Article Text

Statistics from Altmetric.com
Summary box
What is already known about this subject?
Ulcerative colitis (UC) is associated with colorectal cancer (CRC).
The risk of CRC appears to have decreased in magnitude.
Clinical risk factors influence the risk and determine the frequency of surveillance.
What are the new findings?
The overall incidence of CRC was 1.6% in a prospective cohort at a 20-year follow-up of UC, the IBSEN 20 cohort.
The total lifetime risk of CRC was similar to the risk in the background population of Norway.
How might it impact on clinical practice in the foreseeable future?
The present study provides real-world knowledge on the risk of CRC in UC allowing us to update and improve surveillance strategies.
Introduction
The association between ulcerative colitis (UC) and colorectal cancer (CRC) is widely accepted although the magnitude of the risk seems to have decreased, according to recent studies.1 2 In 2014, an Australian study described a cumulative incidence of 1% at 10 years, 3% at 20 years and 7% at 30 years for CRC-UC.3 More recently, a population-based inception cohort study, the IBSEN study, described a twofold increased risk after 20 years for male patients with UC but no increase in risk for female patients with UC, compared with the background population.4
Several risk factors have been established and include cumulative inflammatory damage, severe and extensive inflammation, previous neoplasia in the colon, coexistence of primary sclerosing cholangitis (PSC), a history of first-degree relatives with CRC and male sex.5–12 In contrast, anti-inflammatory medication seems to be protective, probably as chronic inflammation contributes to the development of CRC.6 13 14 Colonoscopic surveillance is effective for the detection of CRC in UC patients with UC; however, the effect on survival is not established. Moreover, although decreasing in incidence in parallel with technical advances in endoscopy a significant number of patients develop interval cancer, indicating the need for more sensitive tools for risk assessment.15–17 This need is further emphasised by the rising incidence of UC, with the need for endoscopic surveillance due to disease flares or complications.18 19 More detailed knowledge on the specific effect of each risk factor could enable more precise and personalised surveillance.
Thus, the aim of the present study was to assess the association between selected clinical risk factors and CRC in a prospective population-based cohort of UC patients.
Material and methods
Study population
A population-based inception cohort of patients with inflammatory bowel disease (IBD), the IBSEN cohort, diagnosed with IBD from 1 January 1990 until 31 December 1993, has been prospectively followed at 1, 5, 10 and 20 years after diagnosis. The organisation of the cohort, diagnostic criteria for IBD and clinical follow-up protocol have been described in detail elsewhere.20 21All visits included a clinical examination, a structured interview and laboratory tests. Surveillance colonoscopies were performed according to guidelines in patients with PSC, history of CRC in first-degree relative or pseudopolyps. Colonoscopies were otherwise performed at local and referral hospitals when indicated clinically. Surveillance colonoscopy was not performed in the remaining patients as surveillance has not been found to be cost-effective and newer modalities time-consuming. Patients were followed closely and thus received adequate anti-inflammatory treatment.
A total of 517 patients were diagnosed with UC; half were men (51 %) and the median age at inclusion was 37.4 years (range: 4–88). A total of 10 patients were lost to follow-up during 20 years of follow-up. A total of 26 of 347 patients with left-sided colitis and a total of 31 of 170 patients with extensive colitis underwent colectomy.21 22
Data collection
All Norwegian citizens are assigned a unique digital identification number, which makes it possible to link data from several registries and enables highly reliable epidemiological research. All medical doctors in Norway are, by law, obliged to report new and suspected cancers to the Cancer Registry which contains detailed information on each case of cancer, thus ensuring completeness of approximately 99%. Cases of dysplasia are not recorded in the Cancer Registry of Norway.
The International Classification of Diseases, 10th Revision (ICD-10) is the standard diagnostic tool for epidemiology, clinical diagnosis and health management. All cases of malignant neoplasms of the colon, malignant neoplasms of the rectosigmoidal junction and malignant neoplasms of the rectum (C18-C20) recorded until January 2015 in the Cancer Registry of Norway were used in this study.
