Article Text

Abstract
Objective We examined the risk of primary gastrointestinal cancers in women with breast cancer and compared this risk with that of the general population.
Design Using population-based Danish registries, we conducted a cohort study of women with incident non-metastatic breast cancer (1990–2017). We computed cumulative cancer incidences and standardised incidence ratios (SIRs).
Results Among 84 972 patients with breast cancer, we observed 2340 gastrointestinal cancers. After 20 years of follow-up, the cumulative incidence of gastrointestinal cancers was 4%, driven mainly by colon cancers. Only risk of stomach cancer was continually increased beyond 1 year following breast cancer. The SIR for colon cancer was neutral during 2–5 years of follow-up and approximately 1.2-fold increased thereafter. For cancer of the oesophagus, the SIR was increased only during 6–10 years. There was a weak association with pancreas cancer beyond 10 years. Between 1990–2006 and 2007–2017, the 1–10 years SIR estimate decreased and reached unity for upper gastrointestinal cancers (oesophagus, stomach, and small intestine). For lower gastrointestinal cancers (colon, rectum, and anal canal), the SIR estimate was increased only after 2007. No temporal effects were observed for the remaining gastrointestinal cancers. Treatment effects were negligible.
Conclusion Breast cancer survivors were at increased risk of oesophagus and stomach cancer, but only before 2007. The risk of colon cancer was increased, but only after 2007.
- cancer epidemiology
- gastrointestinal neoplasia
- screening
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
The number of breast cancer survivors is growing due to improvements in early cancer detection and treatment.
The long-term risk of new primary malignancies among patients with breast cancer may be increased due to cancer treatment and/or shared risk factors.
What are the new findings?
The risk of being diagnosed with oesophagus cancer and stomach cancer was higher for patients diagnosed with breast cancer before 2007 than for the general population, while in later years the risk approximated unity.
The opposite was observed for colon cancer, where the risk was increased only after 2007.
The absolute cancer risks were relatively low.
How might it impact on clinical practice in the foreseeable future?
Knowing and quantifying the risk of gastrointestinal cancers among patients with breast cancer are of major public interest to substantiate and possibly refine guideline recommendations.
The observed low absolute risks support that extensive screening strategies to detect more gastrointestinal cancers is not indicated among patients with breast cancer.
Background
Breast cancer is the most frequently diagnosed cancer among women in Western and Asian countries. It constitutes approximately one-third of all newly diagnosed tumours in women.1 Because of the establishment of screening programmes for breast cancer with early detection and improvements in treatments, the mortality rates of breast cancer have decreased in most Western societies.2–4
Given the rise in prevalence of long-term survivors of breast cancer, concerns exist that the different treatment modalities have contributed to the development of new primary cancers. Endocrine therapy has been a cornerstone treatment in oestrogen receptor positive breast cancer and may interfere with several sites in the gastrointestinal tract with endocrine function. Radiotherapy may induce cancer in sites in close proximity to the breasts, that is, the pharynx, oesophagus, and gastric ventricle.5 6
Previous studies examined the risk of new primary gastrointestinal malignancies among patients with breast cancer.5–15 Notwithstanding, studies were limited by follow-up periods (<10 years),5 9 11 13 15 lacked data on human epidermal growth factor receptor 2 (HER2) status,5–15 and few studies covered all types of gastrointestinal cancers.10 12 Many studies also included patients with breast cancer diagnosed before 2007,7–15 the year when tamoxifen was replaced by aromatase inhibitors in postmenopausal women with estrogen-receptor-positive breast cancer. Because the treatment of breast cancer has changed considerably over the past decades, and because some studies reported contradictory findings, it is necessary to revisit earlier findings. Such data are needed to guide follow-up programmes of these patients. Therefore, we performed a population-based cohort study of risks of new primary gastrointestinal cancers among patients with an incident breast cancer, compared with risks in the general population. We also evaluated whether the associations varied by time periods and treatment regimens.
