Article Text

Abstract
Introduction In 2013, peptic ulcer disease (PUD) caused over 300 000 deaths globally. Low-income and middle-income countries are disproportionately affected. However, there is limited information regarding risk factors of perioperative mortality rates in these countries.
Objective To assess perioperative mortality rates from complicated PUD in Africa and associated risk factors.
Design We performed a systematic review and a random-effect meta-analysis of literature describing surgical management of complicated PUD in Africa. We used subgroup analysis and meta-regression analyses to investigate sources of variations in the mortality rates and to assess the risk factors contributing to mortality.
Results From 95 published reports, 10 037 patients underwent surgery for complicated PUD. The majority of the ulcers (78%) were duodenal, followed by gastric (14%). Forty-one per cent of operations were for perforation, 22% for obstruction and 9% for bleeding. The operations consisted of vagotomy (38%), primary repair (34%), resection and reconstruction (12%), and drainage procedures (6%). The overall PUD mortality rate was 6.6% (95% CI 5.4% to 8.1%). It increased to 9.7% (95% CI 7.1 to 13.0) when we limited the analysis to studies published after the year 2000. The correlation was higher between perforated PUD and mortality rates (r=0.41, p<0.0001) than for bleeding PUD and mortality rates (r=0.32, p=0.001). Non-significant differences in mortality rates existed between sub-Saharan Africa (SSA) and North Africa and within SSA.
Conclusion Perioperative mortality rates from complicated PUD in Africa are substantially high and could be increasing over time, and there are possible regional differences.
- peptic ulcer disease
- perforation
- bleeding
- obstruction
- Africa
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of the study
What is known about this subject?
No meta-analysis assessing the perioperative mortality rates of complicated peptic ulcer disease (PUD) has been conducted representative of the entire African continent.
Prior meta-analysis focused only on sub-Saharan Africa (SSA).
We assessed the incidence of perioperative mortality rates in Africa and the associated risk factors.
What are the new findings?
Perioperative mortality rates from complicated PUD display regional and sub-regional variations, higher in SSA than in North Africa.
Within SSA, the mortality rate is greatest in southern Africa.
Mortality rates were moderately correlated for perforated ulcers but had a weak correlation with bleeding PUD.
Meta-regression demonstrated that increasing age was a major risk factor for perioperative mortality.
How might it impact on clinical practice in the foreseeable future?
Perioperative mortality rates from complicated PUD in Africa are high and could be increasing. Region-specific preventative strategies are urgently needed to improve survival.
Introduction
Peptic ulcer disease (PUD) is a common affliction across the globe. According to the Global Burden of Disease estimates, PUD was responsible for over 300 000 deaths in 2013 globally.1 Its sequelae are variable but can be deadly when PUD is complicated by bleeding, obstruction or perforation.2 Until recently, surgery was the dominant method of treatment. Currently, medical therapies provide effective treatment, thereby decreasing complications and the need for surgery.2 3
Overall, the success of medical therapy has led to a decreased incidence of complicated PUD. This evolution has occurred over the past century by three likely mechanisms: the improved socioeconomic conditions of patients, recognition and subsequent treatment of the pathogen Helicobacter pylori, and the advent of proton-pump inhibitors.2 Additionally, diagnostic and therapeutic endoscopy has become a prominent component of PUD management. The benefits of these advances can be substantial, though they are not universally available.4
Despite these advances, the burden of this disease persists in low-income to middle-income countries (LMICs). Previous studies have found that countries with fewer resources exhibit higher rates of death from PUD.2 In fact, PUD has been identified as the leading cause of death among emergent surgical conditions with a rate of 3.5 per 100 000 deaths, 85% of which occur in LMICs.3
A previous review has examined perforated PUD focusing on sub-Saharan Africa (SSA).5 However, no systematic review has investigated perioperative mortality rates following PUD surgery in all of Africa. Africa is a heterogeneous continent where countries have different political, social and economic structures. Diseases and health outcomes tend to be heterogeneous, and therefore, providing a one-size-fits all health message becomes ineffective if not tailored to the regional or country level. We, therefore, sought to add North Africa to our study with the aim of exploring possible regional differences in the perioperative mortality rates that could exist between North Africa and SSA. Factors responsible for the variations in mortality rates have not been explored. To fill in the gap in knowledge, we aimed to systematically describe the literature on the profile of PUD requiring surgical intervention and the associated mortality in Africa and to explore sources of variations.
Methods
Literature search strategy
We developed a study protocol (see online supplementary text 1) based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (see online supplementary table 1). We searched three databases (MEDLINE, Embase and Cochrane Library) to identify all studies which reported on mortality rates following surgical management of complicated PUD. The last search date was 8 February 2019. Keyword and Medical Subject Headings were done with various combinations of search terms “peptic ulcer disease”, OR “gastric ulcer”, OR “duodenal ulcer”, AND (“mortality” OR “Death” OR “Hospital Mortality” OR “Perioperative Period”, AND “Africa”). The full list of search terms is given in online supplementary table 2. No restrictions were imposed on the year of publication, patient characteristics such as gender, ethnicity and age at diagnosis, or on the language of the publication in order to maximise catchment of relevant studies and to allow for a more thorough analysis.
