Article Text

Abstract
Background The Netherlands has a low hepatitis C virus (HCV) prevalence, estimated at 0.16%. Previous studies have shown that up to 30% of the diagnosed HCV population in the Netherlands has been lost to follow-up (LTFU). Retrieval of these patients could halt progression of liver disease in infected patients, reduce the number of infected individuals and limit HCV transmission. Several regional Dutch retrieval projects have already been executed, which demonstrated that retrieval is feasible. Therefore, we initiated a nationwide retrieval project, aiming to achieve microelimination in previously diagnosed but LTFU patients with chronic HCV through retrieval.
Methods Laboratory records will be used to identify possible patients with chronic hepatitis C, defined as either a positive most recent HCV RNA or positive HCV antibodies without known RNA result. Reviewing patient records and obtaining current contact information from municipality databases will identify LTFU patients who are eligible for retrieval. These patients will be invited for outpatient clinic care. The primary outcome of the study is the total number of LTFU patients who have been successfully linked to care.
Discussion Hepatitis C ELimination In the NEtherlands (CELINE) is within the remit of WHO elimination targets and the Dutch National Hepatitis Plan. The methodology of CELINE is based on previously conducted regional retrieval projects and is designed to overcome some of their limitations. After ethical approval was obtained in 2018, the first centre initiated retrieval in 2018 and the project is expected to finish in 2021.
Trial registration number NCT04208035.
- hepatitis C
- HCV
- health service research
- antiviral therapy
- infectious disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Hepatitis C viral (HCV) infection is a major public health threat worldwide.1 It was estimated that 71 million individuals were chronically infected with HCV in 2015, causing 399 000 deaths annually.2 3 After the introduction of the highly effective direct-acting antivirals (DAAs), WHO adopted its Global Health Sector Strategy on viral hepatitis, setting the goal of global elimination of viral hepatitis as a public health threat by 2030.4 Since then, numerous countries have started to plan measures in order to comply with WHO goals.
The Netherlands has a low HCV prevalence, estimated at 0.16%.5 The population in the Netherlands is 17 million and annually, approximately 300 people die as a result of HCV infection.6 HCV infections are mainly restricted to high-risk populations such as people who (formerly) inject(ed) drugs (PWID), immigrants from HCV endemic countries, people living with HIV, men who have sex with men (MSM) using pre-exposure HIV prophylaxis (PrEP) and people with inherited bleeding disorders.7–11 In the Netherlands, the highest burden of HCV infection is among first-generation migrants.5 Various measures to reach HCV elimination are already in place in the Netherlands. First, blood donors and MSM (if HIV positive or using PreP) are screened regularly. Furthermore, harm reduction strategies are available for PWID (opioid substitution therapy, needle exchange programmes) and MSM (eg, NoMoreC,12 an initiative in Amsterdam to increase awareness and HCV testing). As of November 2015, unrestricted DAA access is available in the Netherlands.13 DAAs are fully reimbursed by Dutch healthcare insurance, with exception of the yearly obligatory deductible excess of €385. Healthcare insurance is obligated for people residing in the Netherlands. However, asylum seekers, prisoners and homeless people are unfortunately unable to file for insurance. Healthcare workers can in these cases request specific funding for DAA treatment, a lengthy and difficult process.
In 2016, a National Hepatitis Plan, including both hepatitis B and C, was developed, focusing on five key pillars of interest: (1) awareness and vaccination, (2) identification of infected persons, (3) diagnostics and treatment, (4) improving care organisation and surveillance, and (5) monitoring the disease landscape. The current study falls under the second pillar.14
Previous studies have shown that up to 30% of the diagnosed HCV population in the Netherlands has been lost to follow-up (LTFU).15–18 Retrieval of these patients could both halt further progression of liver disease in infected patients and reduce the number of infected individuals through treatment and cure. Additionally, reducing the number of infected individuals serves as secondary prevention, by preventing ongoing transmission (treatment as prevention). Several regional HCV retrieval projects have been executed in the Netherlands, which demonstrated that retrieval is feasible.15–17 Therefore, we initiated a nationwide retrieval project ‘Hepatitis C ELimination In the Netherlands: CELINE’, based on the best practice methodology of these regional projects.