Methods
Setting and design
This nationwide population-based cohort study was conducted in Denmark, which has a population of 5.8 million inhabitants.16 The national healthcare system is tax supported, ensuring unfettered access to general practitioners and hospitals for all Danish inhabitants, including care for patients with cancer.17 Accurate linkage of all registries at the individual level is possible in Denmark owing to the unique central personal registry number assigned to each Danish inhabitant at birth and to residents on immigration.17
Patients with breast cancer
All women≥18 years of age diagnosed with incident localised or regional spread breast cancer between 1 January 1990 and 31 December 2017 were identified using the Danish Cancer Registry (DCR).18 The DCR contains detailed data, including cancer stage, on prospectively recorded incident cancers diagnosed in Denmark since 1943. All incident cases of cancer in Denmark have been reported to the DCR from all clinical departments and departments of pathology and forensic medicine. From 2004 onwards, reporting to the registry became electronic and administered by the Danish National Patient Registry (DNPR). Tumours have been classified according to the International Classification of Diseases, Tenth Revision and the International Classification of Diseases for Oncology, Third Edition since 1978. Routinely scheduled quality control is performed, ensuring a high degree of completeness and validity of the registry with 95%–98% completeness and accuracy of recorded diagnoses.18
We excluded patients with a history of cancer at any time before their hospital contact for breast cancer to ensure that cases of breast cancer and cancer outcomes both were incident. Data were retrieved on oestrogen receptor and HER2 receptor status from the Patobank,19 which is a nationwide Danish registry of all pathology specimens analysed since 1996. Data on breast cancer treatments were retrieved from DCR until end of 2003 and from the DNPR since 200420 (including radiotherapy, chemotherapy, tamoxifen therapy, aromatase inhibitor treatment, lumpectomy, and mastectomy). Data on lumpectomy and mastectomy were obtained from the DNPR and restricted to 1996 onwards due to data registration limitations.
Gastrointestinal cancers
We searched the DCR to identify any subsequent gastrointestinal cancer after the diagnosis of breast cancer. Gastrointestinal cancers included cancers of the oesophagus, stomach, small intestine, colon (including rectosigmoid colon), rectum, anal canal, liver, gallbladder and biliary tract, and pancreas. We also classified the cancers into upper gastrointestinal cancers (oesophagus, stomach, and small intestine), lower gastrointestinal cancers (colon, rectum, and anal), and other gastrointestinal cancers (liver, gallbladder and biliary tract, and pancreas). To avoid bias due to heightened diagnostic workup, we focused on 1-year breast cancer survivors in the main analysis and subgroup analyses. To examine potential temporal trends, we also stratified the main analysis by calendar time period (1990–2006 and 2007–2017). In this analysis, we restricted follow-up to 10 years. All codes used in the study are in online supplementary tables 1 and 2.
Supplemental material
Statistical analysis
The breast cancer cohort was characterised by median follow-up time, age group (18–49, 50–59, 60–69, ≥70 years), calendar year period of breast cancer diagnosis with cutpoints selected according to the 2007 introduction of aromatase inhibitors in Denmark (1990–2006 and 2007–2017),21 oestrogen receptor and HER2 receptor status, and breast cancer treatment within the first year after breast cancer diagnosis (radiotherapy, chemotherapy, tamoxifen therapy, aromatase inhibitor treatment, lumpectomy, and mastectomy). Additionally, patients were classified by Charlson Comorbidity Index scores (low, moderate, and severe comorbidity levels).22 Cumulative gastrointestinal cancer incidences during 20 years of follow-up after breast cancer diagnosis were computed and graphically presented using the cumulative incidence risk function, accounting for death as a competing risk.23 24 Incidence rates were calculated using the number of events divided by risk time. Associated 95% CIs were derived using a normal approximation (Wald interval),25 assuming a Poisson distribution.
To contextualise the risk of new gastrointestinal cancers among patients with breast cancer with the cancer risk of the general population, we calculated standardised incidence ratios (SIRs) as the observed number of cancers relative to the expected number, based on national incidence rates by age in 5-year intervals, and by calendar period in 5-year intervals.26 As the SIR estimates were calculated using indirect standardisation, they were not directly comparable to each other. Corresponding 95% CIs were derived using Byar’s approximation, assuming that the observed number of cases in a specific category followed a Poisson distribution. We used exact 95% CIs when the observed number of cancers was less than ten.27 Multiplying the number of person years of observation by national incidence rates yielded the number of cancer cases that would be expected if patients with breast cancer had the same risk of cancer as the general population. In SIR analyses, follow-up began 1 year after their hospital contact date for breast cancer, while follow-up ended at occurrence of a primary gastrointestinal cancer diagnosis, emigration, death, or 31 December 2017, whichever came first.