Supplemental material
Inclusion criteria, study population and case ascertainment
Studies were included in the analysis if they met the following inclusion criteria: the study examined the incidence of mortality among patients who underwent surgery for complicated PUD (the proportion of patients with PUD who died perioperatively and postoperatively). The definition of complicated PUD in our study was an ulcer with bleeding, perforation, obstruction or refractory to conservative management. We defined the perioperative mortality rate as in-hospital death during or after the operation.
Study selection
Two of the authors (SP and MP) independently reviewed titles and abstracts to identify records that were deemed potentially eligible for inclusion. Two authors (SP and MP) independently confirmed the eligibility of retrieved articles. Data were extracted from eligible articles. We excluded publications that were duplicates, and studied only non-complicated PUD, case reports and case series.
Data extraction and quality assessment
Data were extracted from studies independently by two authors (SP and MP) using an adapted version of a standard data entry electronic form (see online supplementary table 3). Disagreements between extractors were discussed with other coauthors (PS and LK) until a consensus was reached. The overall mortality rate of the study population was extracted from each eligible paper. Data on country and region in which the study was conducted, year of publication, study design, sample size, mean age at the time of presentation for surgery, gender, history of PUD and duration of chronic symptoms, risk factors (non-steroidal anti-inflammatory drugs (NSAIDs), smoking, alcohol, H. pylori), ASA status, presence of shock on admission, duration of acute symptoms, presence of free air on X-ray, ulcer location, type of PUD complication (bleeding, perforation, obstruction or other) and type of surgical procedure. Two authors (SP and MP) independently assessed the quality of the papers included in the review using the Oxford Centre for Evidence-Based Medicine’s Levels of Evidence Guidelines (March 2009).6
