries. Clarithromycin-based triple therapy (TT), which was first developed during the 1990s, was recommended as a first-line eradication therapy due to a good eradication rate initially. Owing to the increasing resistance of H. pylori to clarithromycin, standard TT was abandoned as a first-line eradication therapy7 8 when the local resistance rate of clarithromycin was ≥15%. Many combination regimens have been proposed, including bismuth-containing quadruple therapy (BQT), concomitant therapy (CT), sequential therapy (ST), high-dose dual therapy (DT), and quinolone-based triple (QTT) or quadruple therapy. Two recent network meta-analyses (NMA) aimed at determining an optimal first-line eradication therapy were conducted, and the eradication therapies were grouped into 14 or 17 comparators, respectively.9 10 Although the priority of effective eradication regimens differed, both studies concluded that a longer duration was associated with a higher eradication rate in first-line therapy. However, the optimum regimen of second-line eradication therapy remains elusive despite intensive investigations.
In the search for optimal second-line eradication therapy, most trials focused more on the relative efficacy among burgeoning novel regimens and seldom compared the experimental group to one standard therapy. Although pairwise meta-analyses contribute considerable valuable evidence, few studies have performed robust comparisons among multiple eradication regimens. NMA, also known as mixed treatment comparison, simultaneously compares several treatment comparators using direct and indirect comparisons with preservation of randomisation in individual trials.11–13 Recently, an NMA was conducted to clarify the best second-line eradication regimen,14 but it lacked a comprehensive search methodology, inclusion of relevant studies was incomplete, and relatively few treatment comparisons were performed, and thus its application in clinical practice may be of limited value.
In the present study, we conducted an NMA to compare the relative efficacy and dropout rate of H. pylori second-line eradication among 16 treatment regimens in the past two decades to identify the most favourable second-line eradication therapy for patients with treatment failure. Furthermore, we performed a subgroup analysis to determine the priority of second-line regimens in countries with high clarithromycin resistance (≥15%) and high levofloxacin resistance (≥15%), and in patients with documented failure of first-line TT in order to verify the recommendation of the Maastricht V/Florence Consensus and American College of Gastroenterology (ACG) Clinical Guideline in 2017.7 8
Materials and methods
Search strategy and selection criteria
This study was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations.15 We searched the electronic databases including PubMed, Embase, and Cochrane Central Register of Controlled Trials without language restriction, and performed a manual literature search of references in retrieved articles and significant reviews for eligible publications. A detailed description of the search strategies is provided in online supplementary table S1. Because antibiotic resistance may rise incrementally and potentially bias the analysis, we restricted the inclusion of articles to those published between January 2000 and September 2018.
Supplemental material
We included randomised controlled trials that evaluated eradication rate of second-line H. pylori eradication therapy in adults with treatment-failure after first-line regimen (aged ≥18 years) and with a confirmed diagnosis of persistent H. pylori infection according to one or more standard detection methods (13C-urea or 14C-urea breath test, rapid urea test, histological examination, bacterial culture, or stool antigen detection) at least 4 weeks after completion of a first-line regimen. We included reports that compared 2 or more of 16 regimens. Reports that studied naïve patients, paediatric patients, pregnant women, or patients with histories of allergic reaction to antibiotics, active upper gastrointestinal bleeding, gastrectomy, endoscopic submucosal dissection, malignancy (including gastric or non-gastric origins), and severe concurrent comorbidities were excluded.
Outcome measures
We determined the H. pylori eradication rate of intention-to-treat (ITT) analysis at least 4 weeks after completion of a second-line eradication regimen from enrolled studies. We also analysed the H. pylori dropout rate due to loss of follow-up and adverse events during the follow-up period to investigate the therapeutic compliance and safety.
Data extraction and quality assessment
Two investigators (Y-LC and Y-CT) independently screened the titles and abstracts for eligibility, and full texts were assessed to clarify the eligibility status of each article. All discrepancies were discussed and resolved in consultation with a third investigator (S-IS). Non-English articles were translated. We calculated the ITT or attempted to contact the corresponding authors if it was not indicated in the article. The full text was requested from the investigators if needed. Two reviewers (Y-LC and Y-CT) extracted data independently and then the data were checked by a third investigator (S-IS). The following variables were extracted: participants’ characteristics, country of study, study design, detection methods of H. pylori infection, and details of regimens.
We grouped eradication therapies into 16 regimens according to clinical importance: bismuth-containing quadruple therapy for 7 days (BQT-7), bismuth-containing quadruple therapy for 10–14 days (BQT-10/14), triple therapy for 10–14 days (TT-10/14), sequential therapy for 10 days (ST-10), concomitant therapy for 7 days (CT-7), concomitant therapy for 10 days (CT-10), high-dose dual therapy for 14 days (DT-14), quinolone-based triple therapy for 7 days (QTT-7), quinolone-based triple therapy for 10–14 days (QTT-10/14), quinolone-based bismuth-containing quadruple therapy for 10–14 days (QBQT-10/12/14), quinolone-based sequential therapy for 10–14 days (QST-10/12/14), quinolone-based concomitant therapy for 7 days, rifabutin-based triple therapy for 7 days, and probiotic add-on therapy before, during, and after second-line antibiotic regimens (probiotics (before), probiotics (during), probiotics (after)). Two investigators (Y-LC and Y-CT) evaluated the risk of bias of all studies independently, and assessed the quality of the articles included in the analysis with version 2 of the Cochrane tool for assessing Risk of Bias in randomised trials (RoB V.2.0 tool).16 17 Disagreements were discussed until a consensus was reached and a third investigator (S-IS) was consulted when necessary.
