Article Text

Abstract
Objective To assess health-related quality of life in patients with non-dysplastic Barrett’s oesophagus (NDBO) and endoscopically treated dysplastic Barrett’s oesophagus (DBO).
Design This quantitative, self-administered questionnaire study was conducted across three National Health Service hospitals. Data were collected from three other cohorts; gastro-oesophageal reflux disease (GORD), colonic polyp surveillance and healthy individuals. Fisher’s exact and Spearman’s rank correlation tests were used for analysis. Propensity score matching adjusted for age, sex and comorbidities.
Results 687 participants were eligible for analysis (NDBO n=306, DBO n=49, GORD n=132, colonic polyps n=152 and healthy n=48). 53% of NDBO participants reported similarly high cancer worry, comparable to DBO (50%, p=0.933) and colonic polyp participants (51%, p=0.355). Less cancer worry was reported in GORD participants (43.4%, p=0.01 vs NDBO). NDBO participants reported anxiety in 15.8% and depression in 8.6% of cases, which was similar to the other disease cohorts. Moderate or severe heartburn or acid regurgitation was found in 11% and 10%, respectively, in the NDBO cohort, comparable to DBO participants (heartburn 2% p=0.172, acid regurgitation 4% p=0.31) but lower (better) than GORD participants (heartburn 31% p=<0.001, acid regurgitation 25% p=0.001). NDBO participants with moderate or severe GORD symptoms were associated with higher rates of anxiety (p=<0.001), depression (p=<0.001) and cancer worry (p=<0.001). NDBO patients appropriately perceiving their cancer risk as low had lower rates of cancer worry (p=<0.001).
Conclusion This study provides insight into the problems Barrett’s oesophagus patients may face. Future care pathways must be more patient focussed to address misconceptions of cancer risk, oesophageal cancer related worry and GORD symptom control.
- barrett’s oesophagus
- quality of life
- surveillance
- endoscopy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Health-related quality of life (HRQoL) assessment provides a valuable insight into disease impact at an individual and population level.
HRQoL is a well-recognised outcome measure for healthcare delivery and treatment efficacy.
The annual cancer conversion rate from non-dysplastic Barrett’s oesophagus (BO) to oesophageal adenocarcinoma is relatively low.
Few historical studies concerning HRQoL in BO are outdated and cannot be translated to current care pathways.
What are the new findings?
This study provides a valuable insight into the problems patients with BO may face and efficacy of current National Health Service BO care pathways.
Oesophageal cancer related worry in patients with non-dysplastic BO appears disproportional to their risk.
Oesophageal cancer related worry is comparable between non-dysplastic BO and treated dysplastic BO cohorts despite significant differences in actual risk.
Gastro-oesophageal reflux disease (GORD) symptom control is an important component of HRQoL with >10% non-dysplastic Barrett’s oesophagus patients reporting moderate-to-severe symptoms.
Poor symptom control and misconceptions of oesophageal cancer risk are associated with greater cancer specific worry.
How might it impact on clinical practice in the foreseeable future?
Future care pathways should be more patient focussed with greater reassurance and communication to address; misconceptions of cancer risk, GORD symptom control, oesophageal cancer specific worry.
This research highlights the key areas of interest for the development and validation of a dedicated BO Patient Reported Outcome Measure (PROM).
Introduction
The incidence of oesophageal adenocarcinoma (OAC) and its precursors, gastro-oesophageal reflux disease (GORD) and Barrett’s oesophagus (BO), are increasing.1 2 BO is a well-established, relatively low risk,3 precancerous diagnosis that requires long-term endoscopic surveillance as per multinational guidelines.4 5 Without early detection, OAC is often devastating in terms of prognosis.6 Considering the relatively low annual cancer conversion rate of BO to OAC, 0.33% in most recent meta-analysis,3 the majority of patients with BO will never develop OAC but must live with the burden of a precancerous label. Recent advances in endoscopic therapy (ET) for those who develop dysplasia or early OAC are increasingly effective with durable outcomes.7 However, these patients still face multiple endoscopic procedures, long-term surveillance and risk of disease recurrence.4 5 8 9 Little is known about how these diagnoses and care pathways affect patients health-related quality of life (HRQoL).