Data analysis
The primary outcome was the estimation of the overall perioperative mortality rate in patients with complicated PUD. The metaprop function from R package meta was used to calculate the pooled effect estimates of mortality rates in patients with PUD.7 There was significant between-study heterogeneity (I2=80%, p<0.01). Therefore, a random-effect model was employed for the analysis. The random-effect models are more conservative than fixed-effect models and generate a wide CI. We used the byvar option to conduct subgroup analysis by region (SSA vs North Africa), sub-region (West, East, Central, South and North Africa) and country. The proportions (mortality/sample size) were transformed using the logit transformation to stabilise the variance. We chose the logit function because it does not have problems with back-transformation observed when Freeman-Tukey double arcsine is used.8 We used the DerSimonian-Laird estimator method to estimate the pooled between-study variance.9 Results were graphically displayed in forest plots.
A random-effect meta-analysis model assumes that the observed mortality rates among patients with PUD can vary across studies because of real differences in the PUD mortality rates in each study, as well as sampling variability (chance). Such heterogeneity is caused by differences in study populations (such as the age of patients), type of PUD complication and other risk factors. Between-population heterogeneity was assessed using I2 statistics, expressed as % (low (25%), moderate (50%) and high (75%) and Cochrane’s Q statistic (significance level of <0.05).10 To investigate potential sources of heterogeneity, we conducted meta-regression analyses.11 We examined independent correlates of mortality rates using mean