CELINE aims to microeliminate chronic hepatitis C in LTFU patients in all hepatitis centres in the Netherlands by retrieving and relinking them to care. Whereas the previously executed regional retrieval efforts successfully relinked 15% of LTFU patients to care,15–18 we hypothesise that this optimised nationwide retrieval initiative could increase this number. Therefore, we aim to achieve a retrieval rate of 25% of patients LTFU and eligible for retrieval.
Methods and analysis
Study design
CELINE retrieval and re-evaluation efforts are part of regular care and serve no specific research purpose. Archived clinical data from retrieved patients will be collected and analysed for research purposes. Therefore, CELINE is considered a multicentre observational cohort study.
Setting
CELINE aims to cover all certified hepatitis treatment centres in the Netherlands. At the time of writing, there are 46 certified hospitals (both academic and non-academic), and names and location may be found at the website of the Netherlands Association for the Study of the Liver, which is constantly updated.19 Where possible, CELINE retrieval will be extended to other hospitals, Community Health Services, laboratories performing diagnostics for primary care and addiction centres. CELINE has started in 2018 and is scheduled to finish in 2021.
Study population
CELINE aims to retrieve all LTFU patients with (possible) chronic HCV in the Netherlands in the 15-year period prior to collection of data. LTFU is defined as the lack of a scheduled future outpatient care appointment. Possible chronic hepatitis C is defined as the presence of persistent viremia (positive HCV RNA) or a positive antibody test without a known HCV RNA test at the time of LTFU. Patients are excluded from retrieval if their current address is unknown, if they are currently not living in the Netherlands, if they do not have health insurance or if HCV treatment is not indicated due to comorbidity or a short-life expectancy. Patients under 18 years of age or unable or unwilling to give informed consent are not excluded from retrieval and may still be seen at the outpatient clinic. However, they will not be included in the core CELINE study.
Retrieval strategy
The retrieval strategy of CELINE consists of four phases (see figure 1). In the first phase, the identification phase, electronic laboratory records will be used to identify patients that are (possibly) currently infected with chronic hepatitis C. These laboratory records contain all HCV diagnostic tests (HCV RNA, HCV antibodies, immunoblots and HCV genotype) performed in the 15 years prior to start of data collection. This timeframe was chosen as healthcare providers are required by law to maintain their patient records for this period.20 However, daily practice varies, and therefore we aim to look back as far as possible. Subsequently, reviewing (electronic) patient records will exclude patients with a spontaneously cleared or cured infection, with severe comorbidity or limited life expectancy, those referred to another centre, still in outpatient care or patients who have been deceased. This results in a list of patients with a (possible) chronic HCV infection who are LTFU.