HRQoL ‘reflects physical, social and emotional attitudes and behaviours of an individual as they relate to their prior and current health state’.10 HRQoL is therefore a key outcome measure of healthcare delivery and treatment efficacy. Despite this, HRQoL assessment in many studies is poorly done or tokenistic.11 To date, there is no validated BO specific patient reported outcome measure. Past quantitative research has therefore used numerous instruments to capture the impacts of this precancerous disease. Significant reductions in generic (eg, SF-36 form) and disease specific (GORD or gastrointestinal) HRQoL scores have been reported. A prior literature review12 and qualitative research13 has identified key areas of interest when measuring HRQoL in BO patients. These include GORD symptom control, psychological effects (eg, anxiety and depression), worry of oesophageal cancer and burden of repeated surveillance endoscopies. The few historical studies concerning BO HRQoL are outdated and cannot be translated to current care pathways. Other limitations include underpowered samples, use of a single measurement tool or a lack of appreciation for confounding factors. Even less research has been conducted regarding the impact of dysplastic Barrett’s oesophagus (DBO).14–16 Therefore, the true prevalence of HRQoL detriments remains largely unknown. Quantitative assessment of HRQoL will provide a valuable insight into the problem’s patients may face, efficacy of current care and highlight areas future healthcare delivery can focus resources on. This study aimed to assess HRQoL in patients with non-dysplastic BO and endoscopically treated DBO compared with other common gastrointestinal disorders and healthy individuals.
Methods
This quantitative, multicentre, self-administered questionnaire study recruited from three National Health Service (NHS) hospitals within the North West of England two of which provide ET for DBO. Simultaneously, data were collected from three other cohorts including a prior diagnosis of GORD without BO, colonic polyps requiring surveillance and healthy individuals without comorbid disease. All participants were >18 years old with no upper age limit. Participants were recruited via postal invite or in person. In order to minimise any acute impact on their responses, postal invitations occurred at a time independent of endoscopy or outpatient appointment. Likewise, those recruited in person were instructed to complete the survey at home at a time independent (>4 weeks) of a hospital appointment. For further information relating to the participant groups and recruitment please see the online supplementary file.
Supplemental material
HRQoL instruments; scoring and data management
Based on previous qualitative research and literature review, the following self-administered instruments were included in the questionnaire.12 13 For further information on each HRQoL instrument, scoring and data management please see the online supplementary file.
The Short Form 36 (36 items, 8 domains)
The SF-36 measures generic HRQoL allowing comparison between different diseases and the general population.17 It is the most extensively used and validated generic measure across many populations.
The Cancer Worry Scale (6 Domains, 4-point Likert scale)
The Cancer Worry Scale (CWS) is designed to measure cancer specific worry and impact of worry on daily functioning.18 It has been successfully used in assessing fear of developing cancer or cancer recurrence in breast, ovarian and bowel cancer settings.19–21 The following score cut-offs, defined by Custers and colleagues, were adopted; <10 as negative, 10 to 11 as borderline and ≥12 as positive.22 This score was accompanied by an assessment of numerical and perceived risk of developing cancer using a 7-point Likert scale.
Hospital Anxiety and Depression Score (2 domains, 14 items, 4-point Likert scale)
The Hospital Anxiety and Depression Score (HADS) is the most extensively used and validated screening tool for anxiety and depression.23–25 The author proposed cut-off points for these scores were adopted; 0 to 7 suggests the absence of symptoms, 8 to 10 indicates the presence of symptoms to a moderate degree with doubtful cases, ≥11 indicates significant symptoms which correspond to confirmed cases.23 26
The Gastrointestinal Symptom Rating Scale (15 items, 5 domains, 4-point Likert scale)
This extensively used symptom specific score measures frequency, intensity, duration and impact on daily life. It can identify clinically important change and discriminates well between each domain, most markedly in reflux and indigestion.27 28 There is no defined score cut-offs.