The interpretation and reporting of these data are the sole responsibility of the authors, and no endorsement by the Cancer Registry of Norway is intended, nor should it be inferred.
Data in this study were extracted from the enrolment, 1-year, 10-year and 20-year follow-up time points.
Ethics
The regional ethics committees and the Norwegian Data Inspectorate approved the study. Patient identity and record confidentiality were maintained according to guidelines from the Norwegian Ministry of Health. All patients signed an informed consent form. This study was conducted in accordance with the Declaration of Helsinki.
Patient and public involvement (PPI) statement
Indirect PPI
We did not directly include PPI in this study, but the database used in the study was developed with PPI and is updated by a committee that includes patient representatives.
Statistical analyses
Data were described with medians and ranges for continuous variables and counts with percentages for categorical variables. The age used in the analysis was age in years at the 20-year follow-up presentation.
Patients who developed CRC prior to UC diagnosis were not included in the statistical analysis.
Follow-up time was defined as the time from the date of diagnosis of UC to the date of CRC diagnosis, date of death, colectomy or end of follow-up which ever came first. The event was defined as the occurrence of CRC. The risk of having CRC was modelled using Cox proportional hazard regression and the results are expressed as HRs with 95% CIs. Variables tested in the univariate Cox models were gender, maximum extent of colitis at any time, duration and age at diagnosis of UC, coexisting PSC and first-degree relative with CRC. All tests were two-sided and p values <0.05 were considered statistically significant. All analyses were performed using SPSS V.24.