Data synthesis and statistical analysis
First, we conducted a pairwise random-effect meta-analysis. The pooled ORs and 95% CI were reported for binary variables, and heterogeneity was assessed by visual inspection of the forest plot and tested using I2 statistics.18 For binary variables, we conducted a one-stage meta-analysis using a generalised linear mixed model with the exact binomial likelihood. Since the desired outcome was successful eradication of H. pylori infection, ORs>1 indicated superior efficacy.
Second, we undertook a frequentist NMA using Stata (V.16, Stata) for each outcome separately. We conducted mixed treatment comparisons of NMA with a random-effect model, which was based on the mvmeta command with the restricted maximum likelihood approach,19 to investigate treatment efficacy and the dropout rate. For dichotomous variables of the dropout rate, we noted zero events. For cell counts of zero, imputation with 0.5 was added.
Finally, we evaluated potential inconsistencies between direct and indirect evidence within the NMA using the design-by-treatment interaction model,20 loop-specific approach, and the side-splitting method.21 Statistical significance was set at 5% for all analyses. We also estimated the probabilities of each treatment being at each rank for each intervention and outcome. We obtained a treatment hierarchy using the surface under the cumulative ranking curve and mean ranks (SUCRA).22 Comparison-adjusted funnel plots23 and Egger’s tests were used to examine potential small-study bias after treatments were ordered from the oldest to the newest. For Egger’s test, we regarded a two-sided p value as significant when it was less than 0.05.
Subgroup analysis
In addition, we performed subgroup analysis to determine the ranking of second-line regimens in countries with high clarithromycin resistance (≥15%) and high levofloxacin resistance (≥15%), and in patients with documented failure of first-line TT. The resistance rates of H. pylori to clarithromycin and levofloxacin in each country were extracted from relevant articles (online supplementary table S2).6 24
Results
Literature search and eligible studies
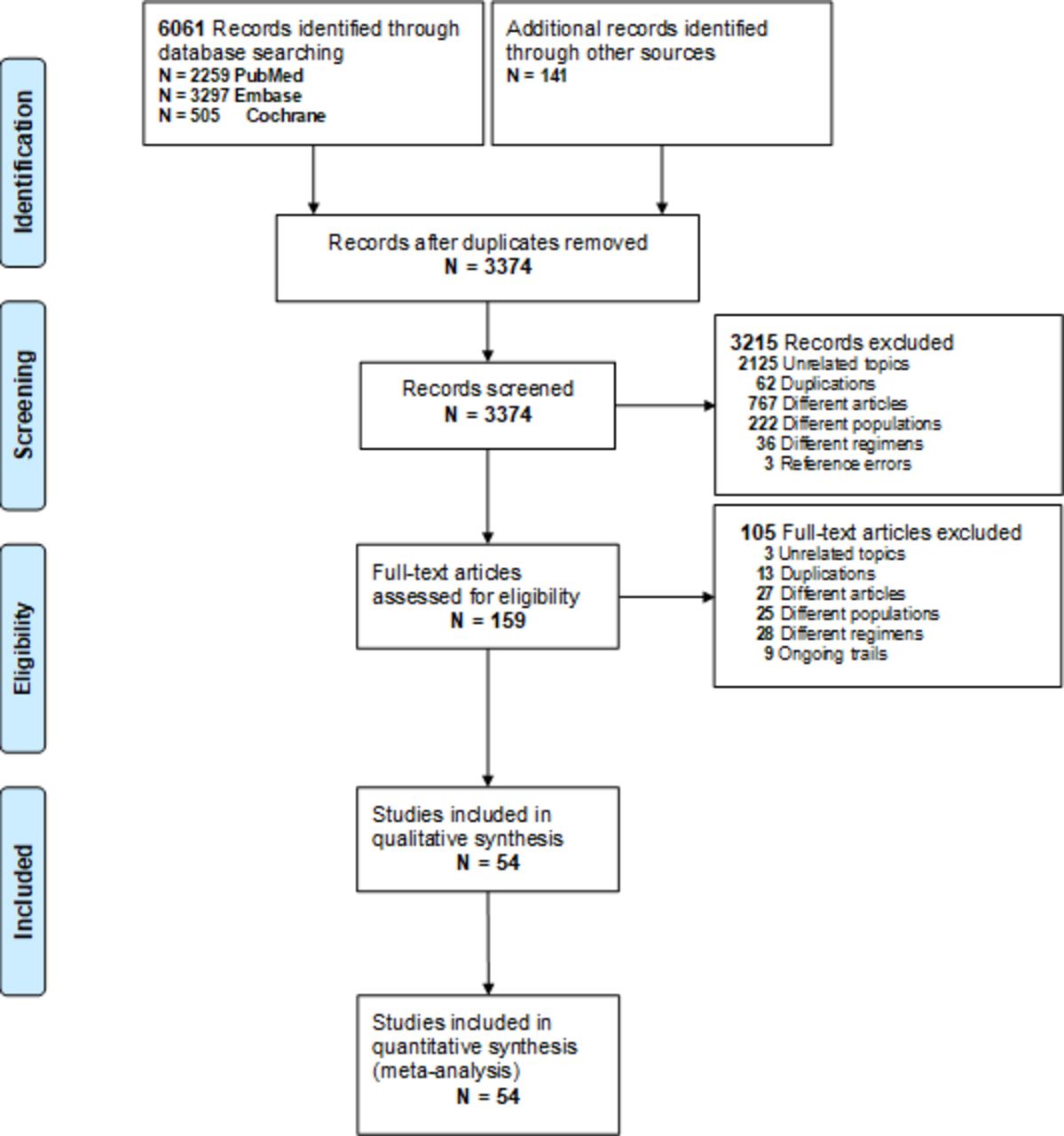
The comprehensive search strategy identified 6061 studies from electronic databases and a further 141 studies were identified by manual search (figure 1). After eliminating 2828 duplicated articles and screening the titles and abstracts of 3374 articles, 159 full-text articles were assessed for eligibility. Finally, we included 54 articles with a total of 8752 participants for qualitative and quantitative synthesis.