Statistical analysis
HRQoL outcomes are multidimensional with no single identifiable endpoint. Therefore, our primary outcomes were each of the questionnaire subcategories. Fisher’s exact test was used to identify associations between diagnostic groups and questionnaire items.
Further analysis examined for differences in the questionnaire subdomains between the non-dysplastic Barrett’s oesophagus (NDBO) group and the other groups separately using the average treatment effects, after propensity scores were calculated to adjust for potential confounders. Within this analysis, individuals were matched over the estimated probability of being at the diagnostic group, called propensity score, adjusted for sex, age and number of comorbidities. The healthy cohort, who lack comorbidities, were adjusted for age and sex only.29 Thus, individuals with the same propensity score have similar baseline observed characteristics, that is, age, sex and comorbidities. A sensitivity analysis to ensure the results of propensity matching score were consistent was implemented using nearest neighbour matching, where the closest individuals were matched according to a predefined distance.30
Finally, Fisher’s exact and Spearman’s rank correlation tests were performed to examine for possible associations between variables, that is, test for association between reflux symptoms and worry of oesophageal cancer or HADS anxiety.
A p value of <0.05 was considered clinically significant. When interpreting SF-36 scores; mean scores for each domain were converted into norm-based scores, as per author guidance,31 with a p value <0.05 accompanied with a coefficient of +/−3 points considered clinically significant.31 For further information on SF-36 norm-based scoring please see the online supplementary file. All statistical analyses were performed using Stata V.15.32
Results
Response rates and demographics
Two thousand and seventy-five individuals were invited to participate across all groups with an overall response rate of 38.4% (see online supplementary figure 2.1-1). The relatively low response rate likely reflects the use of postal invitation and the length of the survey. Responder versus non-responder characteristics for the BO group can be seen in the online supplementary