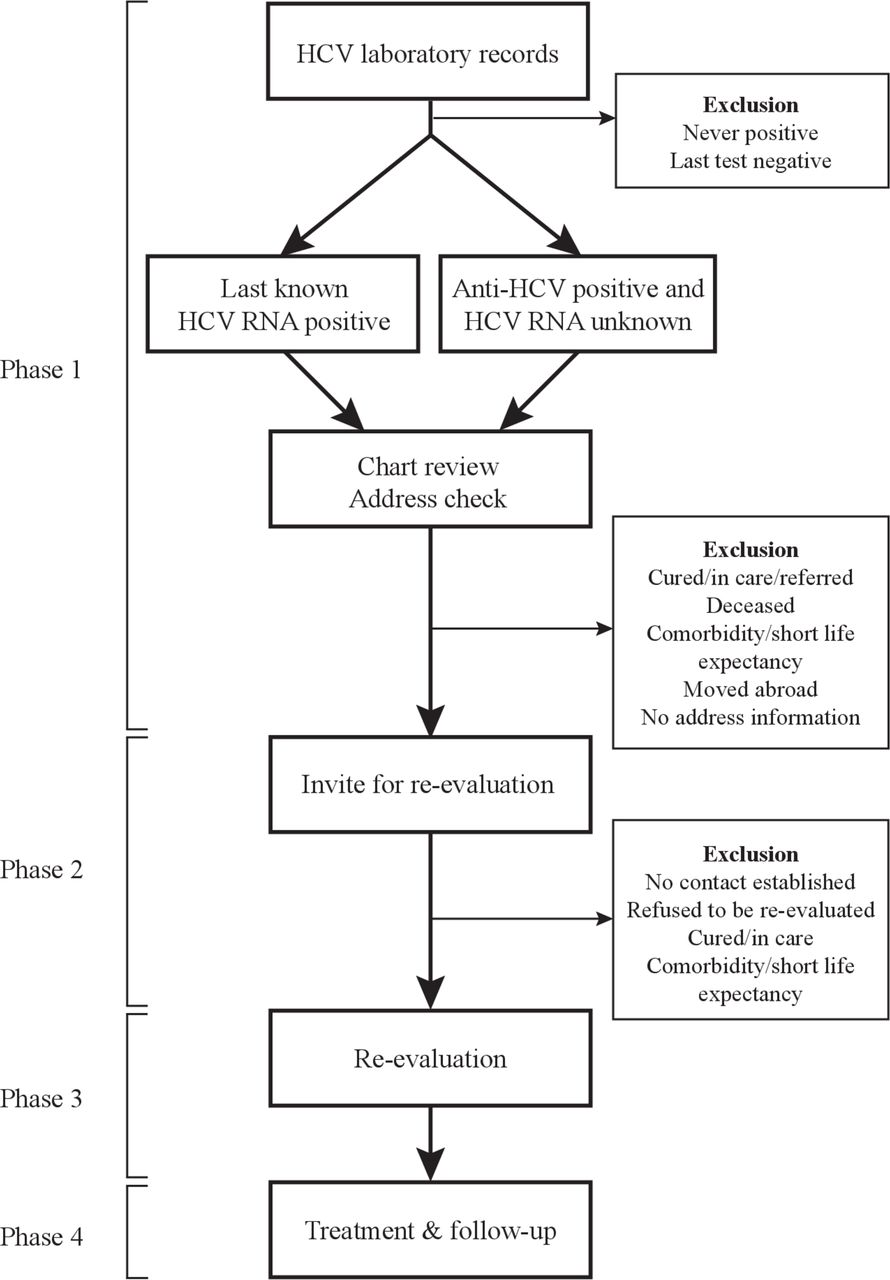
{kind=link}
CELINE retrieval strategy. HCV, hepatitis C virus.
The next step involves consultation with the Municipal Personal Records Database (in Dutch: Basisregistratie Personen) to determine whether a patient is alive and if so, where they are currently residing. If the hospital in question is not authorised nor able to obtain authorisation to access these records, these data will be collected by contacting the patient’s general practitioner’s (GP) office. All patients in the Netherlands are attached to a GP office that serves as a portal to wider healthcare options. Patients who are LTFU, alive and with available current address information are defined as eligible for retrieval.
In the second phase of CELINE, patients eligible for retrieval will be contacted by a letter that provides additional information about hepatitis C and the new treatment options. Patients will be invited for an outpatient clinic visit at a hepatitis centre close to their current residence. A reply card and return envelope will be enclosed with the letter in which a patient can explicitly give or withhold permission to be contacted by the researcher. If patients do not object, they will be contacted via telephone by the coordinating researcher approximately 2 weeks after receiving the letter. If patients do not wish to be contacted by the researcher, they can express this in the reply card, by telephone or via email. If we are unable to contact a patient after sending the letter, an attempt will be made to contact them via their GP or other concerned healthcare professionals.
The third phase is the core phase of CELINE and consists of re-evaluating retrieved patients. This outpatient clinic visit is part of regular care and thus covered by health insurance. Patients will be asked by their treating physician/nurse specialist to sign the informed consent form for approval of further data collection. Patients who do not give informed consent can still re-enter regular care, but no data will be collected for research purposes. These patients are however counted as ‘retrieved’.
The fourth phase of CELINE is treatment and follow-up. The physician will discuss the results of the performed tests and determine a suitable treatment and/or follow-up schedule, in accordance with current hepatitis C guidelines.21 The mandatory Dutch healthcare insurance fully reimburses DAA treatment, with exception of the obligatory deductible excess of €385 per year.