age, sub-region and year of publication as predictors. Study-level determinants of mortality rates were expressed as absolute differences in the percentage of perioperative mortality. Potential ascertainment bias (as might be caused by publication bias) was assessed with funnel plots, by plotting the study effect size against SEs of the effect size, and Egger’s test.12
Results
Clinical and surgical attributes
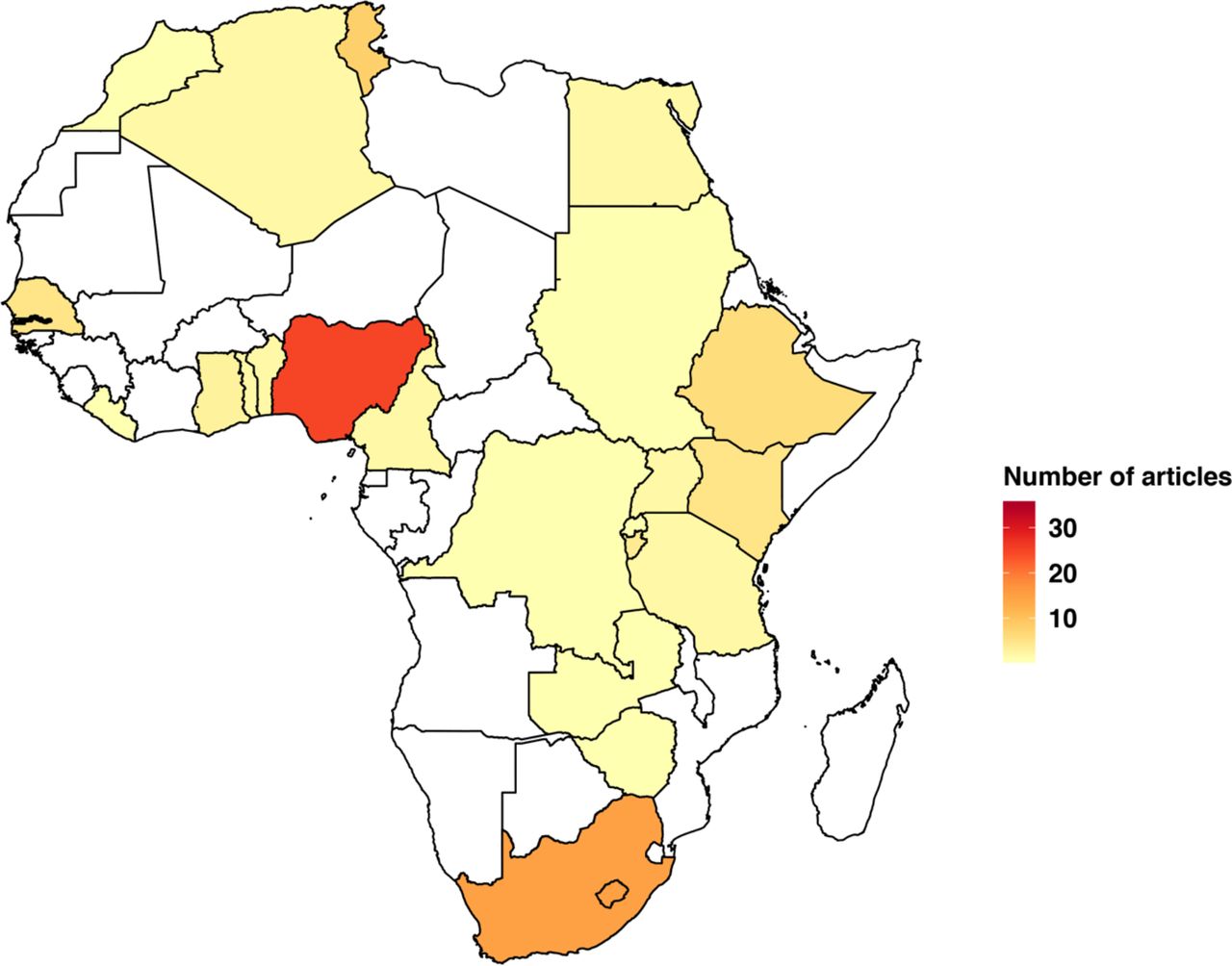
Our search retrieved 1196 articles, of which 122 were carefully reviewed (figure 1). We retrieved the full text for all of these articles and carefully reviewed each one. The full-text review identified 95 eligible papers from 24 countries in Africa. These studies yielded a total of 10 037 patients with complicated PUD. The vast majority (85%) of the studies were from the sub-Saharan region. Nigeria contributed the most studies (25) followed by South Africa (15) (figure 2). The year of publication ranged from 1955 to 2018. Figure 3 shows the map of Africa displaying the mortality rates. The clinical and surgical attributes of the patients included are summarised in table 1. Men constituted 79% of the patients, and the median age for the entire study sample was 39 years (SD 8.6 years). The proportions of patients with a history of smoking, alcohol intake and NSAID use were 57%, 45% and 35%, respectively, and 64% had a history of peptic ulcers. The anatomical location of the ulcers was predominantly duodenal (78%) followed by gastric (14%). Regarding complications indicated for surgery, the vast majority of the PUDs were perforated (41%). Obstruction and bleeding were the indication for surgery in 22% and 9% of the patients, respectively. Surgical procedural types were vagotomy and drainage in 38% and primary repair in 34% of the patients, although resection and reconstruction and drainage and were also slightly too moderately represented (12% and 6%, respectively). Study-specific details and references are in table 2. All of the articles were scored as level 2 B evidence (see online supplementary table 3).