Results
Incidence of CRC at a 20-year follow-up
A total of 517 patients with UC were included in the study. The median time of follow-up in years was 20.4 (95% CI: 0.1 to 24.2) and IQR was 2.53.
The cumulative incidence of developing CRC was 1.6% (8/517) at a 20-year follow-up from the diagnosis of UC. The total lifetime risk of developing CRC either before or after the UC diagnosis was 2.3% (12/517) (figure 1).
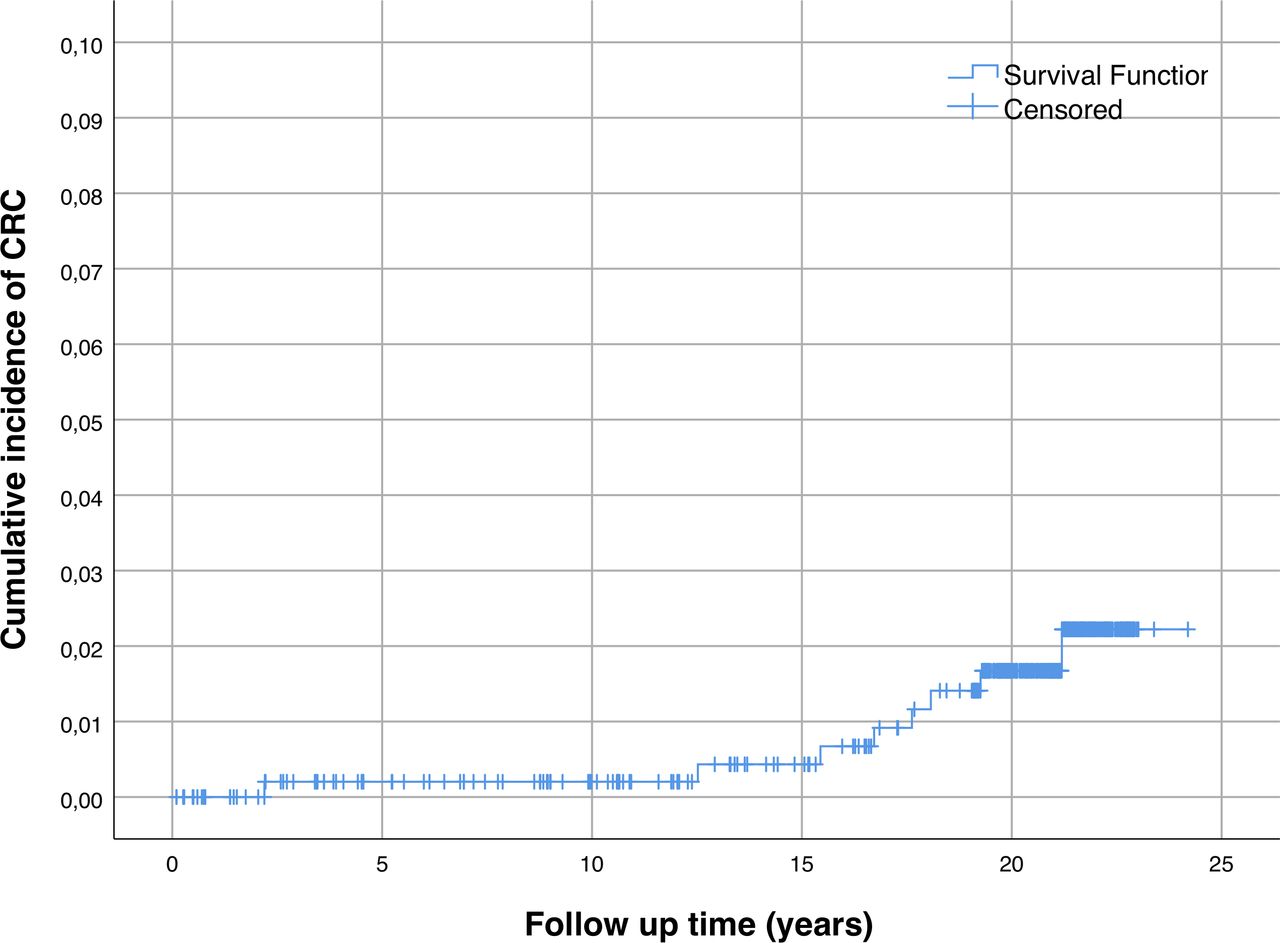
{kind=link}
Kaplan Meier curve with 95% confidence intervals showing the cumulative incidence of CRC by calendar period of follow-up
CRC was diagnosed ≥1 year after the UC diagnosis in a total of 8 of 517 patients (5/8 men), and the median age at CRC diagnosis was 56 (range: 39–88).
CRC was diagnosed prior to UC diagnosis in a total of 4 of 517 patients, all men with the median age at CRC diagnosis being 69 years (range: 64–79). These patients were not included in the risk analysis.
The clinical characteristics of all patients with UC are summarised in table 1.
Clinical characteristics of ulcerative colitis patients, n=517
Variables associated with risk of CRC
Only patients diagnosed with CRC after their UC diagnosis were included in the analyses presented below.
Older age at UC diagnosis was associated with higher risk of CRC. Patients aged above 70 at UC diagnosis had a 15-fold higher risk of CRC compared with those diagnosed aged below 40 years, HR 15.68 (95% CI: 1.31 to 187.92).
Neither sex, extent of colitis at any time nor concomitant PSC was associated with the risk of CRC.
Details concerning the selected risk factors and clinical characteristics of patients with CRC are summarised in tables 2 and 3.