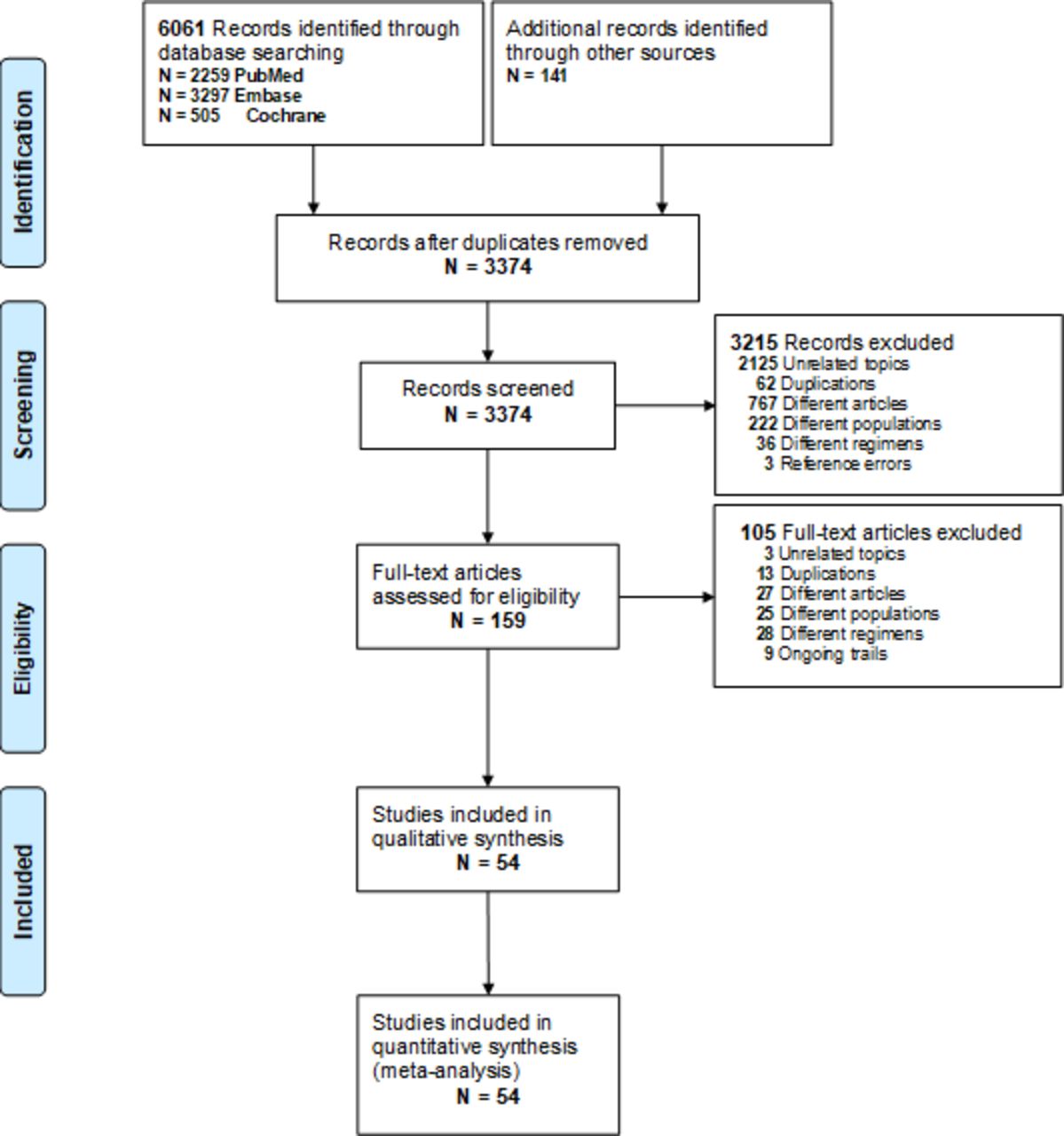
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Characteristics and clinical parameters of included studies
The methodological narrations and characteristics of study design and outcomes of the 54 randomised controlled trials are summarised in online supplementary table S3, table S4A, and table S4B. Among these studies, the sample size ranged from 48 to 600 (median 126), while the medians and IQRs for age and percentage of male gender were 49.5 (10.5), and 52.2 (9.9), respectively. Most studies were conducted in the Western Pacific (70.4%) region, and none were from African nations. Most trials enrolled patients after failure of first-line TT therapy (75.9%). Lactobacillus species (sp), Bifidobacterium sp, and Saccharomyces sp were the most common probiotics included in our review, while only one study prescribed Will yoghurt, a Korean brand containing multistrain probiotics. The eradication therapies commonly supplemented with probiotics were BQT-10/14 and QTT-10/14. The Cochrane Collaboration’s Risk of Bias assessment is shown in online supplementary table S5. For randomised controlled trials, some concerns were common in overall bias. Some studies did not describe the allocation sequence method thoroughly, or whether the trial personnel or participants were aware of their medications in the blinding process. Taken together, the aforementioned procedural issues resulted in some concerns regarding the domains of randomisation and deviations from the intended interventions.