table 2.1-1. These data suggests the non-responder group have fewer comorbidities, however this may be due to differences in recording than a true difference between the groups. Comorbidities for the responders were self-reported and obtained via clinical coding databases whereas the non-responders were identified from coding alone. Participant demographics for all four groups is displayed in table 1 (further breakdown of comorbidity prevalence and subcategories can be found in the online supplementary table 2.1-2).
Participant demographics
Gastrointestinal Symptom Rating Scale. Moderate or severe symptoms (15 items)
Generic health-related quality of life (SF-36)
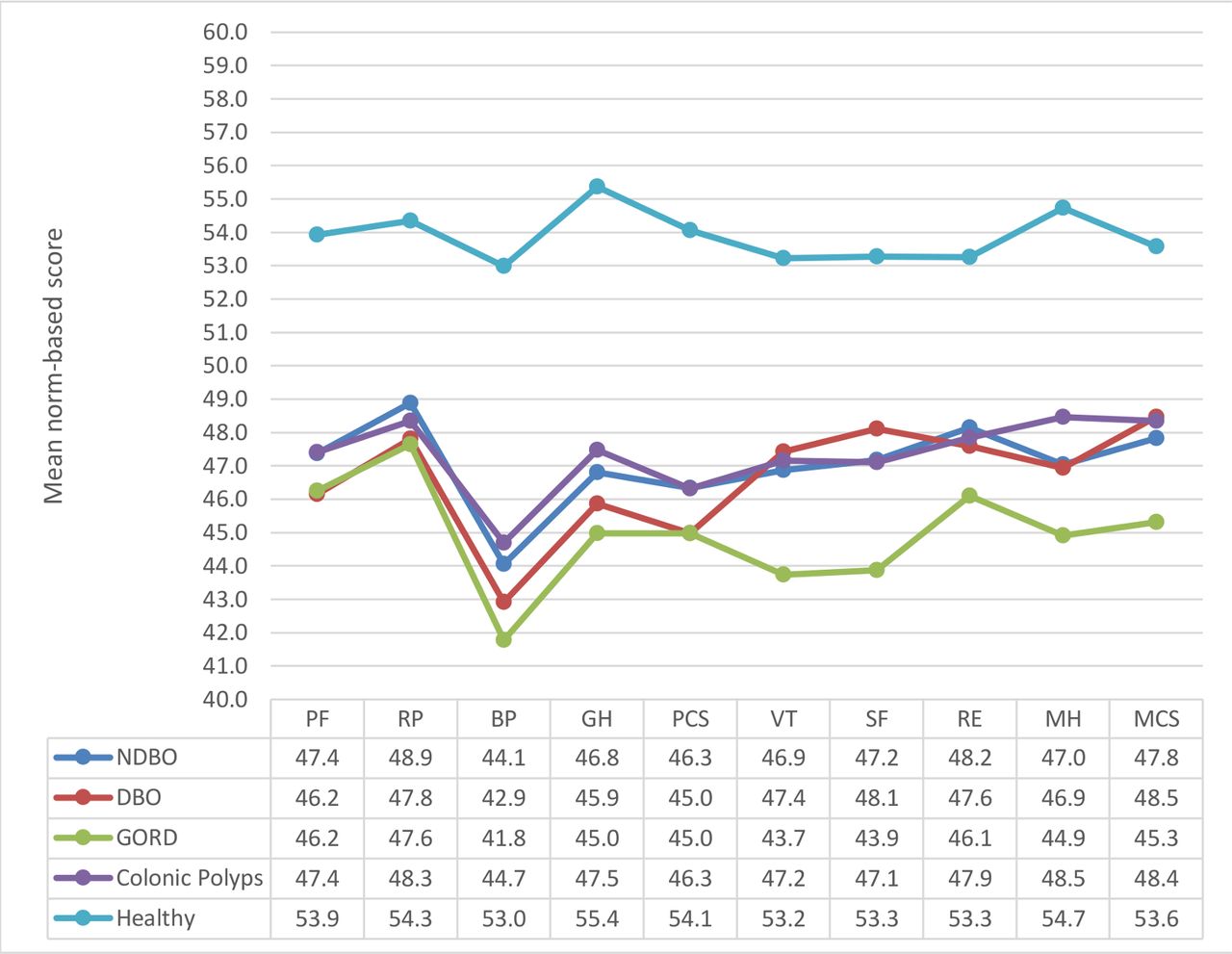
The mean norm-based scores, calculated against an age and sex matched UK population norm, are depicted in figure 1. The healthy cohort consistently scored at or above the UK general population norm in all domains. All disease groups showed detriments across the physical domains, in particular bodily pain, resulting in physical component summary scores below the population norm (BO=46.9, DBO=45.0, GORD=45.0 and colonic polyps=46.3). The GORD group were also below the general population average for all four mental health domains culminating in the only disease group to record an Mental Component Summary (MCS) score below average (GORD MCS=45.3) (figure 1).

{kind=link}
SF-36 norm based scores. Norm based scores give a direct comparison to a general population norm without having to cross reference to norm values. The scores for all groups have been age and sex matched to a prior UK general population norm. A score of 50 with a deviation of +/−3 points is considered comparable to the general population. Lower scores (<47) indicate worse HRQoL whereas higher scores (>53) indicate better HRQoL than the general population. BP, bodily pain; DBO, dysplastic Barrett’s oesophagus; GH, general health; GORD, gastro-oesophagealreflux disease; HRQoL, health-related quality of life; MCS,Mental Component Summary Score; MH, mental health; NDBO, non-dysplastic Barrett’s oesophagus; PCS, Physical Component Summary Score; PF, physical functioning; RE, role limitations emotional; RP, role limitations physical; SF, social functioning; VT, energy and vitality.