As a complement, we also evaluated the impact of different patient characteristics and treatment regimens during the first year following breast cancer on the subsequent risk of gastrointestinal cancers. To avoid conditioning on the future28 and the risk of detection bias, follow-up was started 1 year after the breast cancer diagnosis (consistent with the main analysis), excluding patients with gastro-oesophageal cancer events or death within the first year. In these analyses, patient characteristics included breast cancer stage, oestrogen receptor and HER2 receptor status, age groups, and treatment regimens included radiotherapy, chemotherapy, tamoxifen therapy, aromatase inhibitor treatment, lumpectomy, mastectomy. These subgroup analyses were performed for the main cancer groups only (ie, upper, lower, and other gastrointestinal cancers) to retain precise effect estimates.
To allow a minimum of 2 years of follow-up for all patients, we performed a sensitivity analysis, restricting the study population to 1 January 1990 and 31 December 2015.
Statistical analyses were performed using SAS, V.9.4 (SAS Institute). In Denmark, registry-based research does not require approval from an ethics committee or informed consent from patients.
Results
The cohort comprised 84 972 patients with a first-time breast cancer diagnosis (table 1). The patients were equally distributed across age categories. Breast cancer stage was localised in 58% of the patients, and 60% were oestrogen receptor positive. The majority of patients had a low Charlson Comorbidity Index score (81%).
Characteristics of patients with breast cancer, Denmark, 1990–2017
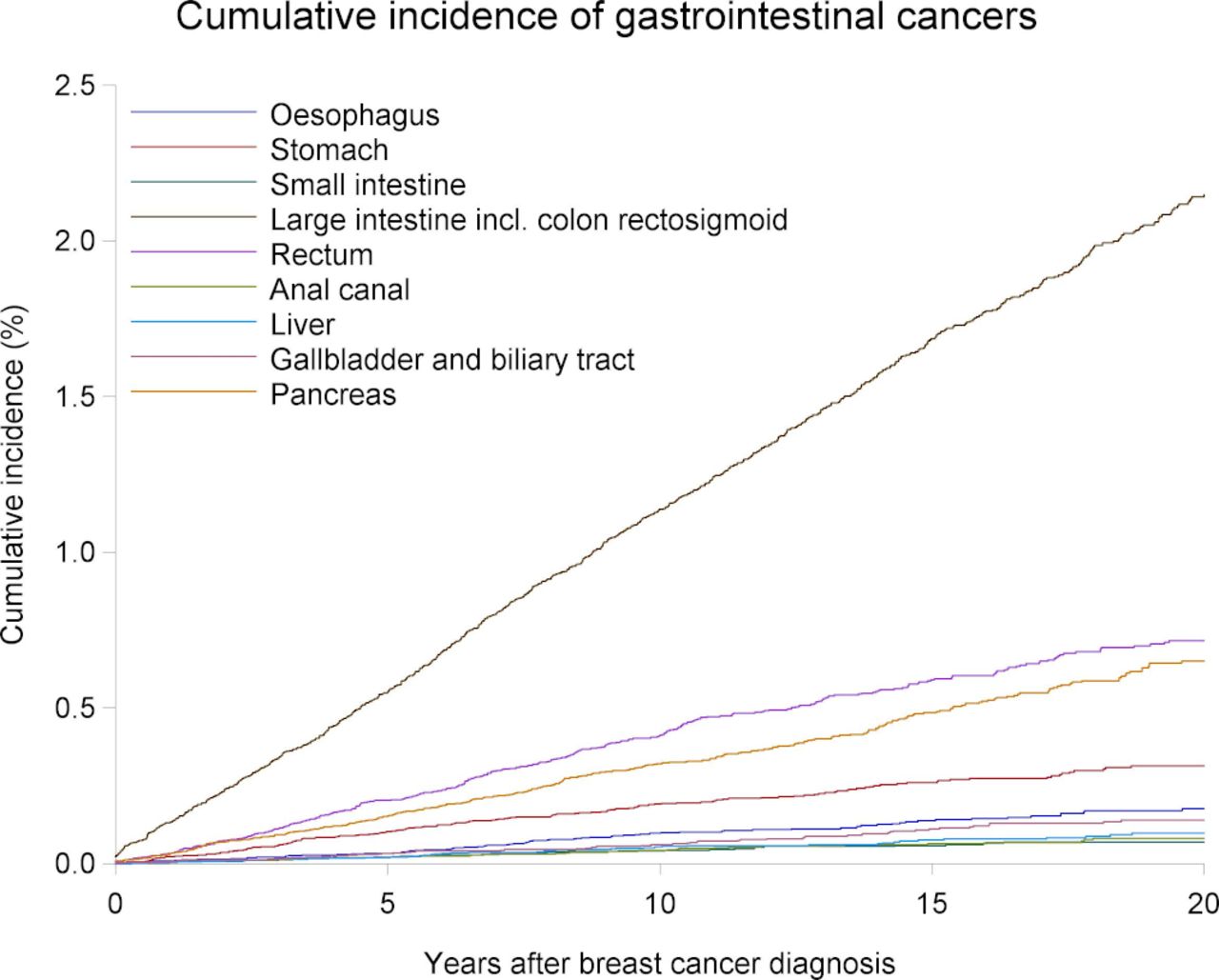
During the 28 years of follow-up (median, 7.4 years), 2340 incident gastrointestinal cancers were diagnosed among patients with breast cancer. The cumulative incidence of gastrointestinal cancers after 1 and 20 years of follow-up was 0.26% and 4.40% (0.01% and 0.18% for oesophagus cancer, 0.02% and 0.31% for stomach cancer, 0.01% and 0.07% for small intestine cancer, 0.13% and 2.15% for colon cancer, 