Risk factors for colorectal cancer among patients with diagnosis of colorectal cancer after ulcerative colitis (n=8)
Clinical characteristics of patients with CRC prior to (n=4) and after UC diagnosis (n=8)
Discussion
In the present inception cohort study prospectively following 517 patients with UC, the overall cumulative incidence of developing CRC was 1.6% at a 20-year follow-up from the diagnosis of UC. The total lifetime risk of developing CRC either before or after the UC diagnosis was 2.3%. The present study is the first to prospectively follow an unselected cohort of patients with UC for 20 years and thus provide real-world data about the magnitude of CRC in UC. The overall incidence of CRC in UC is, to our knowledge, the lowest reported so far reflecting the population-based nature of the cohort. The St Mark’s surveillance tertiary centre cohort study found a cumulative incidence of 2.9% and 10% in patients with extensive UC at 20-year and 40-year follow-up, respectively.17 However, a cumulative incidence of 1% at 10 years, 3% at 20 years and 7% at 30 years for CRC-UC was reported in a cohort of 504 patients with UC with varying extent of colitis included from both tertiary and community-based healthcare centres.3
Interestingly, the overall risk of CRC in the present UC cohort was found to be slightly lower than the risk of sporadic CRC in Norway.23 The cumulative risk of CRC before the age of 75 years is reported to be 2.8% for women and 3.1% for men, ranking Norway as the country with fourth-highest rate in the world.23
The decrease in risk of CRC for patients with UC has been attributed to improved control of colonic inflammation by medication, appropriate follow-up with regular colonoscopies and technical advances with improved detection of early neoplastic lesions. At the time of the initiation of the present study, standard treatment strategies for UC were 5-ASA as maintenance therapy and prednisolone in cases of disease flares. However, treatment for steroid-refractory severe colitis was colectomy in this ‘pre-biologic’ era.24 Patients without PSC, history of CRC in first-degree relative or pseudopolyps did not undergo surveillance colonoscopy as surveillance is not systematically implemented in Norway and was thus not included in the protocol. All patients included in the study attended regular clinical follow-up including colonoscopy when indicated and optimisation of anti-inflammatory therapy. Thus, the low observed risk of CRC in the present study appears more likely to be attributed to participation in the present study with adequate control of inflammation than improved surveillance techniques. Similarly, a nationwide population study following 32 911 Danish patients with UC for 30 years found that the overall risk of CRC in UC was decreasing and comparable with the general population. Surveillance was not routinely implemented in Denmark at the time of the observation period (1979–2008) implying that the decline could not be attributed to superior surveillance procedures.1
Although the association between pseudopolyps and CRC remains debated, patients with a history of pseudopolyps underwent surveillance colonoscopy according to guidelines at the time of the study.25
Patients who had undergone colectomy were not included in the risk analysis. Colectomy was performed due to severe and extensive inflammation unresponsive to available medical treatment. Also, patients in whom high-grade dysplasia or multifocal neoplastic lesions were detected underwent colectomy. As previously described, colectomy may therefore be viewed as a ‘protective’ factor against CRC.26 Although younger patients are less prone to accept stoma than older patients, colectomy could be expected to be more frequent in younger persons due to more extensive and aggressive inflammation. In contrast, operators may be less willing to perform colectomy in older patients due to an increased risk of intraoperative and postoperative complications. However, the power of the study did not allow for the evaluation of competing risk so that the true risk of CRC may be underestimated.
All patients included in the study were referred to colonoscopy when indicated at scheduled clinical follow-up but did not undergo a systematic surveillance scheme. Colonoscopies were performed at local and referral hospitals and therefore recorded in records of several hospitals. Also, the Norwegian Cancer Registry does not include dysplasia. Thus, despite a rigorous approach, data regarding dysplasia are incomplete.
Based on the assumption that inflammation in UC is a prerequisite for the development of CRC, patients in whom CRC was diagnosed prior to UC were not included in the risk analyses. These cases may due to previously undiagnosed UC or due to differential diagnostic challenges by which the diagnosis of UC was delayed due to the presence of CRC.
Previous studies have similarly excluded CRC diagnosed within 1 year of IBD.1
In the present study, the observed median age of CRC in patients with CRC diagnosed after UC (56 years (39-88)) was in line with previous reports for CRC-UC.7 27 However, the median age of the four patients in whom CRC was diagnosed prior to UC was comparable with the reported median age for sporadic CRC (73 years).23 These cases of CRC may in fact be a complication of undiagnosed UC. Accordingly, UC-CRC has been reported to occur around 17 years earlier than the median age (73 years) for sporadic CRC in the non-IBD population of Norway.28
We further observed that patients older than 70 years at diagnosis had a 15-fold higher risk of CRC compared with those diagnosed when younger than 40 years. However, the CI is wide so that these results must be considered with caution. Increasing age is in itself a risk factor for dysplasia and CRC, thus old age in itself rather than either longstanding IBD or elderly onset UC may have contributed to CRC in the patients in the present study. Although, little data are available for IBD diagnosed in the elderly, advancing age itself has not been found to increase the risk of IBD-CRC.29 Nevertheless, a study from 2009 suggested that the interval between colitis and CRC decreases with age and that higher age at onset of IBD may be related to a more aggressive CRC suggesting the need for earlier surveillance in elderly patients with IBD.30 The incidence of CRC in elderly patients with IBD is however low although these patients have been found to have a greater need for hospitalisation related to surveillance colonoscopy. One might consider individualised surveillance strategies in elderly patients.