Study outcomes
The primary outcome of CELINE is the total number of LTFU patients who have been successfully linked to care. Linkage to care is defined as having had at least one visit at the outpatient clinic of a registered hepatitis centre.
Secondary outcomes are:
Total number of LTFU patients in the investigated time period.
Case ascertainment rate, defined as established contact (via telephone or in writing) with a patient who is eligible for retrieval.
Awareness of hepatitis C diagnosis among the LTFU patients.
Percentage of patients who never had an outpatient clinic appointment with a hepatologist or infectious disease specialist after initial positive HCV test.
Percentage of patients who are still viraemic (HCV RNA positive) at screening visit.
Following patient and disease characteristics of the retrieved patients: liver fibrosis stage, reasons for becoming LTFU, time since last HCV related hospital visit, mode of HCV transmission and treatment outcome.
When liver fibrosis stage is assessed with Fibroscan (Echosens, Paris, France), the following cut-off values are used: ≤7.0 kPa for F0-F1 (no or mild fibrosis); 7.1–9.4 kPa for F2 (moderate fibrosis); 9.5–12.4 kPa for F3 (advanced fibrosis); and ≥12.5 kPa for F4 (cirrhosis).22
Data collection
Data of invited LTFU patients will be stored in a password-protected Excel file on the internal server of the hospital in question. This data can only be accessed by the local investigator and will remain confidential. Data of LTFU patients who signed informed consent will be entered into the database by the coordinating researcher after the patient has signed the informed consent form. It includes data on patient and disease characteristics, such as comorbidities, alcohol and drug use, country of birth, date of diagnosis, mode of transmission, HCV genotype, HCV RNA level, complications of chronic liver disease (cirrhosis, portal hypertension, ascites, hepatic encephalopathy, varices/variceal bleeding and hepatocellular carcinoma) and treatment history. Furthermore, year of becoming LTFU, reason for LTFU, liver fibrosis stage according to Fibroscan, abdominal ultrasound results (organomegaly, portal vein characteristics, liver surface characteristics and presence of ascites or hepatocellular carcinoma) and laboratory results (haemoglobin, thrombocytes, international normalized ratio (INR), estimated glomerular filtration rate (eGFR), alanine transaminase (ALT), aspartate transaminase (AST), gamma-glutamyltransferase (GGT), alkaline phosphatase (ALP), total bilirubin, albumin) will be collected. Year of LTFU is defined as the year of the last HCV-related hospital visit or the last HCV blood test.
Data management
Collected data will be encrypted; every patient will receive a unique code, which will be used for all study related documents and materials. Only the local principal and coordinating investigators will have access to the local source file, in which the unique code is linked to personal data such as name, gender and date of birth. A validated and GCP compliant data management program, CastorEDC, will be used for data storage.
Statistical analysis
Descriptive data will be reported as either percentages, means (±SD) and medians (with IQR) when appropriate. Analyses will be performed using IBM SPSS Statistics V.25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, V.25.0).
Ethics and dissemination
Ethical approval
The Research Ethics Committee (in Dutch: Commissie Mensgebonden Onderzoek, CMO) Arnhem-Nijmegen has ruled that CELINE does not include the Medical Research Involving Human Subjects Act (in Dutch: Wet Medisch-wetenschappelijk Onderzoek met mensen, WMO), and a non-WMO declaration has been provided in 2018. Each participating hospital has to provide local approval before CELINE can be initiated. Patients will be asked informed consent for registration of their coded data in the CastorEDC database by a member of the treatment team. Participation is voluntary and will not influence standard clinical care. The Code of Conduct for the Use of Data in Health Research will be taken into account.23
Benefits and risks assessment
As a result of participation in this study, the LTFU population could benefit from re-entry into the regular healthcare system. If patients still have an indication for and want to receive treatment, they can participate with all the benefits of the current treatment regimes. Furthermore, CELINE serves a population benefit by adhering to the treatment as prevention paradigm (reducing the pool of infected people by treating them limits transmission of the disease). The minimal risks of this study (inconveniences of blood withdrawal, possibility of unexpected medical findings) do not outweigh this benefit.
