Article Text

Abstract
Introduction Axial hiatal hernias are a common incidental finding in endoscopical examinations, but reflux symptoms do not necessarily correspond to the presence of hiatal hernias. Diagnosing a reflux disease is difficult due to a leak of existing distinct criteria, especially in order to evaluate a surgical indication. Also a preoperative measurement of the hernia is necessary to choose between surgical options.
Methods and analysis We planned a semiblinded trial including a questionnaire and an oesophagogastroduodenoscopy afterwards. While the endoscopy is done, the hiatus oesophagi should be measured in inversion technique under maximum insufflation including length, width and herniated volume. A sample of 210 participants until December 2020 is determined to evaluate the primary endpoint: we look forward to evaluate the anatomical parameters of reflux and non-reflux participants.
Ethics and Dissemination The study has been approved by the local ethics committee on 12th February 2019, the data will bei published after closure of inclusion.
Trial registration number German Clinical Trials Register (DRKS00016863).
- reflux
- gastroscopy
- hiatal hernia
- endoscopical technique
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The incidence of axial hiatal hernia is much higher in those with reflux symptoms than in those without.1 To evaluate the causality of reflux symptoms pH-metry and oesophageal manometry are common examination techniques,1 2 otherwise some authors refuse these methods in case of documented reflux symptoms and hiatal herniation.3 Our aim is to evaluate the morphology of hiatal hernia and to correspond diameter and volume to several symptoms. Manometry and pH-metry are, according to German guidelines, optional to define reflux symptoms caused by hiatal hernia.4 For example, manometry is used to define the exact axial length of the hernia and to evaluate the sphincter motility,5 yet the clinical purpose of motility disorders is not fully understood.6 At the moment we do not see a technical option to measure the width of the hernia in maximum insufflation using manometry in order to compare the findings of this method to visual endoscopy. On behalf of pH-metry we would like to argue similarly: on the one hand, Quality of Life Questionnaires do not necessarily correspond to the findings of DeMeester scorings,7 on the other hand, we assumed that it would be difficult and dangerous for the participants to take part in 24-hour pH-metry under maximum insufflation due to the risk of aspiration.
We strongly recommend the idea to verify the influence of axial hernias by corresponding methods, that is why we are looking forward to use manometry and pH-metry in normal insufflation and laparoscopic measurements as next step in following studies.
Often classifications of hernias are based on the axial length, but the differences between symptomatic and non-symptomatic patients are small and investigator dependent.8 9 As a scale to measure the width of the hernia, the diameter of the endoscope is used, but the results vary on a wide range.9
One reason for poor interobserver agreement could be different techniques and standards in measuring the hiatal hernia, for example, measuring the hiatal flap, the diameter or axial length.8 10 Therefore, we try to standardise the endoscopical evaluation to determine the length, diameter and volume of the hernia. The clinical relevance of axial length remains unclear,11 that is why we hope to improve the reliability by measuring the herniated volume. Also it is the width that determines the choice of operation method.12 Although evaluating the hiatal hernia in retroversion/inversion is not a new technique,10 to our knowledge it is the first time to collect the data in order to calculate the volume. As you may see in figures 1 and 2, the hiatal hernia under maximised insufflation appears to be much wider (figure 2) than under ‘ordinary’ conditions (figure 1), yet there is no proof of clinical relevance of this observation.

Endoscopical image of the hiatus oesophagus of a female participant in inversion without maximum insufflation.