Primary outcome: efficacy
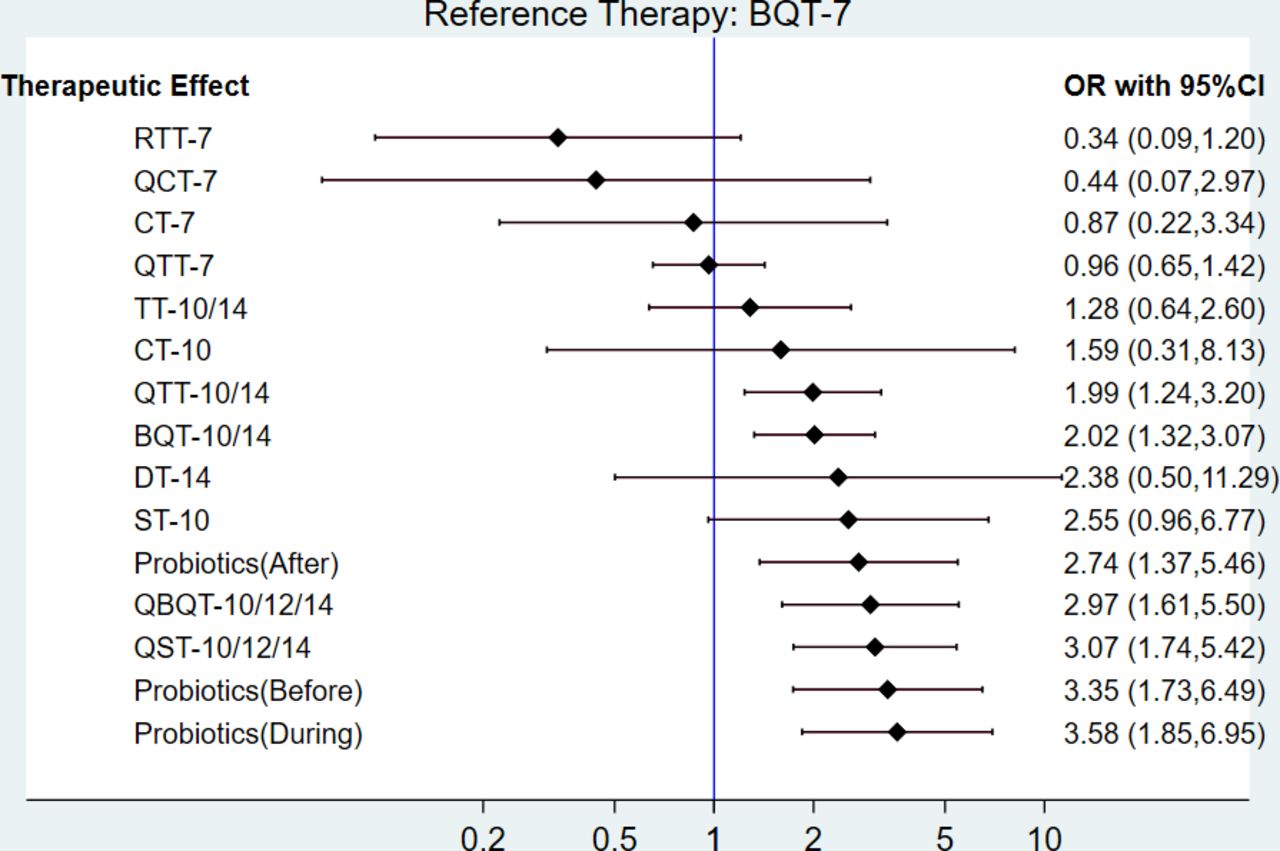
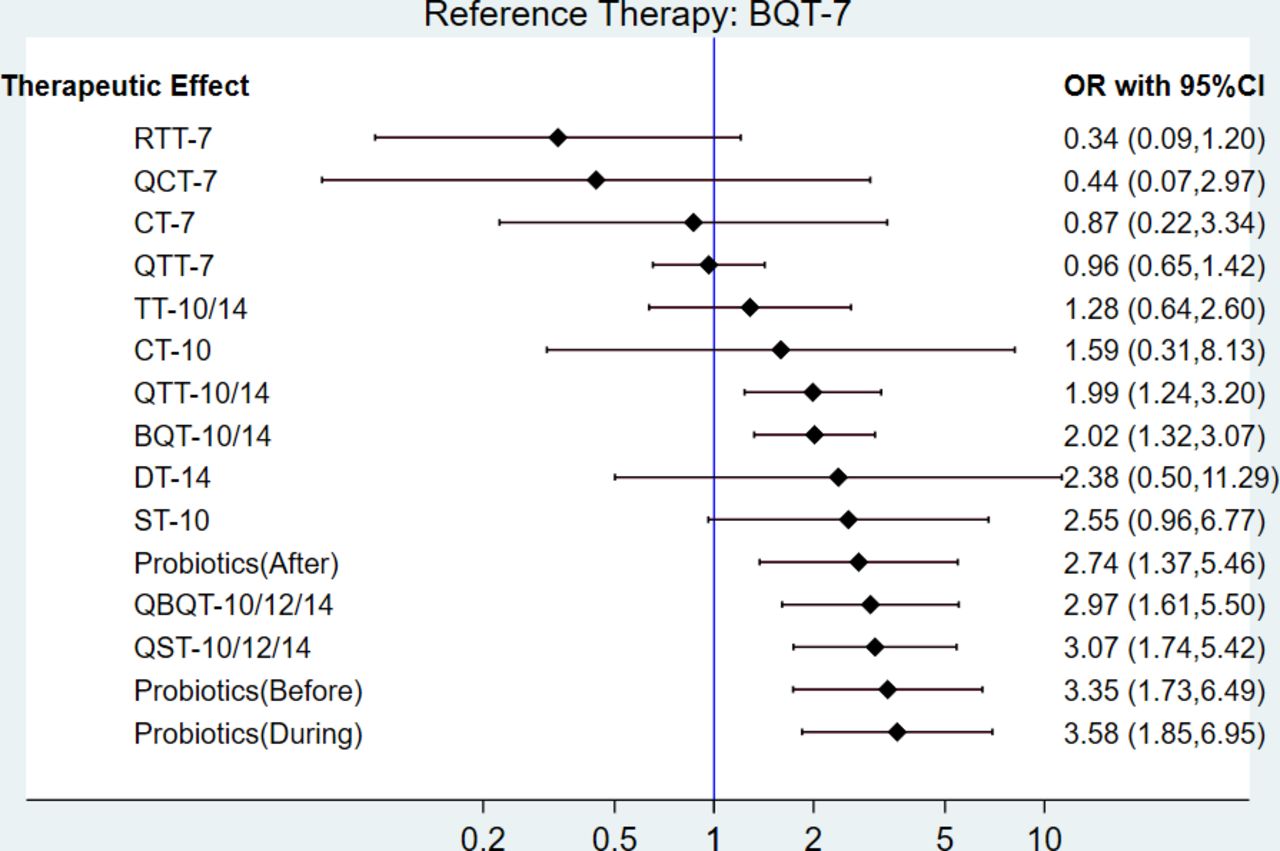
The network comparisons geometry for the efficacy of second-line H. pylori eradication therapies is shown in figure 2 (online supplementary figure S1A, S1B, S1C). The most common pairwise comparisons were BQT-7 versus QTT-7, followed by BQT-10/14 versus QTT-10/14. Among these 16 regimens, the regimens with the most participants enrolled in clinical trials were QTT-10/14, BQT-7, and BQT-10/14. Traditional meta-analyses of the included regimens are shown in online supplementary figure S2A. A forest plot of NMA for overall efficacy is shown in figure 3. When compared with BQT-7 (reference regimen), probiotics (during) (OR 3.58, 95% CI 1.85 to 6.95), probiotics (before) (OR 3.35, 95% CI 1.73 to 6.49), QST-10/12/14 (OR 3.07, 95% CI 1.74 to 5.42), QBQT-10/12/14 (OR 2.97, 95% CI 1.61 to 5.50), probiotics (after) (OR 2.74, 95% CI 1.37 to 5.46), BQT-10/14 (OR 2.02, 95% CI 1.32 to 3.07), and QTT-10/14 (OR 1.99, 95% CI 1.24 to 3.20) showed significantly greater efficacy and were at least twice as effective as the reference group. Moreover, regimens with longer duration tended to show higher efficacy of eradication compared with regimens with shorter duration. The means for eradication rates (%) of probiotics (during), probiotics (before), QST-10/12/14, QBQT-10/12/14, probiotics (after), BQT-10/14, and QTT-10/14 were 77.54, 78.96, 86.47, 80.31, 79.24, 78.78, and 73.72, respectively, while the mean for eradication rates of BQT-7 was 67.80.
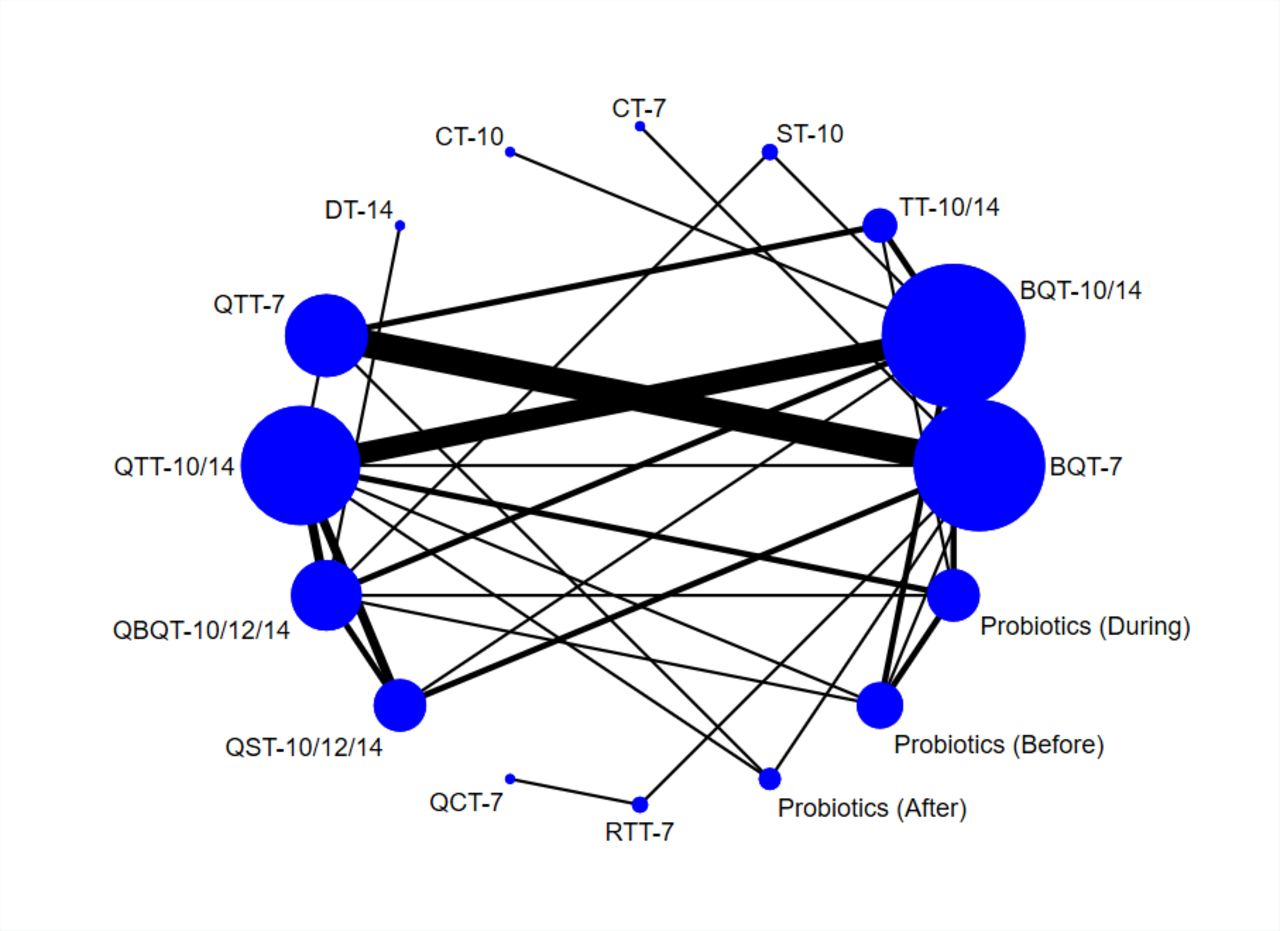
Network comparisons geometry of second-line H. pylori eradication therapies (overall). BQT-7, bismuth-containing quadruple therapy for 7 days; BQT-10/14, bismuth-containing quadruple therapy for 10–14 days; CT-7, concomitant therapy for 7 days; CT-10, concomitant therapy for 10 days; DT-14, high-dose dual therapy for 14 