Discussion
Even though effective treatment is available and fully reimbursed in the Netherlands, with the exception of the obligatory deductible fee mentioned previously, up to 30% of the diagnosed HCV population is LTFU.15–18 CELINE is a nationwide retrieval project which aims to achieve microelimination in previously diagnosed but LTFU patients with chronic HCV through retrieval and linkage to care. This project is within the remit of WHO elimination targets and the Dutch National Hepatitis Plan.4 14 24 The REtrieval And cure of Chronic Hepatitis C REACH) pilot study has shown that retrieval of LTFU patients with hepatitis C is feasible, although certain limitations accompanied the regional set-up of the study.18 We believe that the Netherlands is the right setting for CELINE due to the favourable HCV epidemiology and access to DAA treatment. In addition, the Netherlands has an excellent infrastructure and high quality of healthcare.
We believe that microelimination, the concept of applying elimination targets to specific subpopulations,25 is the preferred strategy for HCV elimination in countries with low HCV prevalence, such as the Netherlands.5 An important subpopulation for microelimination are patients who are LTFU, as they are already diagnosed and spontaneous clearance of chronic HCV is rare.26 Nonetheless, this population is rarely mentioned as a microelimination target population.25 27 This might be due to the fact that retrieval comes with many ethical and legal challenges, which we have described in detail elsewhere.20 By showing that retrieval is feasible and beneficial, we hope that CELINE can serve as an inspiration and a blueprint for other countries or regions to implement retrieval projects.
One of the strengths of CELINE is its methodology, which is based on several previously executed regional retrieval projects.15–18 These projects have shown that it is the best practice to identify LTFU patients by combining microbiology data with data from patient files. Medical microbiologists are allowed to share their data on HCV tests with hepatologists or infectious diseases specialists, since legally they are considered members of the treatment team.28 Such legal and ethical challenges have been described in detail elsewhere.20 The regional retrieval studies preceding CELINE have identified a number of (logistical) obstacles which could threaten the execution of the project. One of the issues was that researchers were not allowed to retrieve patients outside of their study region, which limited their efficiency substantially. Also, even when this was allowed, significantly fewer patients who had moved outside the region were willing to visit the original retrieving centre, most often because of the geographical distance.18 Another problem was that in some projects, physicians were not allowed to contact patients directly. They had to be contacted by their GP, which resulted in multiple barriers: (1) GPs in the Netherlands had to add another (unpaid) task to their already full agenda, which made response suboptimal, (2) many patients lacked updated GP information, which made it impossible to contact them at all and (3) most GPs are not HCV experts and therefore perhaps not fully equipped to adequately inform patients about treatment options. Therefore, within the remit of the CELINE project, patients are invited directly by the hospital physician, without direct interference of their GP. When a patient agrees to be re-evaluated, the GP is informed. We hypothesise that this simplification, together with the nationwide aspect of CELINE, will result in a better retrieval (25%) compared with earlier efforts (<15%).15–18
One limitation of the CELINE project, and also of hepatitis C elimination in the Netherlands in general, is the lack of a national hepatitis C database. Such a database is currently being established and its development might be facilitated due to the national collaboration network as is laid out through CELINE. Furthermore, not all hepatitis treatment centres have authorisation to obtain current address information from municipalities. Address information in these cases has to be obtained from GPs. Similar to regional projects, the current GP might be unknown. Moreover, even with up-to-date address information, patients who do not respond to the retrieval letter cannot always be contacted because of an unknown telephone number. Another limitation is that patients are not compensated for the payment of their yearly deductible excess fee of €385, which could result in patients refusing retrieval due to financial reasons. Finally, CELINE is a time-consuming project, which might make it difficult to translate to other healthcare environments that lack sufficient funding.
Relinkage to care will likely result in the patient being cured, which might prevent development or halt progression of liver disease. Furthermore, CELINE will result in a reduction of the pool of patients infected with HCV in the Netherlands, preventing further transmission. CELINE will also give insights into the hepatitis C cascade of care in the Netherlands. The project will provide numerous implications to improve patient care. An additional outcome of CELINE is a template for retrieval of LTFU patients with chronic hepatitis C that can be used and followed in other healthcare environments and/or countries.