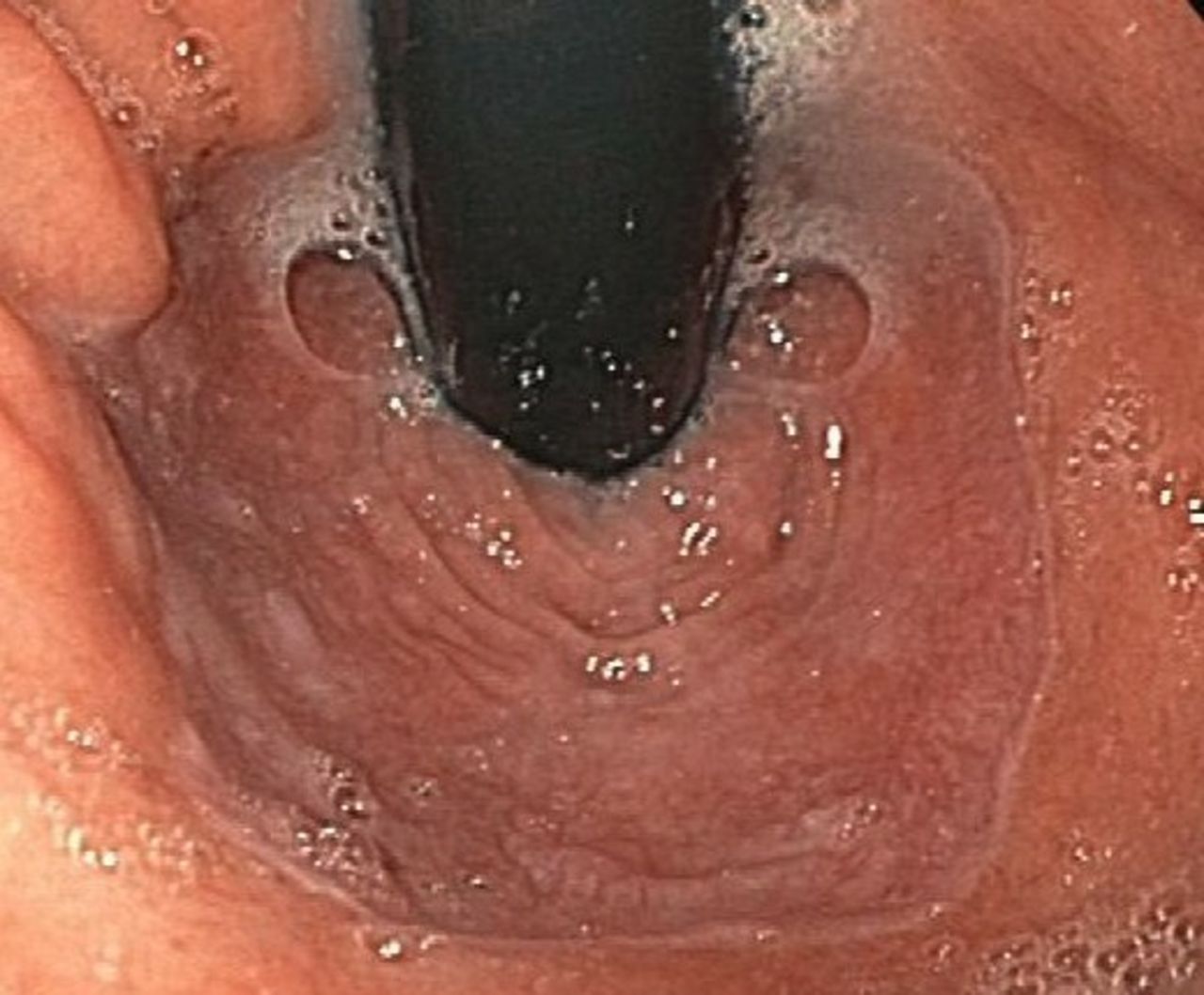
Endoscopical image of the same hiatus in maximised insufflation.
By using a questionnaire to evaluate the symptoms of reflux disease this trial issues to correlate the symptoms with the data measured via endoscopy. Former studies documented little correlation,8 9 so for clinical purpose it seems difficult to indicate an antireflux operation just because of typical symptoms.3 Using additional diagnostics, for example, manometry, pH-metry and pathological mucosa lesions, may help indicate surgical therapy, but it is not a single standing argument.1 2 9
In the long run we aim to define a classification based on clinical purpose and the herniated volume helping to choose between surgical and non-surgical treatment. We therefore hope to extend our procedure to multiple endoscopical centres and to compare the findings of endoluminal measurements with laparoscopic/extraluminal parameters in a second trial.
Methods and analysis
This study is a semiblinded trial comparing different types of categorisations of hiatal hernias, including diameter, axial length and volume of those suffering from reflux symptoms, according to a questionnaire with those who don’t. The endoscopist does not know the questionnaire results. Because of the missing influence of the use of proton pump inhibitor (PPI) to the anatomical parameters of hiatal hernias, we refused to evaluate the PPI response in detail.
During the oesophagogastroduodenoscopy (OGD) the endoscope can be moved to inversion to examine the diameter of hiatus oesophagus after maximising the insufflation of the stomach. Afterwards, the investigator will measure the axial length. The volume could be calculated out of these data.
Hypothesis
The following hypotheses are intended to be tested:
H0: The diameter, axial length and herniated volume of the hiatus oesophagi of those suffering from reflux symptoms (scored via questionnaire) and non-suffering participants are equal.
H1: The hiatal hernia of reflux participants is wider, longer or of increased herniated volume than the ones of non-reflux participants.
Trial design
The so called "HiatoGast 1"-Trial is a monocentric, observatory one consisting of two steps. First, the participants’ reflux symptoms will be evaluated by a special questionnaire. The questionnaire consists of 15 items corresponding to different symptoms (eg, nausea, vomiting, dysphagia, heartburn, regurgitation, use of PPI, and so on) or differential diagnosis of reflux disease (angina pectoris, gastric surgery, chronic obstipation). The intensity and frequency of the symptoms will be documented as a Likert scale.