Although these data give an insight into generic HRQoL measures in relation to a previously published UK norm, it does not deliver any information to how the BO group compares in relation to the other cohorts and it remains unclear whether the generic HRQoL detriments seen here are due to the disease in question or other confounding factors such as comorbidities. In order to provide some insight into this, propensity score analysis was conducted where individuals of each diagnostic group were matched in regards to confounding factors and all groups were compared with the non-dysplastic BO cohort to look for significant differences in each domain. The non-dysplastic BO cohort had significantly lower (worse) scores across all domains compared with the healthy cohort. The BO cohort also had significantly higher (better) scores in the general health domain than the DBO cohort (coefficient=4.3, 95% CI=0.9 to 7.6, p=0.014). Otherwise the domain and summary scores were statistically comparable to all three disease groups. This suggests that initial observed differences in the mean scores between the groups may be related to confounders than the disease in question. For example, the BO cohort had mean scores >3 in both the energy and vitality and social functioning domains when compared with the GORD group. However, after propensity score matching analysis the coefficients were only +1.2 and +0.7, respectively, (online supplementary table 2.1-3 shows the coefficient, 95% CI and p values after propensity score matching for age, sex and comorbidities).
Gastrointestinal symptoms
The majority of the non-dysplastic BO cohort reported good reflux symptom control with 11% reporting moderate or severe heartburn and 10% reporting moderate or severe acid regurgitation. These rates were not statistically different to the treated DBO cohort. When compared with GORD patients, non-dysplastic BO participants had significantly better reflux control with 31.3% (p=<0.001) and 25.2% (p=0.001) of GORD participants reporting moderate-to-severe heartburn or acid regurgitation respectively (table 2). These findings were reproduced when comparing the two groups reflux domain score (combined heartburn and acid regurgitation items) with propensity score matching analysis (see online supplementary table 2.1-4). It was noteworthy that GORD participants also exhibited other significant gastrointestinal symptoms when compared with non-dysplastic BO participants, that is, increased nausea (p=<0.001), belching (p=p=<0.001), flatus (p=0.002) and harder stools (p=0.004). This finding is supported by a significantly greater gastrointestinal symptom total mean score after propensity score matching analysis (p=0.012) (see online supplementary table 2.1-4). As expected, the healthy cohort had significantly fewer gastrointestinal symptoms across all five domains and lower overall scores. Also, the colonic polyp patient group displayed significantly fewer upper gastrointestinal symptoms (abdominal pain p=0.006, reflux p=0.001 and indigestion p=0.047 domains) but were comparable in terms of lower gastrointestinal symptoms with the patients with non-dysplastic BO.
Cancer worry
A substantial proportion of non-dysplastic BO participants reported significant worry regarding oesophageal cancer with 53% recording positive and 17% borderline CWS. This finding was not significantly different to those treated for DBO (p=0.933) and participants undergoing colonic polyp surveillance (p=0.355) when questioned regarding colorectal cancer. GORD participants reported significantly less oesophageal cancer worry compared with non-dysplastic BO participants (p=0.01), however 43% still reported a positive CWS (table 3). This finding is despite 83% (n=109/132) of GORD participants having undergone a prior reassuring and relatively recent (mean 0.9 years.) gastroscopy. Healthy participants also reported high rates of worry (29%) when asked about cancer in general.
Cancer Worry Scale (total mean and categorical)
Cancer risk perception
The annual incidence of disease progression with BO is between 0.2% to 0.4% compared with that of disease recurrence in ET treated DBO of 1% to 2%.3 9 33 34 Based on this, the majority of the BO cohort either underestimated (43%) or overestimated (34%) their numerical 1-year risk, leaving only 22% who correctly chose either 0.2% to 0.4%. DBO participants tended to under (75%) rather than over (8%) estimate their numerical risk of disease recurrence with only 18% choosing appropriately (see online supplementary table 2.1-5).