PreferredReporting Items for Systematic Reviews and Meta-Analyses flowchart of a systematic review of peptic ulcer disease mortality in Africa.

Distribution of the number of articles analysed.

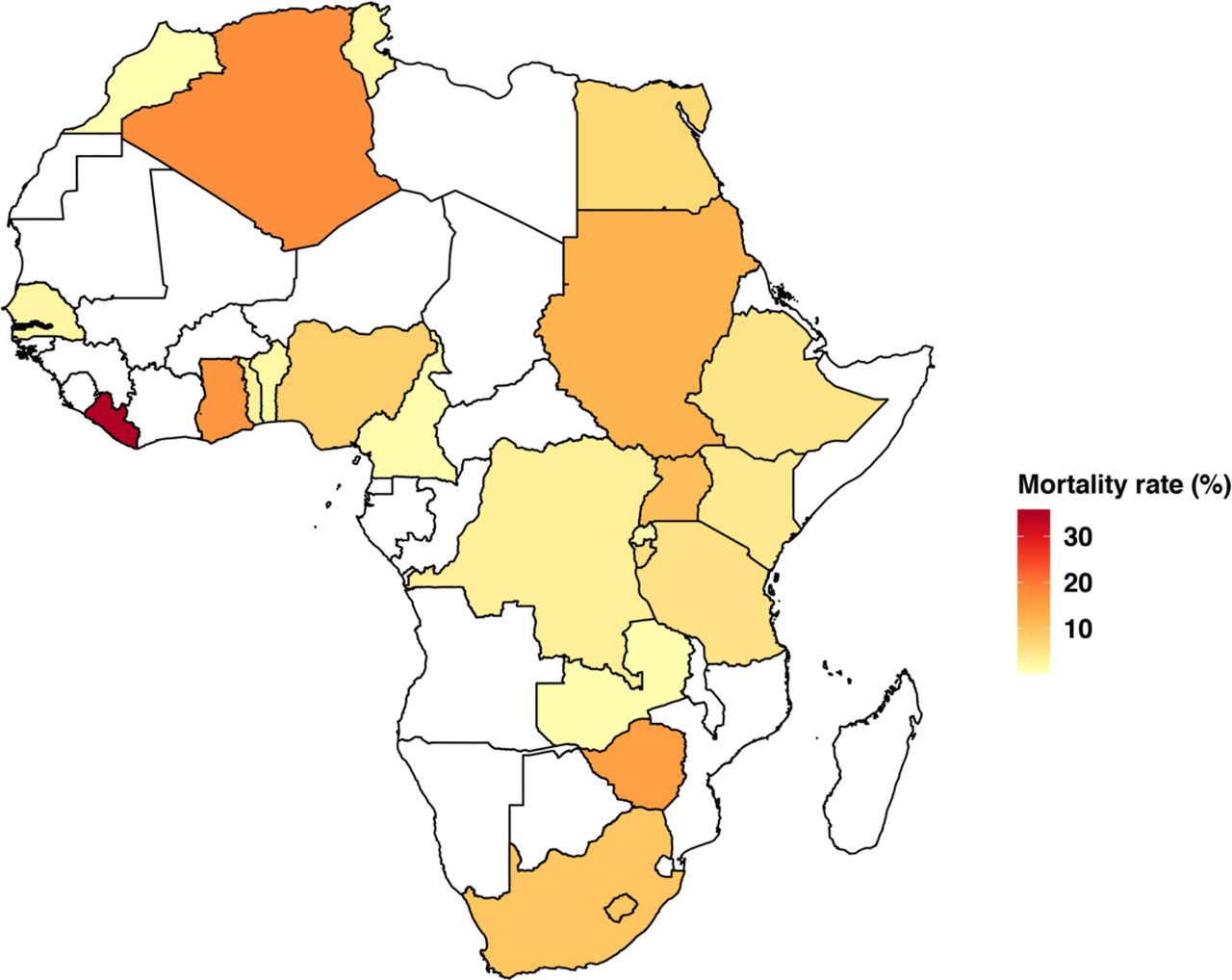
Distribution of the perioperative peptic ulcer disease mortality rates in Africa.
Clinical and surgical attributes of patients with peptic ulcer disease included in the meta-analysis
Subgroup analysis and meta-regression for the perioperative mortality rates from complicated peptic ulcer disease in Africa
Meta-analysis
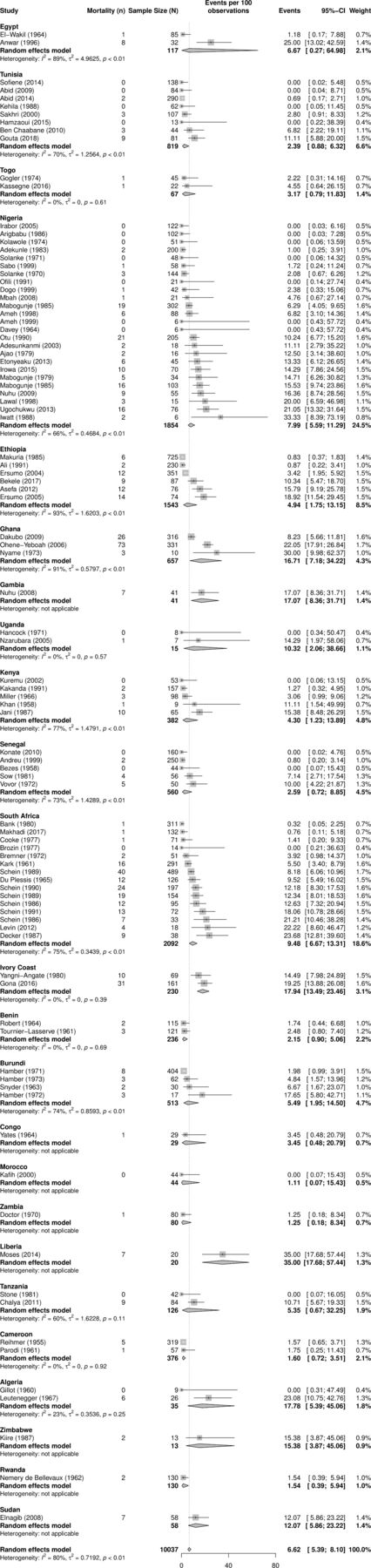
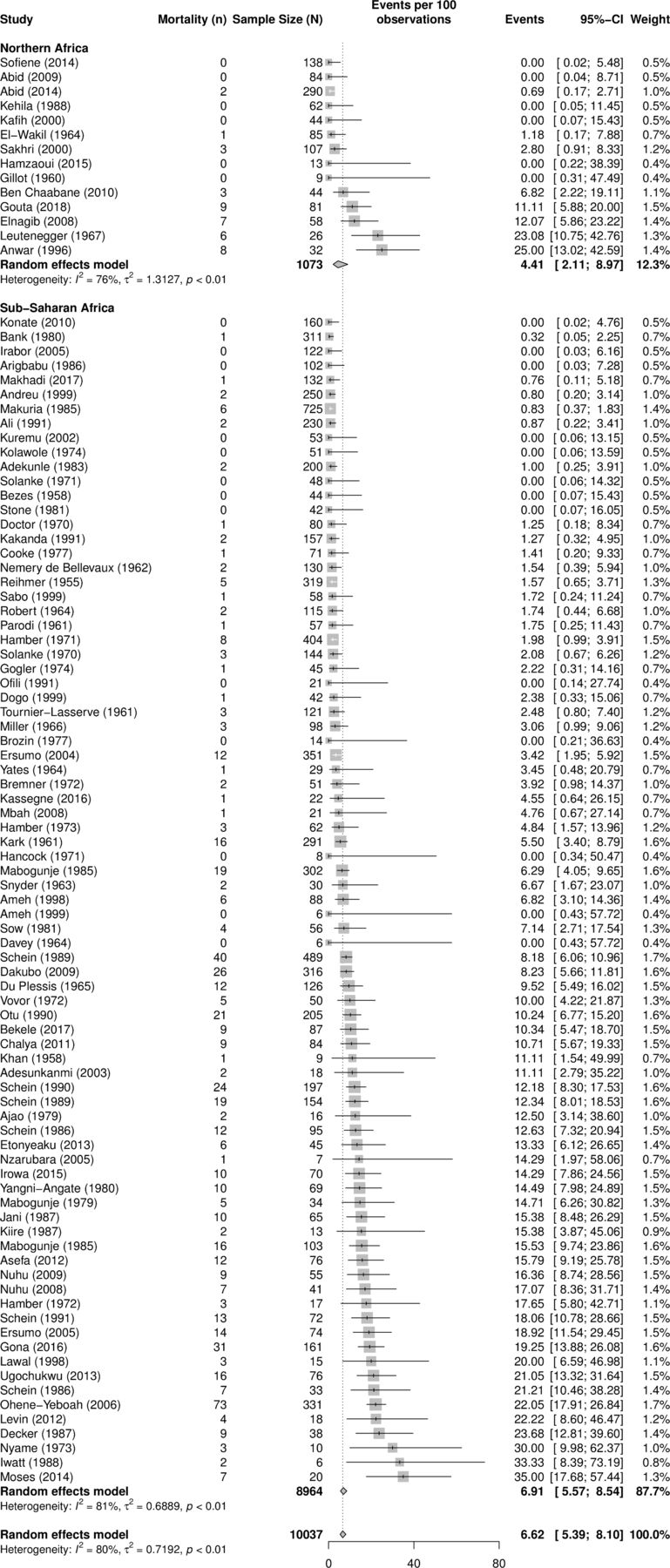
The overall perioperative mortality among patients with PUDs was 6.6% (95% CI 5.4% to 8.1%). (figure 4). It increased to 9.7% (95% CI 7.1% to 13.0%) when we limited the analysis to studies published after year 2000 (figure 5), suggesting that the overall effect is not driven by older studies, which are more likely to have a small sample and report retroactive data. Displayed in figure 6 are the country-specific mortality rates. The mortality rates varied widely between countries, with the lowest in Morocco, 1.11% (95% CI 0.07% to 15.43%) and the highest in Liberia, 35.00% (95% CI 17.68% to 57.44%). Between-study heterogeneity for the overall mortality rate was very high (I2=80%, p=0.01). On a sub-regional basis (figure 7), South Africa displayed the highest mortality at 9.14% (95% CI 6.46% to 12.78%), a rate which was higher than that of Central Africa, 1.78% (95% CI 0.85% to 3.69%), but not different from the mortality rates of East, West or North Africa. Regional disparities were also evident. Mortality rates were higher in SSA, 6.9% (95% CI 5.39% to 8.10%), compared with North Africa, 4.41% (95% CI 2.11% to 8.97%), even though the difference was not statistically significant (figure 8).