Afterwards an investigator conducts the OGD. The OGD will be performed as routine intervention in sedation. All three organs will be examined and pathologies will be documented and/or biopsies will be taken. During this examination the endoscope can be moved to inversion to examine the hiatus oesophagus. To do so, the stomach will be bloated to maximum insufflation. Afterwards, the diameter (oesophagogastric junction and hiatal) and shape of the hiatus can be evaluated and documented. The axial length is defined as the difference of endoscope’s length at hiatus and Z-line measured close to teeth row by ruler.
Out of these data we will be capable of calculating the herniated gastric volume using the mathematical model of a blunt cone. Statistically the measurements of reflux and non-reflux participants will be compared: as the answers to the questionnaire will be of nominal status square contingence will be performed. For evaluation of significant differences between hiatal volume, diameter or axial length, Student’s t-test or Mann-Whitney U test will be used based on a p value <0.05. The comparison of different parameters will be evaluated by analysis of variance (p<0.05).
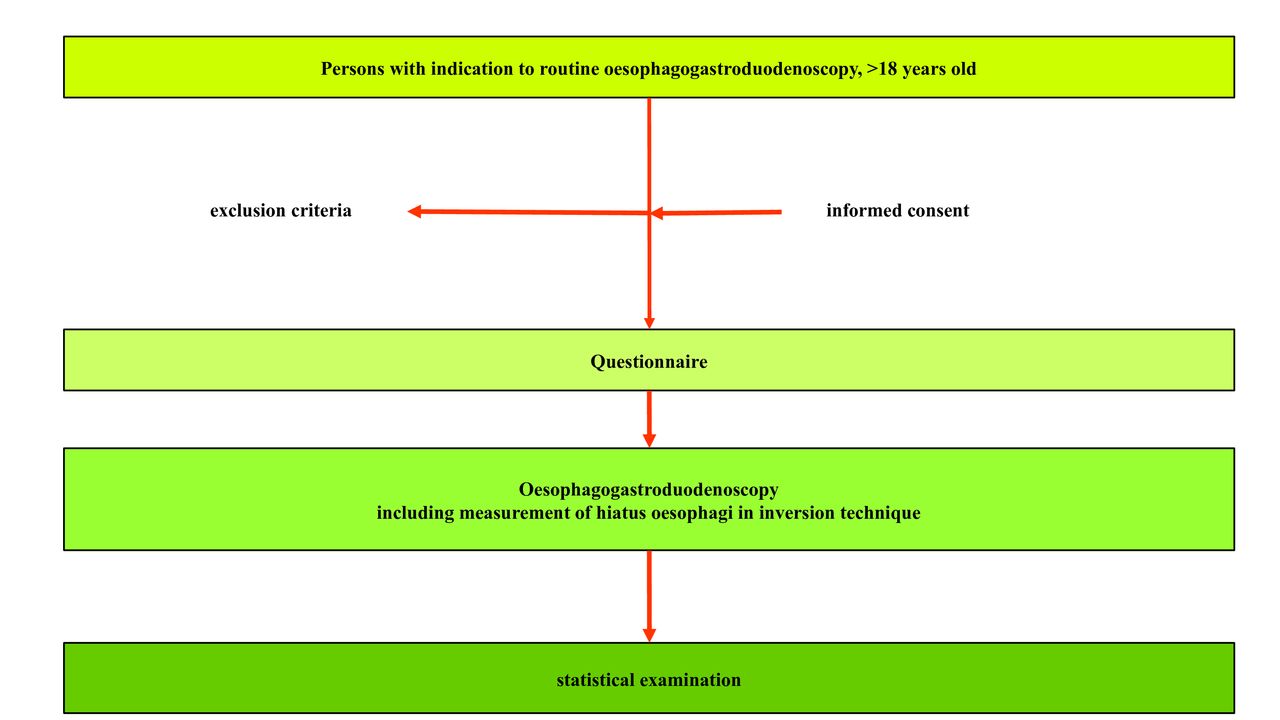
Figure 3 illustrates the design: study population and eligibility criteria.

{kind=link}
{kind=link}
{kind=link}
The trial design.
The study population consists of those over 18 years old who undergo routine OGD because of a medical indication. Persons who are willing to take part after informed consent and who are capable of understanding the risks and tasks of the study will be included. Reflux symptoms are not a criterion a priori. Emergency indications of OGD and participants who underwent surgery of the stomach are excluded, all indications must be medical and independent of our study. There will be no physical screening before inclusion.
Trial location and organisation
"HiatoGast 1"-Trial is located at the university hospital of Friedrich-Alexander University Erlangen-Nuremberg, Germany.