0.03% and 0.72% for rectum cancer, 0.01% and 0.08% for anal canal cancer, 0.00% and 0.10% for liver cancer, 0.01% and 0.14% for gallbladder and biliary tract cancer, and 0.03% and 0.65% for pancreas cancer; figure 1). The incidence rate per 100 000 person years was increasing slightly during follow-up for any gastrointestinal cancers (319 during +1 years, 249 during 2–5 years, 336 during 6–10 years, and 398 beyond 10 years of follow-up; table 2). The SIR for cancer of the stomach was increased approximately 1.5-fold during 2–5 year of follow-up (1.48, 95% CI 1.13 to 1.90) and 6–10 years of follow-up (1.43, 95% CI 1.06 to 1.88), after which it was moderately elevated at 1.2-fold. The SIR for cancer of the colon was neutral during 2–5 years of follow-up, and approximately 1.2-fold increased beyond 5 years of follow-up (table 2). The excess risk of colon cancer was mainly driven by localised cancer (+1 year SIR estimates were 1.20, 95% CI 1.09 to 1.33 for localised colon cancer, 1.08, 95% CI 0.94 to 1.23 for regional spread disease, and 1.06, 95% CI 0.93 to 1.21 for distant stage cancer). For cancer of the oesophagus, the SIR was increased only during 6–10 years (1.55, 95% CI 1.10 to 2.13). While there was a weak association with pancreas cancer beyond 10 years after breast cancer diagnosis, the risks of the remaining gastrointestinal cancers were not appreciably increased at any point during follow-up.

{kind=link}
Cumulative incidence of gastrointestinal cancers after a breast cancer diagnosis during 20 years of follow-up.
Risk of selected site-specific gastrointestinal cancers in patients with breast cancer (1990–2017), by follow-up periods
Time-trend analyses revealed that the risk was higher than expected for lower gastrointestinal cancers, particularly colon cancer, but only after 2007 (SIR=1.21, 95% CI 1.09 to 1.34; table 3). The opposite trend was observed for upper gastrointestinal cancers, where the SIR was increased during the first part of the study (1.42, 95% CI 1.19 to 1.68). The remaining outcomes were largely unaffected by calendar period stratification.