However, an accurate understanding of numerical risk may not be important for patients or indeed correlate with their perception of risk. The corresponding items on the perceived risk scale show a greater percentage of BO and DBO patients who perceive their risk more accurately (32% in both groups). If ‘very small’ is also included in this calculation for non-dysplastic BO patients then this increases to 59% (n=169) of patients who selected the lower end of the scale and fundamentally perceive their risk as ‘small’. The result produced by the same calculation for the DBO group is comparable (n=27, 61%), suggesting they have a similar risk perception of OAC as patients who have never had dysplasia. Numerical and perceived risk scales correlated with each other across three of the five diagnostic groups (BO, DBO and colonic polyps).
The incidence of OAC in GORD is well established,35 36 although substantially lower than in BO cohorts. This study found many GORD patients worry about OAC (43.4%) with 10.6% perceiving their risk as large. Likewise, the incidence of colorectal cancer (CRC) in patients engaging in polyp surveillance in the UK is low (208/100 000 per year) and significantly reduced by surveillance. The risk in patients undergoing surveillance who lack high-risk features (eg, poor-quality colonoscopy, proximal polyps, high-grade dysplasia or adenoma >20 mm) may be comparable or lower to that of the general population.37 The majority of patients within this study’s cohort were either intermediate (57%) or low (26%) risk as per current national guideline definitions.38 Despite the known protective effects of adenoma surveillance, 13.8% of participants in this study perceived their risk as large with 51% reporting a positive Cancer Worry Score in relation to CRC.
Psychological impact
The prevalence of anxiety within the non-dysplastic BO cohort was 15.8% with a further 15.2% recording a borderline result. Rates of depression were lower (8.6% positive and 10.6% borderline) (table 4). Antidepressant usage was highest in the GORD group (18%) which is also reflected by the occurrence of mental health disorders which was highest in this cohort (33%) (see online supplementary table 2.1-2). One may therefore expect significantly higher rates of anxiety and depression in this group. However, all the disease groups were statistically comparable to the non-dysplastic BO cohort. Only the healthy group demonstrated significantly different scores with less anxiety (HADS A positive=4.2%, p=0.001) and depression (HADS D positive=0%, p=0.006). This finding was reproduced when the HADS mean scores (HADS A mean and HADS D mean) were compared after propensity score matching analysis (p=<0.001).
Hospital anxiety and depression scores
Correlation of measures
BO patients who reported moderate or severe GORD symptoms (heartburn, reflux) were associated with higher rates of both anxiety (p=<0.001, p=<0.001) and depression (p=<0.001, p=<0.001). Higher (worse) scores in the reflux domain (combined items) were also associated with higher (worse) Cancer Worry Scores (p=<0.001). Patients with higher cancer worry were associated with significant anxiety (p=<0.001) and depression (p=<0.001). Those who correctly perceived their cancer risk as low tended to have significantly lower rates of cancer worry (p=<0.001). This was also the case for numerical risk estimation (p=0.003).
Discussion
The major finding in this study was the high prevalence of OAC-related cancer worry among patients with non-dysplastic BO undergoing surveillance. It also appears that after ET for dysplasia or early OAC patient cancer specific worry is comparable to that of patients who have never had dysplasia. This finding is supported by the HRQoL data from the Ablation of Intestinal Metaplasia containing dysplasia (AIM) dysplasia trial.14 At 12 months follow-up, patients who had undergone successful radiofrequency ablation (RFA) for DBO reported significantly less worry than those who had received a sham procedure. Interestingly this was at a time when the true efficacy of ET was unknown. It therefore appears that informing patients they no longer have dysplasia or indeed BO is very reassuring to them. These findings need further delineation with a prospective paired pre and post treatment HRQoL study. The other study concerning cancer worry and DBO treatment was conducted by Rosmolen and colleagues.15 They compared oesophageal cancer worry of endoscopically treated high-grade dysplasia or early OAC to patients treated surgically in a single centre Netherlands study. Significantly higher levels of cancer worry were found in ET patients compared with surgically managed ones with similar disease stage. This may reflect the perceived risk of recurrence associated with having an intact oesophagus, especially when one considers the asymptomatic nature of disease progression. The