To summarise, CELINE is a nationwide project that aims to retrieve and re-evaluate LTFU patients with chronic hepatitis C in the Netherlands. We aim to reduce liver disease burden for these patients and reduce further HCV transmission. The ultimate goal is to eliminate hepatitis C as a public health threat in the Netherlands, in accordance with WHO elimination targets.4 24
Trial status
After ethical approval was obtained in 2018, the first centre has initiated retrieval in 2018. So far, 14 centres have been included and 111 patients have been relinked to care. The study is still recruiting.
Acknowledgments
The HepNed study groups consists of: Janke Schinkel, Amsterdam UMC location AMC; Sophie B. Willemse, Amsterdam UMC location AMC; Bart van Hoek, LUMC; Dirk Posthouwer, MUMC; David Burger, Radboudumc; Hans Blokzijl, University Medical Centre Groningen; Karel J. van Erpecum, University Medical Centre Utrecht.
Footnotes
Twitter @MarleenvanDijk_, @mvdvalk, @jooparends, @joostphdrenth
Contributors All authors participated in design and execution of the study. CJI, SMB and MvD wrote the manuscript. MvdV, RJdK, JEA, JPHD, JS, BvH, DB and HB critically reviewed the manuscript.
Funding CELINE is supported with an unrestricted grant from Gilead Sciences.
Disclaimer Gilead Sciences does not have any role in study design, data collection, management, analysis and/or interpretation.
Competing interests CJI, SMB and MvD have no conflicts of interest. MvdV declares that the Amsterdam Infection & Immunity Institute Amsterdam UMC, on behalf of MvdV, received fees for participation in advisory boards of Abbvie, Gilead, Johnson & Johnson, Merck Sharp & Dohme (MSD), and ViiV and received independent research grants from Abbvie, Johnson & Johnson, Gilead, and MSD. RJdK declares that the Erasmus University Medical Centre, on behalf of RJdK, received honoraria for consulting/speaking from Gilead, Janssen-Cilag, Bristol-Myers Squibb (BMS), Abbvie, MSD, Roche, and Norgine and received research grants from Gilead, Janssen-Cilag, BMS, and Roche. JEA declares that the University Medical Centre Utrecht, on behalf of JEA, received honoraria for participation in advisory boards of Gilead, Janssen-Cilag, BMS, Abbvie, MSD, and ViiV and received research grants from BMS, Abbvie, and ViiV. JPHD declares that the Radboudumc, on behalf of JPHD, received honoraria or research grants from Novartis, Ipsen, Otsuka, Abbvie, and Gilead. JPHD served as consultant for Gilead and Abbvie, and in the last two years has been member of advisory boards of Otsuka, Norgine Gilead, BMS, Janssen, and Abbvie. JS participated in advisory boards of Gilead and received research grants from Gilead and Abbvie. SW has received honoraria for consulting/speaking from Gilead, Janssen-Cilag, BMS, and Roche, participated in advisory boards of Gilead, BMS, and Abbvie and received research grants from Gilead, Janssen-Cilag BMS, Abbvie, MSD, and Roche. BvH participated in advisory boards of Janssen-Cilag, BMS, Abbvie, MSD, and Norgine and received a research grant from Zambon Pharma. DP has no conflicts of interest to declare. DB has received honoraria for consulting/speaking from MSD, participated in advisory boards of MSD and received research grants from Gilead, Janssen-Cilag, BMS, MSD, and Roche. HB has participated in advisory boards of Gilead. KvE participated in advisory boards of Gilead, Janssen-Cilag, BMS, Abbvie, and MSD and received research grants from Gilead and Janssen-Cilag.
Patient consent for publication Not required.
Ethics approval Formal ethical approval was waived in 2018 by the Research Ethics Committee Arnhem-Nijmegen as they ruled that CELINE does not fall within the Medical Research Involving Human Subjects Act. Local approval is obtained in each participating centre.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Future data are available upon reasonable request from the corresponding author.