Article Text

Abstract
Introduction Liver cirrhosis is the fifth largest cause of adult deaths, and a major complication, variceal bleeding is associated with a 1-year mortality of 40%. There is uncertainty on the first-line therapy for prevention of variceal bleeding owing to a lack of adequately powered trials comparing non-selective beta blockers, in particular carvedilol, with variceal band ligation.
Methods and analysis CALIBRE is a multicentre, pragmatic, randomised controlled, open-label trial with an internal pilot. The two interventions are carvedilol 12.5 mg od or variceal band ligation (VBL). Patients with liver cirrhosis and medium to large oesophageal varices that have never bled are eligible for inclusion. The primary outcome is any variceal bleeding within 1 year of randomisation. Secondary endpoints include time to variceal bleed, mortality, transplant-free survival, adverse events, complications of cirrhosis, health-related quality of life, use of healthcare resources, patient preference and use of alternative or crossover therapies. The sample size is 2630 patients over a 4-year recruitment period, across 66 hospitals in the UK.
Ethics and dissemination The study has been approved by a National Health Service (NHS) Research Ethics Committee (REC) (reference number 18/NE/0296). The results of this trial will be submitted for publication in a peer reviewed journal. Participants will be informed via a link to a preview of the publication. A lay summary will also be provided via email or posted to participants prior to publication (ISRCTN reference number: 73887615).
- cirrhosis
- portal hypertension
- oesophageal varices
- gastrointestinal bleeding
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Existing research and current practice
Liver disease is the fifth largest cause of adult deaths,1 2 with mortality predicted to double in 20 years.1 Patients with liver disease die younger with the average age of death of 59 years, compared with 82–84 years for heart and lung disease and stroke.1 One of the major complications of cirrhosis is portal hypertension and variceal bleeding. In patients with cirrhosis, varices develop at a rate of 5% per year with 10 year cumulative incidence of 44%.3 At least 3000 patients are admitted to hospital in England per year with variceal bleeding, with inpatient mortality of 15% and 1-year mortality of up to 40%. Increased hospitalisation results in increased use of secondary care and substantial healthcare costs. Since many patients are of working age there are also significant societal implications. Therefore, reducing the risk of the first variceal bleed (primary prevention) is an important clinical and economic goal.
At present, there are two options for primary prevention of variceal bleeding, namely non-selective beta-blockers and variceal band ligation. Beta-blockers used for portal hypertension in the UK are propranolol and carvedilol. A Cochrane review and meta-analysis of 19 trials (with a total of 1504 patients) comparing variceal band ligation versus beta-blockers showed a reduced risk of variceal bleeding with variceal band ligation (risk ratio, 0.67; 95% CI 0.46 to 0.98) with no effect on survival.4 However, the overall quality of evidence was low to moderate. When only high quality trials (seven trials, 713 patients) with minimal bias and sufficient follow-up were studied, the difference in bleeding rates was no longer evident. In another meta-analysis, although adverse events were more frequent with beta-blockers (OR 2.61, 95% CI 1.60 to 4.40, p<0.0001), fatal adverse effects were significantly lower with non-selective beta-blockers (NSBB; OR 0.14, 95% CI 0.02 to 0.99, p<0.05).5 The fatalities relate to banding induced bleeding from ulcers. No adverse events from beta-blockers such as symptomatic hypotension, dyspnoea and gastrointestinal upset directly resulted in death.
Trial rationale
The main focus of the research is the comparison of beta-blockers and variceal band ligation in the prevention of the first variceal bleed. There have been two important guidelines published in the UK in 2015–2016 from NICE and the British Society of Gastroenterology (BSG).3 6 NICE favours banding for primary prevention, whereas the BSG suggests banding if the patient is intolerant of beta-blockers. The recommendations of the BSG guidelines are similar to those of international guidelines.7 8 Therefore, there is at present disparity in the current guidelines with regard to first-line therapy for primary prevention.
Many specialists have significant concerns about the adverse effects of variceal band ligation, in particular the risk of banding induced bleeding.4 5 There are also concerns about the use of beta-blockers in patients with advanced cirrhosis with some studies showing higher mortality9 10 while others report improved survival.11 In particular with carvedilol, improved survival has been suggested.12 None of these studies are randomised trials and are therefore limited by their designs and the potential for confounding and other biases.
Data on cost effectiveness in the context of primary prevention are available from just one publication.13 This suggested beta-blockers have reduced overall costs compared with variceal band ligation. However, in the 2016 National Institute for Health and Care Excellence (NICE) cirrhosis guidelines, after extrapolation of the meta-analysis showing less bleeding with variceal band ligation, variceal band ligation was found to be more cost effective.6 There are no cost effectiveness studies alongside a randomised controlled trial (RCT) comparing carvedilol with variceal band ligation.