days; P+Regimen, add-on therapy of probiotics before second-line antibiotic regimens; QBQT-10/12/14, quinolone-based bismuth-containing quadruple therapy for 10–14 days; QCT-7, quinolone-based concomitant therapy for 7 days; QST-10/12/14, quinolone-based sequential therapy for 10–14 days; QTT-7, quinolone-based triple therapy for 7 days; QTT-10/14, quinolone-based triple therapy for 10–14 days; Regimen (P), add-on therapy of probiotics during second-line antibiotic regimens; Regimen +P, add-on therapy of probiotics after second-line antibiotic regimens; RTT-7, rifabutin-based triple therapy for 7 days; ST-10, sequential therapy for 10 days; TT-10/14, triple therapy for 10–14 days.
{kind=link}
{kind=link}
{kind=link}
Network forest plot of indirect comparisons (ORs) of second-line H. pylori eradication therapies (overall). BQT-7, bismuth-containing quadruple therapy for 7 days; BQT-10/14, bismuth-containing quadruple therapy for 10–14 days; CT-7, concomitant therapy for 7 days; CT-10, concomitant therapy for 10 days; DT-14, high-dose dual therapy for 14 days; P+Regimen, add-on therapy of probiotics before second-line antibiotic regimens; QBQT-10/12/14, quinolone-based bismuth-containing quadruple therapy for 10–14 days; QCT-7, quinolone-based concomitant therapy for 7 days; QST-10/12/14, quinolone-based sequential therapy for 10–14 days; QTT-7, quinolone-based triple therapy for 7 days; QTT-10/14, quinolone-based triple therapy for 10–14 days; Regimen (P), add-on therapy of probiotics during second-line antibiotic regimens; Regimen +P, add-on therapy of probiotics after second-line antibiotic regimens; RTT-7, rifabutin-based triple therapy for 7 days; ST-10, sequential therapy for 10 days; TT-10/14, triple therapy for 10–14 days.