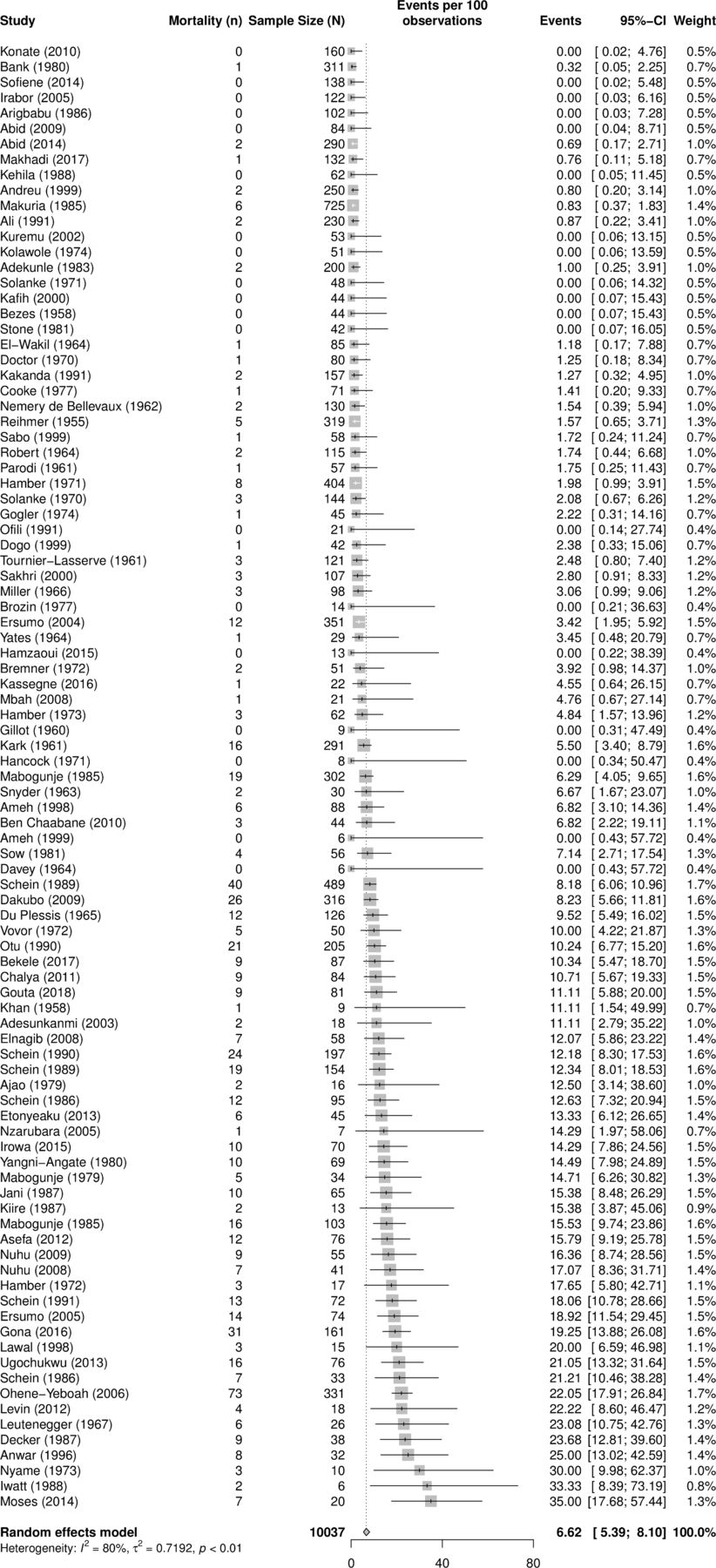
Overall pooled peptic ulcer disease mortality rates (%) in Africa.

Pooled peptic ulcer disease mortality rates (%) in Africa stratified by publication year.

Country-specific peptic ulcer disease mortality rates (%) in Africa.
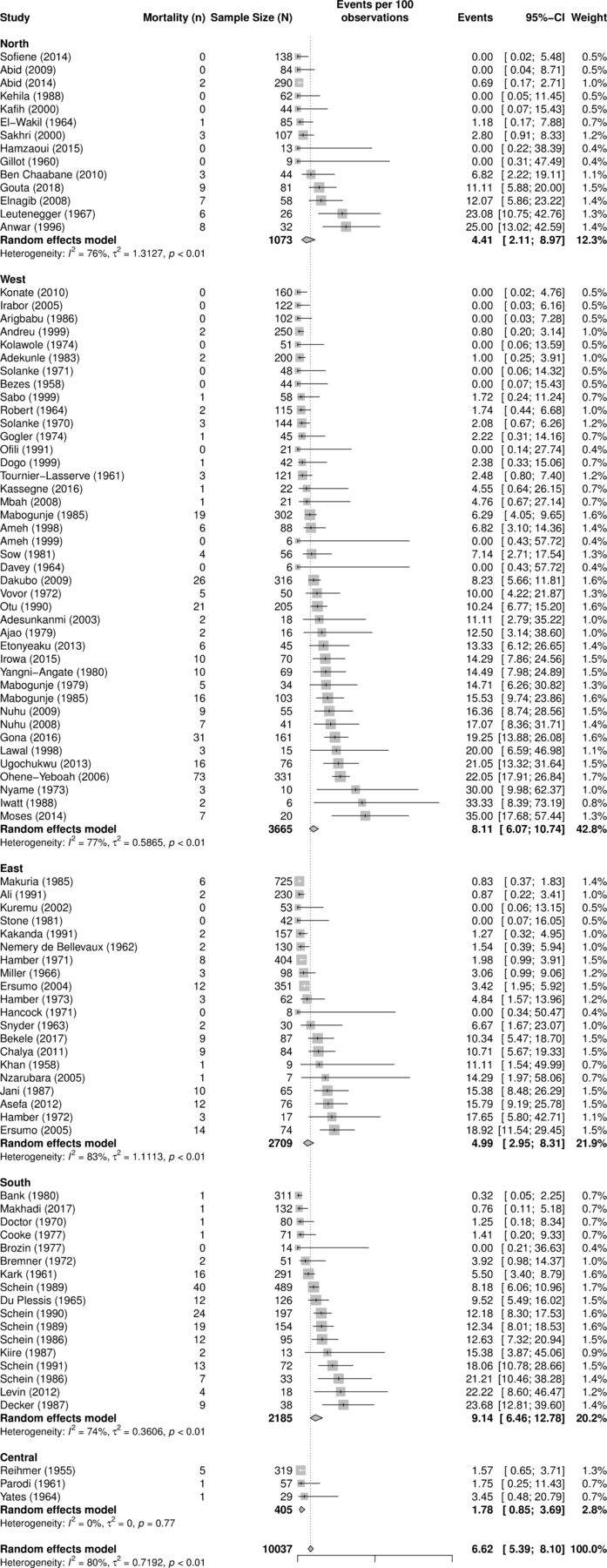
Subregion-specific peptic ulcer disease mortality rates (%) in Africa.