payoff for lower levels of worry, in this surgical cohort, was significantly worse oesophageal and cancer related symptoms. This finding is supported by previous HRQoL data concerning oesophagectomy-treated patients.39 It must be noted however that this study was single centre, relatively underpowered and did not control for comorbidities. Interestingly, the authors also chose not to measure cancer worry, anxiety or depression in the non-dysplastic BO cohort as they did not expect these to be prevalent. Our study not only found prevalent oesophageal cancer worry in the non-dysplastic BO cohort but also high levels in GORD patients. This is despite a substantially lower relative risk and recent reassuring endoscopy in the majority of cases. Prior research estimates the incidence of OAC in males aged 65 years with daily reflux is 74.7/100 000 per annum. This risk drops off significantly below the age of 55 and is even lower in females. In fact, the risk of OAC in females with GORD is lower than that of males without GORD.35 Surprisingly the healthy cohort reported non-specific cancer worry in 29% or participants. This may reflect the finding that 50% of this cohort reported a family history of cancer and also the use of NHS staff as healthy volunteers. In previous studies healthcare staff have exhibited higher anxiety and depression rates when compared with the general population.40 41
The anxiety and depression scores found in this study are comparable to that reported by Cooper and colleagues in a previous UK BO cohort with mean HADS A scores of 5.5 (current study) and 6.1 (Cooper et al) and mean HADS D scores of 4.2 (current study) and 4.0 (Cooper et al).42 The incidence of combined abnormal and borderline cases were 31% versus 39% for anxiety and 19% versus 14% for depression, respectively.42 Subanalysis of the non-dysplastic BO cohort in this study, suggests that GORD symptom severity is associated with oesophageal cancer worry, anxiety and depression. The causality or direction of these associations cannot be concluded from this analysis alone. Yet, when interpreted alongside qualitative research, conducted by this research group, a greater understanding of these interactions can be achieved. This showed that, in some cases, GORD symptom flares lead to worry or anxiety regarding disease progression. Other factors also instigated in cancer worry included having dependents, an anxious predisposition and inadequate disease specific knowledge, particularly cancer risk perception.13 Indeed, perception of oesophageal cancer risk in this quantitative study correlated well with severity of cancer worry, as did numerical risk.
The data captured in this study suggest symptom control for the majority of BO patients is reasonable with approximately 10% reporting moderate-to-severe symptoms. Symptom severity is comparable to the DBO cohort, a finding consistent with that of Rosmolen and colleagues.15 GORD patients appear to have significantly worse symptoms, a finding supported by prior studies.43–45 There are a number of potential reasons for this. First, higher rates of PPI usage in non-dysplastic BO cohorts (95.1% vs 84.6% in this study). Second, a significant minority of BO patients are diagnosed incidentally and have never suffered GORD symptoms. Finally, GORD cohorts may also contain more participants with functional gastrointestinal disorders. This may be the case in this study as the GORD cohort reported significantly worse gastrointestinal symptoms outside the reflux domain. Also, of those who had undergone a recent endoscopy (109/132), 46% (n=50) had non-erosive disease, 32% (n=35) had reflux oesophagitis and 22% (n=24) had dyspepsia with or without gastritis. It is worth noting that quantitative measurement of symptoms may miss important flare-ups depending on the recall period of the questionnaire used. Prior qualitative work has suggested these flares, although infrequent, can be disruptive for patients, difficult to manage and impact significantly on HRQoL.13
Generic HRQoL measures (SF-36), in this study, suggest BO patients have significantly lower (worse) physical component scores, in particular bodily pain when compared with an age and sex matched UK population norm. These findings are consistent with Lippmann and colleagues45 who examined HRQoL in BO and GORD patients in a single tertiary centre in the USA. Considering BO reflux symptom control is generally good, this finding is unlikely to be solely related to BO and may reflect comorbid disease. Otherwise, using this metric alone (SF-36), BO patients could be considered to have a HRQoL close to that of the general population. This study also highlights the importance of controlling for potential confounding factors when measuring HRQoL, especially when making comparisons between disease groups. Without adjusting for these, data can easily be misinterpreted.