The indirect comparisons of NMA are summarised in table 1 and the SUCRA probability is shown in Figure S3A. Funnel plot did not reveal any visually remarkable asymmetry (online supplementary figure S4A), and Egger’s test showed no significant publication bias (online supplementary figure S5A). Simultaneously, we used several methods to assess inconsistency between direct and indirect evidence (online supplementary table S6, S7, S8). There was no significant inconsistency using the design-by-treatment model (p=0.77) and loop-specific approach (p=0.62). However, using the side-splitting method, we only found statistically significant inconsistency in the comparison of BQT-7 versus QTT-10/14 (p=0.04).
We also performed subgroup analyses in countries with high clarithromycin resistance (≥15%) and high levofloxacin resistance (≥15%), and the priority of second-line eradication regimens was also distributed similarly in each group. In countries with high clarithromycin resistance (online supplementary figure S6A), probiotics (during), probiotics (before), QST-10/12/14, QBQT-10/12/14, probiotics (after), BQT-10/14, and QTT-10/14 had greater efficacy with statistical significance. In countries with high levofloxacin resistance (online supplementary figure S6B), probiotics (before), probiotics (during), QST-10/12/14, QBQT-10/12/14, probiotics (after), and BQT-10/14 showed significantly greater efficacy. Furthermore, a trend of higher efficacy of eradication in regimens with longer duration was also noted. Funnel plot did not reveal any visually remarkable asymmetry and Egger’s test did not reveal any publication bias. Regarding the assessment of inconsistency, the side-splitting method detected statistically significant inconsistency only in subgroup analyses for high clarithromycin resistance. In participants with failure of first-line standard TT (online supplementary figure S6C), probiotics (during), probiotics (before), QBQT-10/12/14, probiotics (after), QST-10/12/14, QTT-10/14, and BQT-10/14 showed a statistically significant difference when compared with BQT-7.