Region-specific peptic ulcer disease mortality rates (%) in Africa.
The main results in the preceding paragraph should be understood in light of possible publication bias. In fact, Egger’s test for publication bias was significant (p<0.0001), and the funnel plots—which showed the relationship between effect size against the SEs— displayed asymmetry (see online supplementary figure 1).
PUD mortality risk factor analysis: correlation
The scatterplots in figure 9 display the correlation between mortality rates and the selected covariates. As shown in figure 9A, duodenal ulcers were negatively associated with mortality rates (r=−0.19, p=0.07); however, gastric ulcers were positively associated with mortality (r=0.23, p=0.036; figure 9B). Although both bleeding and perforated ulcers were both positively associated with mortality (figure 9C,D), the latter had a stronger association (r=0.41, p<0.0001). To test the hypothesis that survival rates are increasing in recent years, we investigated the correlation between publication year and mortality. There was a positive association between publication year and perioperative death rates (r=0.22, p=0.032; figure 9E). Likewise, as shown in figure 9F, mortality rate increased with increasing age at surgery (r=0.23, p=0.036).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation of peptic ulcer disease mortality rates and risk factors/covariates. (A) Duodenal ulcers. (B) Gastric ulcers. (C) Bleeding ulcers. (D) Perforated ulcers. (E) Publication year. (F) Age at surgery.
PUD mortality risk factor analysis: meta-regression
To further investigate the sources of heterogeneity, we applied meta-regression analysis using the following covariates: study-level mean or median age at surgery, year of publication, sub-region and study quality score. Substantial heterogeneity of effect estimates on perioperative mortality rate was evident (p value for heterogeneity of <0.0001). Multivariable meta-regression model including the above-mentioned covariates indicated that per every 10-year increase in publication year, the mortality rates increased by 1% (table 2). Regions and sub-regions were not significantly associated with mortality rates. However, the association between age and mortality risk was marginally significant. With every 10-year increase in age, the mortality rate increased by 2% (p=0.07).
Discussion
The results of this meta-analysis show that the mortality rate due to surgical PUD in Africa is approximately 6.6%, which is comparative to previous reviews limited to SSA that found a mortality rate of 5.7%.5 There is considerable heterogeneity across the continent, both between countries and between geographical sub-regions. The disease characteristics, including the mortality rate, are not consistent with what is observed in high-income countries (HICs).3 The majority of patients in the population studied were young, adult men. Most ulcers were located in the duodenum rather than the stomach. In HICs, this was historically the predominant profile of patients with PUD; however, this has changed considerably over the last 50 years such that the male to female ratio is nearly equivalent; patients are older; and gastric ulcers predominate.3 These changes, attributed to economic development, have not yet been observed in much of low-income countries, as seen in this review. The prevalence and the severity of ulcer complications in HICs have decreased over time as a consequence of eradication of H. pylori, avoidance of NSAIDs and use of acid suppression medications, especially proton-pump inhibitors.3 13 14 The opposite is true in LMICs, such as those in Africa. Here, the mortality rates from complicated PUD increased from approximately 4.8% in 1950 to 10% in 2010, but PUD mortality rate still diverges from secular decrease in overall mortality in the region. There could be several factors explaining the observed secular trend of increased mortality. First, earlier studies included operations predominantly for chronic ulcers, whereas recent papers were predominantly perforations (see online supplementary table 3), which have a worse prognosis. Therefore, the observed trend could be a data-driven effect from selection bias as the focus of the surgical PUD literature shifted from uncomplicated PUD to complicated PUD over time. Second, earlier papers could have had poor quality compared with the recent paper. However, the quality assessment showed that the majority of the included published papers had a similar score of 2B.
The surgical care for complicated PUD has mirrored changes in presentation. Globally, definitive ulcer operations have become all but obsolete15 as medical care for PUD evolved. This pattern is also depicted in this analysis wherein primary repairs now predominate. Over the time period studied, the number of operations performed for perforation increased, along with associated mortality and primary repairs. The observed overall increase in mortality may reflect the emergent nature of these complications. When once, patients underwent elective surgery for chronic PUD and may not have had access to emergent surgical care, now, patients may have access to emergent surgery. Alternatively, it may be a data-driven artefact from selection bias as the focus of the surgical PUD literature shifted from uncomplicated PUD to complicated PUD over time.
In a recent first national study in the UK of complicated PUD requiring emergency surgery found in-hospital 60-day mortality to be higher in patients with bleeding (17.8%) than in patients with perforated PUD (11.7%),16 and yet the vast majority of complicated PUD was perforation (86%). However, a recent European study reported 90-day mortality rates to be higher for perforated PUD at 29.8% than in bleeding PUD at 5.3%.17 In our analysis, the correlation was stronger between perforated PUD and mortality (r=0.41) than bleeding PUD and mortality (r=0.32). It is important to note that this review includes only patients who underwent surgical therapy and therefore does not aim to characterise the overall prevalence of the different complications of PUD.