This study highlights key areas of disease impact on BO patients. These findings are important to consider when implementing BO care pathways. Considering historical BO care has been reported as inconsistent, inadequate or non-existent4 13 46 there needs to be a greater focus on counselling patients regarding cancer risk with perhaps an emphasis on using words rather than numerical values in explanations. Previous research has shown that patients’ perception of risk, rather than knowledge of numerical risk, is what drives health behaviour and influences HRQoL.47 48 Although the majority of patients with non-dysplastic BO in this study, and prior research,49 perceive their cancer risk as low there is still a significant minority who overestimate it. Lowering perceived cancer risk in these patients may in turn reduce cancer specific worry, anxiety and depression. This appears key to non-dysplastic BO participants who appear more likely to overestimate their cancer risk (34% overestimate numerical risk and 42% overestimate perceived risk) compared with treated dysplastic/OAC patients (8% overestimate numerical risk and 7% overestimate perceived risk). A prior US cohort study of non-dysplastic BO patients, conducted by Shaheen and colleagues, found even higher rates (68%) of numerical risk overestimation.50 Discussions concerning cancer risk are also important when not pursuing surveillance, for example newly diagnosed patients who do not meet current surveillance criteria. Reassurance for BO patients may also be provided by a negative surveillance endoscopy. DBO treated patients remain under greater endoscopic scrutiny, which may be one explanation as to why they have a perceived cancer risk similar to that of non-dysplastic levels. The reassuring findings of endoscopy should be communicated by the endoscopist immediately and effectively to all, including GORD and colonic polyp patients undergoing endoscopy who typically do not receive further clinical follow-up. This interaction between endoscopist and patient must not be underestimated. Cooper and colleagues found lower (worse) trust in physician scores were associated with greater levels of anxiety and depression.42 Similarly physician-patient communication surrounding surveillance endoscopies has been shown to be vitally important to patients in prior qualitative work.13 51 Surveillance intervals for some patients can be long (3 to 5 years) and the reassurance of a negative endoscopy will naturally dwindle over time. It may therefore be appropriate to provide BO patients with a direct access to secondary care services in-between their endoscopies.
Limitations
This study is not without limitations. First, the response rate is relatively low. This may lead to significant differences between responder and non-responder characteristics introducing bias, which may reduce reliability and generalisability of the results. To provide some insight into this, responder and non-responder non-dysplastic BO characteristics have been provided (see online supplementary table 2.1-1). Second, the demographics of each cohort are not perfectly matched. However, this has been accounted for within the analysis through propensity score matching which included age, sex and comorbidities. Finally, socioeconomic status was not recorded which is another potential confounding factor in HRQoL research. Despite these limitations the data captured are of good quality, multicentre and consider a range of potential disease impacts.
Conclusions
To our knowledge this study provides the largest and most comprehensive quantitative HRQoL measurement of BO patients within the UK’s NHS. Based on these findings, patients require greater reassurance and communication concerning oesophageal cancer risk. Current and future care pathways must be more patient focussed with greater attention given to assessing and addressing misconceptions of cancer risk, oesophageal cancer related worry and GORD symptom control.
References
Footnotes
Contributors All authors significantly contributed to this work. The concept and design of this study was instigated by YA, JM and SH. This study forms part of a larger research project including preliminary qualitative work in collaboration with MH. JB, YA and RW were responsible for driving recruitment. Data analysis was conducted by JB, PT and GM. JB drafted the initial manuscript. All authors then had a role in revision of the manuscript prior to submission.
Funding This study forms part of a larger research project which has received unrestricted external funding support from Covidien (Medtronic). Covidien have not influenced the design of this study, writing of the manuscript or decision to submit for publication. (Medtronic, Grant/Award Number: ISR-2016-10773)
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Prior ethical approval for this study was obtained from the Health Research Authority Yorkshire and Humber ethics committee (REC reference number 16/YH/0035).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.