Secondary outcome: dropout rate
Because adverse events and patients’ adherence lead to dropout, we calculated the dropout rate from the number difference between ITT and per-protocol groups in all included trials. We observed that there was statistical heterogeneity in the Probiotics (After), QTT-10/14, Probiotics (During), QTT-7, and QST-10/12/14 groups (online supplementary figure S6D).
Discussion
In this NMA, we comprehensively compared 16 treatment regimens since 2000 to clarify the relative efficacy and tolerability of H. pylori second-line eradication therapy in treatment-experienced patients. We demonstrated that probiotics (during), probiotics (before), QST-10/12/14, QBQT-10/12/14, probiotics (after), BQT-10/14, and QTT-10/14 were significantly superior to the other regimens when compared with BQT-7 in treatment-experienced patients. In addition, extending the duration of regimen to longer than 10 days achieved a higher efficacy of eradication compared with that achieved by a regimen lasting 7 days in duration. With respect to dropout rate, there was a decreasing trend of withdrawal and loss of follow-up that was documented frequently in the probiotics (after), QTT-10/14, probiotics (during), QTT-7, and QST-10/12/14 regimens. The priority of second-line eradication regimens was also distributed similarly, not only in countries with high clarithromycin resistance (≥15%) and high levofloxacin resistance (≥15%), but also in patients with failure of first-line TT. Therefore, our NMA demonstrated robust comparisons of second-line H. pylori regimens according to different antibiotic resistance rates, and the results suggest alternative treatment choices with potential benefit beyond the salvage therapies recommended by guidelines.
In general, the most important factors for successful treatment of H. pylori include the pretreatment resistance rate of antimicrobial agents, treatment duration, regimen composition, and patient compliance with eradication regimens. Most available treatment data were trial based, and these results were not generalisable and transferable to different regions owing to the variable distribution of antibiotic resistance rates. For first-line eradication therapy, eradication regimens took local prevalence of clarithromycin resistance into account and extended the duration to 10–14 days.7 8 Previous meta-analyses also found that prolonging the treatment duration to more than 10 days was associated with an improved eradication rate.9 10 25 For second-line therapy, Yeo et al14 and Muñoz et al26 reported that eradication effectiveness was associated with longer duration, which was consistent with our finding. With respect to dropout rate, the trend of withdrawal and loss of follow-up decreased among the probiotics (after), QTT-10/14, probiotics (during), QTT-7, and QST-10/12/14 regimens. The effects of adverse events have seldom been investigated in meta-analyses due to inconsistent standards of safety reporting and selective outcome reporting in previous meta-analyses. We used the dropout rate as a surrogate outcome to reflect patients’ adherence based on the presence or absence of adverse events in daily practice. However, the optimal duration of second-line therapy remains controversial as the effects of post-treatment resistance rate of antibiotics, patient compliance, and cost-effectiveness need to be taken into account.
Prescribing probiotics as an adjuvant therapy in the treatment of H. pylori eradication therapy has been proposed recently, and emerging evidence suggests that probiotic add-on therapy might reduce the adverse effects of eradication regimens and could increase compliance in first-line therapy.7 8 27 Currently, Lactobacillus sp and Bifidobacterium sp are the best-studied probiotics, and Lactobacillus-containing supernatants can significantly reduce the viability of H. pylori independent of lactic acid concentrations. Several mechanisms have been published to explain the possible inhibitory effects of probiotics on H. pylori growth including antimicrobial substance production,28 epithelial cell adhesion site competition,29 mucosal barrier stabilisation,30 immune response regulation,31 and probiotic-induced sIgA secretion, as well as enhancement of mucosal immune function. Moreover, probiotics could minimise the disorganisation of gut microbiota, which might reduce adverse effects related to antibiotics-associated microbiota impairment.32 A recent meta-analysis of 13 randomised controlled trials involving 2306 patients investigating the effects of probiotics supplementation on H. pylori eradication revealed an improved eradication rate (RR 1.15, 95% CI 1.10 to 1.20) and lower incidence of adverse effects (RR 0.71, 95% CI 0.54 to 0.94) with moderate heterogeneity.33 Subgroup analysis showed that probiotic supplementation in patients with sequential and quadruple therapy did not improve the eradication rate, whereas multistrain probiotics might be more beneficial than Lactobacillus alone in terms of overall incidence of side effects. Another NMA analysing the adjuvant effect of probiotics on first-line eradication therapy indicated that probiotics promoted the effectiveness of eradication, especially when combined with BQT, used before and during eradication regimen, mixed with multiple species of probiotics, and when use of probiotics was extended for more than 2 weeks.34 In this study, we demonstrated that probiotic add-on therapies, especially during, before, and after second-line antibiotic regimens, were superior to other regimens in second-line eradication therapy, and most probiotics in our analysis were used for longer than 2 weeks and were combined with BQT or QTT-10/14. Since antibiotics could have an inhibitory effect on probiotics, prescription of probiotics for longer than 2 weeks before an eradication regimen, or taking probiotics and antibiotics separately with a longer interval during the eradication period might enhance the eradication efficacy and minimise any adverse effects.