Furthermore, endoscopic therapies may decrease mortality rates where available, and a lack of access to these may contribute to the mortality rates seen in LMICs. Additionally, older patients are more likely to die from complications of PUD. With increasing life expectancies that accompany economic development and improved healthcare, mortality due to PUD may be a rising problem in ageing populations.18–20
This review demonstrated substantial heterogeneity in mortality from PUD across continental Africa. This heterogeneity could be due to several factors. For example, cultural and socioeconomic factors vary across the continent, and these contribute to the transmission of H. pylori.21 Additionally, access to healthcare varies and may influence the likelihood of treatment for PUD before and after a complication has occurred. As has been recently described by the Lancet Commission, five billion people lack access to safe surgical care.22 Surgical capacity is also a likely factor behind the heterogeneity we observed. According to the Global Burden of Disease Study (GBDS), PUD is the most significant contributor to death and disability among emergent surgical conditions.4 GBDS data also show that the countries in the lowest quintile of the Human Development Index have the highest rates of death and disability attributed to perforated PUD.2
The mortality rates varied significantly for different countries across Africa. Broader analysis between sub-regions and regions revealed fewer differences. When considering the factors mentioned earlier contributing to health outcomes and access to care, we may have expected to see consistently worse mortality in LMICs. Surprisingly, Central Africa had the lowest mortality rate despite its comparatively lower socioeconomic status and political instability. Very few of the studies in our sample were conducted in this region, and they may not be representative. In these conditions, patients may die due to a lack of access to healthcare, making it difficult for researchers to collect accurate information on prevalence. Additionally, in limited-resource areas, infrastructure may not support data collection and reporting. Capacity building and research support are critical in these areas.
Due to the multifactorial nature of complicated PUD, future work to decrease the associated morbidity and mortality must address multiple issues. One, as noted earlier, is healthcare infrastructure. Time to treatment in the setting of peritonitis and sepsis impacts survival. Surgical capacity building is needed to provide safe and timely access to emergent surgical care. Primary prevention of PUD inclusive of interventions to decrease NSAID use and smoking could also be effective.23 Finally, preventing infection by H. pylori, the most critical risk factor for PUD, would be a powerful influence. Currently, there are no vaccines; however, decreasing infection through improved sanitation represents an opportunity to prevent long-term consequences.
H. pylori is highly prevalent in many parts of Africa. Random screening for H. pylori revealed a rate of infection of 85%.24 Given the extent of disease and potential for complications (including gastric carcinoma not specifically discussed here), H. pylori infection poses a significant threat. Test-and-treat strategies have been proposed, and in areas of high prevalence, initial treatment with triple therapy (two antibiotics and a proton-pump inhibitor) is recommended.21 Ideally, a mass eradication programme should be considered. In fact, there is some evidence that such programme can be effective. For example, a randomised controlled trial in Taiwan administered clarithromycin-based triple therapy to participants positive from urea breath test.25 The intervention yielded a 78% reduction in H. pylori in treated patients. Such a programme could decrease the rates of complicated PUD and its associated morbidity and mortality.
Strength and weakness of the study
A key strength of our study is that it is the first systematic review with meta-analysis to describe the mortality rates of complicated PUD as well as associated risk factors in the entire continent of Africa. We use data from over 50% of the countries in Africa, spanning 60 years. As such, our findings are less vulnerable to generalisability concerns than the single-setting studies available so far.
Our study also had limitations. First, some regions, particularly west and south Africa, were poorly represented in terms of the number of publications available and the quality of the data. The implication is that our sample of patients may not be fully representative of the population in Africa. Given that the under-represented regions are also the regions with relatively poor infrastructure, access and socioeconomic status, where mortality from PUD might be higher, our current estimates are likely downward biased.
Second, medical history, including H. pylori infection and treatment, and use of prescription drugs such as NSAIDS or proton-pump inhibitors were not reported in several studies. As a result, we could not ascertain if these factors contributed significantly to the overall patterns of PUD-related postoperative mortality.
Third, while including publications from 60 years ago allows for analysis of temporal trends in mortality rates, it is nearly impossible to account for the improvements in research methodology and resultant improvements in research quality that have occurred over the past decades. Therefore, the observed increase in postoperative mortality among patients with complicated PUD might be a result of improved data collection methods rather than a real effect.
Conclusion
PUD has a high mortality rate in Africa, particularly in the sub-Saharan region and South Africa. The drivers of PUD in SSA are multifactorial and are poorly understood. Future studies need to address these gaps. This will assist in identifying entry points for effective interventions to reduce mortality from PUD.
References
Footnotes
SP and MP contributed equally.
Contributors PS, LK and JSO conceived the initial study idea. PS carried out the statistical analyses and drafted the manuscript. SP, MP, EGK and RO-O prepared the data and participated in the statistical analyses and critical revision of the manuscript. VMC and YA contributed to the statistical analyses, drafting and critical revision of the manuscript. JSO, LK and DIS contributed to the critical revision of the manuscript. All authors approved the final manuscript version to be published and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.