The median duration of UC until the development of CRC was 22 (1-23) years, which is longer than previously described.31 A majority of the CRC cases in the present study occurred later than 8–10 years after diagnosis of the recommended surveillance colonoscopy thus supporting current practice.32 33
In the present cohort, males with UC were found to have a twofold increased risk of CRC when compared with the background population of Norway.4 In the present study, men did not appear to have a different risk of CRC 20 years after the diagnosis of UC compared with women with UC of the same duration.
A total of 15 UC patients with UC had PSC of whom 80% had extensive colitis.34 Although relatively few cases of CRC were observed, the high proportion of extensive colitis, both without and in combination with PSC, supported the previously reported increased risk of CRC. A case–control study of two large IBD cohorts has shown that the risk of colorectal neoplasm increased 6.9-fold with a concomitant diagnosis of PSC.35
In contrast to other studies, in our cohort, extensive colitis was not confirmed as a risk factor for UC-CRC.36 This could be due to a type-II error in this real-life cohort, but also to other factors such as high standard of follow-up and good compliance with anti-inflammatory medication.
A retrospective cohort study from 2012 included 700 patients with UC with extensive colitis in whom a total of six out of nine of the detected CRCs were located in the rectum. Moreover, 71.2% of advanced neoplasia was detected in rectum or sigmoid colon.37 In the present study, four out of the eight CRC cases detected after the diagnosis of UC were located in the rectum/distal colon. The limited number of patients with CRC, however, did not allow us to estimate the effect of location on the risk of CRC.
The use of the Norwegian National Cancer Registry to accurately detect CRC cases, and the prospective and longitudinal follow-up of a population-based inception cohort, are major strengths of the present study. Although the number of patients included was high, the occurrence of CRC was low, limiting the statistical power of analysis of risk factors for UC-CRC. Risk factors were therefore evaluated one by one in univariate analyses as the limited number of CRC cases did not allow any multiple regression modelling.
In conclusion, in this population-based inception cohort study, the risk of CRC after 20 years of UC was low and comparable with the risk of CRC in the background population of Norway. The patients in the present study did not undergo systematic colonoscopic surveillance but close clinical follow-up ensuring adequate anti-inflammatory therapy. Fortunately, the number of observed CRC cases was low. Thus, although CRC remains a significant concern in patients with UC, the present study supports the reported decrease of CRC in UC. The power of the study did not allow us to conclusively evaluate the association between CRC and previously established risk factors. However, we anticipate the number of CRC cases to increase with an even longer follow-up, thus allowing for a more precise estimation of the possible risk factors.
Acknowledgments
The authors thank all members of the Inflammatory Bowel South-East Norway (IBSEN) Study Group for participating in the study.
References
Footnotes
Contributors PK: acquisition of data, analysis and interpretation of data, drafting of the manuscript, revision of the manuscript. SB: critical revision of the manuscript for important intellectual content, study supervision. MC: statistical analysis, critical revision of the manuscript for important intellectual content. MLH, MH, GH-H, TB, OH, IK-M, ICS, NS, JJ: acquisition of data, critical revision of the manuscript for important intellectual content. ØH: acquisition of data, including data form Statistics Norway, Norwegian Causes of Death Registry and the Cancer Registry of Norway, critical revision of the manuscript for important intellectual content. IK-M: Acquisition of data, critical revision of the manuscript for important intellectual content. MHV: critical revision of the manuscript for important intellectual content, study supervision. BAM: study concept and design, critical revision of the manuscript for important intellectual content, study supervision.
Funding PK is employed and funded by the Lovisenberg Diaconal Hospital.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Deidentified participant data is available from https://orcid.org/0000-0002-5884-4543.