According to the Maastricht V/Florence Consensus, BQT and quinolone-containing triple or quadruple therapy are recommended as second-line therapy after failure of first-line standard TT or non-bismuth quadruple therapy.7 In 2017, the ACG Clinical Guideline recommended BQT, levofloxacin TT, or DT, depending on the individual history of antibiotic allergies and whether first-line TT contained fluoroquinolone or not.8 Recently, Gisbert et al found that quadruple therapy containing levofloxacin and bismuth for 14 days achieved a higher eradication rate than second-line therapy after previous failure of standard TT.35 In a previous review, Cheng et al demonstrated that moxifloxacin-containing TT for 7 days was more effective and better tolerated than BQT-7 after failure of TT.36 In another meta-analysis of the efficacy of levofloxacin TT as second-line treatment, the overall eradication rate was 74.5% (95% CI 70.9% to 77.8%). The eradication rate was higher than 80% when the duration was longer than 10 days, when levofloxacin was prescribed one time a day, and when patients received a levofloxacin-susceptible strain.37 Furthermore, the predicted efficacy of levofloxacin TT might be lower than 80% when the levofloxacin resistance is higher than 5%–10%. Therefore, BQT continues to be the first priority of second-line eradication therapy, especially in areas of high quinolone resistance rate or when expanding the duration from 7-day to 14-day regimens.38 In the present review, we found that QST-10/12/14, QBQT-10/12/14, BQT-10/14, and QTT-10/14 may have potential as alternative second-line therapies. QST-10/12/14, QBQT-10/12/14, and BQT-10/14 were superior to QTT-10/14 in terms of high levofloxacin resistance (≥15%).
DT is another emerging treatment choice for second-line therapy and two common compositions of DT exist in clinical research. Yang et al developed a version of DT in 2015,39 comprising amoxicillin and high-dose proton pump inhibitors (PPI) given 4 times daily for 14 days, which maintained the intragastric pH at a value higher than 6.5 regardless of CYP2C19 genotype40 and provided a steady plasma concentration of amoxicillin above the minimal inhibitory concentration level for H. pylori.41 Another meta-analysis in 2016 proposed a DT regimen that involved taking amoxicillin ≥2 g/day and high-dose PPI 3–4 times daily.42 In two recent meta-analyses, DT showed comparable eradication efficacy and fewer side effects when compared with BQT for 10–14 days43 or guideline-suggested rescue therapies.42 However, the inclusion criteria with respect to the definition of DT differed in these two meta-analyses, while most patients enrolled in the study by Yang et al received a first-line eradication regimen, and Gao et al included studies with H. pylori strain resistant to both metronidazole and clarithromycin, as well as patients who failed treatment more than two times.39 More trials might be needed to determine the efficacy and safety of DT in both first-line and second-line regimens. In this study, we found the efficacy of DT-14 was not different compared with ST-10, CT-10, and TT-10/14.
There were several limitations in this NMA. First, we analysed the eradication therapies according to the prevalence of antibiotic resistance rate, clinical importance, and availability of antibiotics, and did not include vonoprazan-containing regimen. In H. pylori eradication therapy, increasing the intragastric pH >5 could induce the bacteria to enter the replicative state and become more susceptible to both amoxicillin and clarithromycin.44 Recently, vonoprazan (TAK-438), a potassium-competitive acid blocker developed by Japan Takeda Pharmaceuticals, has become available. Vonoprazan has several advantages including faster onset, greater potency, stability under acidic environment, and is less influenced by CYP2C19 when compared with the standard dose of PPI,45 which might have a potential benefit in treating H. pylori. A meta-analysis of 14 studies with 14 636 Japanese participants concluded that vonoprazan-based TT was superior to standard TT in first-line therapy, but not in second-line treatments.46 Second, we did not analyse the optimal composition, dose, or duration of probiotics when used as an adjuvant therapy in the treatment of second-line H. pylori eradication therapy. Thus, further investigation is warranted. Third, for randomised trials, some concerns were common in overall bias because of inadequate concealment and blindness of participants in most trials. There was no significant inconsistency except when using the side-splitting method for the comparisons between BQT-7 and QTT-10/14. Finally, few trials reported zero events when considering the dropout rate, which contributed to less precise estimation of patients’ adherence. However, a previous meta-analysis mostly described the tolerability of regimens narratively, and thus we adopted dropout rate due to loss of follow-up and adverse events during the follow-up period to address this issue objectively.
Conclusions
In this NMA, the overall efficacy of probiotics (during), probiotics (before), QST-10/12/14, QBQT-10/12/14, probiotics (after), BQT-10/14, and QTT-10/14 was superior to that of the other regimens when compared with BQT-7 in H. pylori second-line eradication therapy. The priority of second-line eradication regimens also ranked similarly in the subgroup analysis. Our NMA may be of value to clinicians as the findings suggest alternative treatment choices with potential benefit beyond the therapies recommended by guidelines in terms of local antibiotic resistance rate and tolerability.
Supplemental material
Acknowledgments
The authors acknowledge the contribution of the Evidence-based Practice and Policymaking Committee, Taichung Veterans General Hospital, Taichung, Taiwan. They also thank members of the Taiwan Acid-Related Disease and Microbiota Consortium for their valuable suggestions.
References
Footnotes
Contributors S-IS, Y-LC, Y-CT, and H-ZY designed the meta-analysis, with input from all listed authors. Y-LC, Y-CT, and S-IS contributed to data acquisition and drafted the article. Y-KT, S-IS, and Y-LC contributed to data analysis and interpretation. All authors performed critical revision of the manuscript and approved the final draft of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. The data supporting this meta-analysis are from previously reported studies and datasets, which have been cited and belong to deidentified participant data.