Risk of selected site-specific gastrointestinal cancers in patients with breast cancer (1990–2017), by calendar periods
Additional analyses
In age-stratified analyses, the association was attenuated with increasing age for all subtypes of gastrointestinal cancer (table 4). This pattern was especially pronounced for upper gastrointestinal cancers. No substantial difference in risk of secondary cancers was observed for localised and regional breast cancer stages with the exception of upper gastrointestinal cancers where the SIRs were 1.52 (95% CI 1.27 to 1.81) for regionally advanced breast cancer and 1.09 (95% CI 0.93 to 1.28) for localised breast cancer. When stratifying by oestrogen receptor status, the SIRs were not substantially affected for any outcome. The SIR of lower gastrointestinal cancers was elevated among HER2 positive patients, but not substantially for HER2 negative patients.
Risk of gastrointestinal cancers among 1-year patients with breast cancer, by subgroups
In analyses stratified by treatment during the first year after the breast cancer diagnosis, the SIR was largely unaffected by radiotherapy, chemotherapy, and tamoxifen therapy for all outcomes (table 5). We observed no impact of lumpectomy or mastectomy on the risk of secondary gastrointestinal cancers. Due to sparse data, estimates were inconclusive for patients receiving aromatase inhibitor treatment. The sensitivity analyses allowing a minimum of 2 years of follow-up revealed estimates consistent with the main analysis (data not shown).
Risk of gastrointestinal cancers in patients with breast cancer, by treatment during the first year after breast cancer diagnosis
Discussion
In this Danish population-based study, patients with breast cancer had slightly higher than expected long-term risk (<10 years) of cancers of the oesophagus, stomach, and colon, but not other gastrointestinal cancers compared with risks in the general population. The associations were strongest for stomach cancer. Our analyses focusing on temporality showed that the risk of upper gastrointestinal cancer was only increased before 2007, while the risk of lower gastrointestinal cancer only was increased after 2007. The associations were generally stronger in younger versus elderly patients. No substantial treatment effects were observed for patients treated with radiotherapy, chemotherapy, tamoxifen, lumpectomy or mastectomy and there was no difference in subgroups of patients with oestrogen receptor positive breast cancer.
In the present study, we confirmed the findings of a previous study of 525 527 patients with breast cancer from 13 European countries, suggesting a higher than expected long-term (1–9 years) risk of new-onset oesophageal cancer (1.3–2.1-fold), stomach cancer (1.3–1.5-fold), and colorectal cancer (1.2–1.3 fold) among patients with breast cancer.10 Further, our data largely confirmed the findings of a Dutch study of 58 068 patients with invasive breast cancer (1989–2003), which reported increased risks for oesophagus cancer (1.6-fold), stomach cancer (1.3-fold), colorectal cancers (1.1–1.3-fold), but not other gastrointestinal cancers (pancreas and gall bladder).12 The same pattern for colorectal cancer and pancreas cancer was found in the European Prospective Investigation into Cancer and Nutrition cohort.14 In contrast to our findings, two studies of 1-year breast cancer survivors recorded in the Danish Breast Cancer Cooperative Group (DBCG) during 1977–200111 did not report any substantial increased risk for oesophagus cancer, stomach cancer, colon cancer, or other types of gastrointestinal cancers. Other studies from Taiwan,5 USA,15 and France8 reported data with no substantial association between breast cancer and gastrointestinal cancers overall.
Few studies examined the impact of various treatment modalities on the risk of gastrointestinal cancers following a breast cancer diagnosis, yielding somewhat conflicting results.6 9 13 In many of these studies, relatively few gastrointestinal cancer outcomes occurred across the different exposure/treatment groups, resulting in imprecise effect estimates and thus difficulties in drawing meaningful conclusions. Based on data from the Osaka Cancer Registry in Japan (1973–2003),13 recent data from the DBCG,6 and our study, radiation therapy was linked to an increased risk of mainly stomach cancer. A Japanese study found increased risk of stomach cancer among tamoxifen-treated patients, but not among non-tamoxifen-treated patients—a finding which could not be confirmed in our analysis. Studies on chemotherapy and subsequent risk of gastrointestinal cancers are sparse, heterogeneous and not directly comparable to our findings.