DE is responsible for the study protocol, the reporting of adverse events and the preparation of informed consent forms. The inclusion will be operated by the surgeon or physician explaining the OGD as well. The OGD will be performed by experienced investigators who underwent training in inverse evaluation of the hiatus by ME.
Sample size and trial timeline
The sample size is evaluated based on the primary endpoint. The number of participants is based on calculations done by the software G*Power V.3.1.9.2 by Franz Faul, University of Kiel, Germany, ©1992–2014, as a sample size of 210 participants. The actual power has been calculated to 95%. The trial has started in February 2019.
Randomisation, allocation and blinding
The participants are not randomised, the endoscopist does not know the questionnaire results. We refer to this scenario as semiblinded.
Interventions
There is no planned intervention according to the study protocol. It is possible that participants undergo interventions because of the indication/illness.
Follow-up
The study does not include any follow-up.
Primary and secondary endpoints
Primary endpoints
Our goal is to evaluate the differences in hiatal hernia size between participants with and without reflux symptoms relative to the way of measuring (axial vs diameter vs volume).
Secondary endpoints
It is our goal to establish an endoscopical method evaluating axial hiatal hernias, which would be capable of defining hiatal hernia determined reflux symptoms from other reflux causes.
Ethics and dissemination
The Ethics Committee of the University of Erlangen-Nuremberg, Germany, reviewed the study on 8 January 2019. After several clarifications within the consent forms of data security, participation and general participant information the study was approved during the ethics committee summit on 12 February 2019 (reference number 473_18). We hope to publish the data in an internationally available medical journal.
Data management
As the reason for gastroscopy is a strict medical one, the clinical as well as the study relevant data are collected within the clinic’s documentation system (‘ViewPoint’). The additional photos will be collected there as well, the measurement of Z-line and hiatus in inversion must be documented on a separate form. Prior to gastroscopy the investigator will ask the patient for consent. All data (informed consent form, examination results) will be pseudonymised and stored. The original as well as the pseudonymised data will be stored according to German law.
The participant is free to withdraw his or her consent for using, saving or publishing the personal data at any time before initial publishing. The data will be deleted after written declaration.
Safety and reporting of serious adverse events
The indication for endoscopical examination is always a medical one made by a physician. Therefore, the main risks correspond to those of an ordinary OGD while being under sedation. Presumably, there is a minimally elevated risk of overdosing due to a prolongation of the examination. As the stomach will be fully bloated while measuring the hiatus oesophagi the risk of aspiration could be higher. For performing an examination of the hiatus in inversion it is necessary to invert the endoscope using the stomach wall as a barrier. Therefore, a slight increase in mucosa injuries could be possible.
Serious adverse events (SAE), that is, aspiration, bleeding or perforation, will be reported to the principal investigator within 24 hours and will be documented on a special SAE form. The principal investigator will decide whether the event is unexpected and connected to the study procedure. If so, he will report the case to the local ethics committee within 1 week. An evaluation of SAE is planned after examination of 100 participants and after finishing the study.
Methods for minimising bias
Selection bias is presumably not relevant to this study because of wide inclusion criteria. All endoscopies are done by skilled physicians or surgeons supervised by investigators comfortable with inverse evaluation of the hiatus oesophagi. The trial protocol is published within the ethics committee database (www.ethikkommission.fau.de) with explanation to endpoints, methods and statistical evaluation. The study is funded by the department’s income, so we do not see any inappropriate influence from a third party.
Good clinical practice
All investigators took part in a special course explaining the guidelines on ‘good clinical practice’ by the Declaration of Helsinki.6 All investigators were additionally briefed on data security law and informed consent practice.
Registration
The study has been registered in the German Clinical Trials Register, a primary register of WHO operated by the German Institute for Medical Documentation and Information, on 5 March 2019 and can be reviewed under the registration number DRKS00016863.
Protocol version
This protocol is based on the full study protocol issued on 3 December 2018. Relevant corrections or substantial changes within the protocol need to be reported to every investigator, participant, the ethics committee, the trial registry and the journal.
Footnotes
Contributors DE, MAE and ME invented the study design. DE wrote the manuscript and calculated the sample size. HG, CK and RG reviewed and corrected the manuscript, the informed consent paper, the consent forms for taking part in the study and on data security as well as the documentation form.
Funding This work was supported by Deutsche Forschungsgemeinschaft and Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU) within the funding Open Access Publishing.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The ethics committee of the University of Erlangen-Nuremberg, Germany reviewed the study on eighth January 2019. After several clarifications within the consent forms of data security, participation and general participant information the study was approved on the ethics committee summit on 12th February 2019, the reference number is 473_18b.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon reasonable request.