The mechanisms by which breast cancer are associated with some but not all gastrointestinal cancers are probably complex and multifactorial. Cancers potentially attributable to local radiotherapy for breast cancer include oesophagus and stomach cancer due to the close proximity to the breasts. Radiation therapy has become increasingly targeted during the past decades, and thus less likely to affect tissues surrounding the breast. This may explain why the associations observed in our study tapered off in the last part of the study period, in contrast to previous studies.10 In Denmark, the national breast cancer screening programme was launched in 2007. Consequently, a larger proportion of women diagnosed in the late study period rather than the early study period likely were patients with localised disease. These patients require less extensive cancer treatment, and this mechanism may contribute to our findings.
It is also possible that breast cancer and some gastrointestinal cancers are independent cancers driven by shared genetic mutations, but with a longer latency period for gastrointestinal cancers. For example, HER2 overexpression is increasingly recognised as a molecular abnormality involved in the pathogenesis of gastric and oesophageal cancers.29 Similarly, a recent study of patients with Lynch syndrome reported a markedly higher risk of breast cancer among MSH2 mutation carriers than in the general Canadian population, suggesting a link between colorectal cancer and breast cancer.30 Beyond breast and ovarian cancers, it has previously been proposed that mutations in the BRCA1 and BRCA2 genes increase risks for pancreatic cancer. This potential association was not apparent in other studies,10 12 14 but cannot be ruled out based on our observations. In addition, clear patterns have emerged that alcohol consumption is linked to both breast cancer and many other types of cancer, including gastrointestinal cancers.31 As opposed to this, use of non-steroidal anti-inflammatory drugs, which is commonly used among patients with breast cancer, may have reduced the risk of some new primary gastrointestinal cancers, for example, colorectal cancer.32 Importantly, we showed that the SIR was moderately increased for colon cancer after 2007. A national population-based screening programme for colon cancer was implemented in Denmark in 2014. This could have affected our estimates if breast cancer survivors were more likely to participate in the screening programmes and opportunistic screening than individuals in the general population. Oestrogen pathways may be involved in the development of colon cancer,33 and therefore the introduction of aromatase inhibitors may, at least partly, contribute to our findings, although a recent study did not report an association between use of aromatase inhibitors and colon cancer.34
Knowing and quantifying the risk of gastrointestinal cancers among patients with breast cancer are of major public interest to substantiate and possibly refine guideline recommendations. Although our analysis suggested slightly elevated SIR estimates, the cumulative risk of cancer was relatively low, with highest risk observed for colon cancer. It was not an objective of our study to determine whether patients with breast cancer would benefit from additional screening, for example, colonoscopy, but the low absolute risks support that extensive screening strategies to detect more gastrointestinal cancers are not indicated.
Our analysis was based on detailed population-based data with long-term complete follow-up in a uniform healthcare system. Thus, our results are less prone to selection bias, stemming from inclusion of specific study participants or informative loss to follow-up. Limitations should also be addressed. The relatively low number of rare gastrointestinal cancer events prohibits drawing firm conclusions in some of the subgroup analyses. Although we had several detailed clinical data, we had some missing data issues (eg, HER2 status) and lacked data on some variables (eg, life style factors). The accuracy and completeness of cancer diagnoses are high in the DCR,18 although the breast cancer diagnosis has not been validated.
Conclusion
In this study, the risk of being diagnosed with oesophagus cancer, stomach cancer, and colon cancer, but not other gastrointestinal cancers, was higher for patients with breast cancer than for the general population. The excess risk was most noteworthy for stomach cancer. Underlying explanations for these observations may include shared risk factors, surveillance and/or be related to cancer treatments. The risk of lower gastrointestinal cancers was negligible before 2007, but increased thereafter. For upper gastrointestinal cancers, the opposite pattern was observed.
References
Footnotes
Contributors HTS conceived the study idea. KA, JS, DCF, and HTS designed the study. KA and JS reviewed the literature, organised the writing, wrote initial drafts and directed the analyses which were carried out by DKF. All authors participated in the discussion and interpretation of the results. All authors critically revised the manuscript for intellectual content and approved the final version.
Funding This work was supported by Program for Clinical Research Infrastructure established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions.
Disclaimer The funding source had no role in the design, conduct, analysis, or reporting of the study.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Danish Data Protection Agency, record number (2016-051-000001).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Danish law does not allow researchers to share raw data or datasets which include individual-level data points from the registries with third parties.