A large RCT at this time would help clinicians decide on the best treatment in terms of clinical and cost-effectiveness, as the current evidence is based on underpowered and low-quality trials as detailed above.
Carvedilol has been selected as the beta-blocker for this trial. Carvedilol is a well-tolerated non-selective beta-blocker which reduces portal blood flow, and in addition has vasodilating actions due to alpha-1 receptor blockade. The latter helps to reduce portal pressure further, mainly through the effects on intrahepatic resistance. Haemodynamic studies demonstrate a greater reduction in portal pressure than propranolol, and carvedilol can be effective even in patients not responding to propranolol.14 Carvedilol also has pleiotropic anti-inflammatory, antioxidant and antifibrotic properties along with other roles in enhancing insulin sensitivity and improving mitochondrial function that may provide additional benefits in patients with cirrhosis.15 Propranolol is not always well tolerated, and a third of patients fail to achieve a satisfactory reduction in portal pressure. Nadolol is not commonly used in the UK and has similar haemodynamic efficacy as propranolol. Therefore, there is considerable interest in alternatives to propranolol/nadolol, such as carvedilol.
There are only two RCTs of carvedilol versus variceal band ligation in primary prevention.16 17 The first trial from the UK of 152 patients showed significantly reduced bleeding in the carvedilol arm (10% vs 23%, relative hazard 0.41; 95% CI 0.19 to 0.96), with no apparent effect on survival (35% vs 37%, relative hazard 0.91; 95% CI 0.53 to 1.55).17 The second trial from Pakistan of 168 patients did not show any differences in bleeding (8.5% vs 6.9%, relative hazard 1.61; 95% CI 0.27 to 9.69) or mortality (12.8% vs 19.5%, relative hazard 1.53; 95% CI 0.71 to 3.30).16 In the first trial, patients were randomised after endoscopy with delays in the first banding session, leading to a lead time bias against band ligation as a second endoscopy session was required. CALIBRE endeavours to minimise this bias by randomisation mainly at the time of endoscopy. Compliance with variceal band ligation was better in the second trial, but significantly more patients had viral hepatitis than alcohol-related cirrhosis which does not reflect the disease burden of the UK. A recent randomised placebo controlled trial of 140 patients showed that carvedilol reduced progression of varices over a minimum of 24 months follow-up in patients with small varices, with no difference in bleeding or survival.18 Furthermore, the Mayo group recently performed a network meta-analysis which recommends further larger prospective trials of carvedilol in cirrhosis to investigate its potential benefits.19
The results of this trial will provide high-quality data with adequate power and follow-up. If carvedilol is found to be superior to variceal band ligation, then it will become first-line therapy in primary prevention. The trial will also provide a unique cohort for extended follow-up, since consent will be sought to use routine long-term data. This will help us understand the long-term impact of beta-blockers. It is plausible that survival may be better with carvedilol than variceal band ligation as suggested in a study of beta-blockers in secondary prevention.20 If this is true, it will lead to a paradigm shift in primary prevention of variceal bleeding. Such a finding will also encourage further translational research into the underlying mechanisms, which could help stratify patients most likely to benefit from beta-blockers and offer alternative therapies to non-responders.
Beta-blockers as first-line therapy in primary prevention will lead to a large change in practice as NICE guidance presently recommends variceal band ligation. Beta-blockers require much less National Health Service (NHS) resources than variceal band ligation for primary prevention, which usually requires at least 3–5 treatments to eradicate varices followed by indefinite endoscopic surveillance. There is no requirement for patients on carvedilol for primary prevention to undergo endoscopic surveillance.3 Bed pressures for other elective procedures could be eased and waiting times improved.
Internal pilot trial
The first 12 months of the CALIBRE trial will constitute an internal pilot, to assess and confirm logistics, and to determine if it is both feasible and practical for the trial to continue. Integrated qualitative research with patients and staff will contribute to assessments of feasibility and acceptability as detailed later. The qualitative research could lead to changes in the trial protocol as necessary to minimise potential barriers to recruitment and facilitate recruitment in the main trial. The results of the internal pilot will be assessed by the Data Monitoring Committee (DMC), Trial Steering Committee (TSC) and the funder.
Primary objective
The primary aim of this study is to compare carvedilol versus variceal band ligation in preventing any variceal bleeding within 1 year of randomisation in patients with cirrhosis and medium to large oesophageal varices that have never bled.
Secondary objectives
These include the effect of carvedilol and variceal band ligation on survival, development of other complications of cirrhosis and adverse events. The study will also investigate cost-effectiveness, patient preference and use of alternative or cross over therapies.
Methods and analysis
CALIBRE trial design
CALIBRE is a multicentre, pragmatic, randomised controlled, open-label trial with an internal pilot. Approximately 66 Acute NHS Trusts/Health Boards in the UK will be involved in trial recruitment. The detailed trial design is described below.
Eligibility criteria
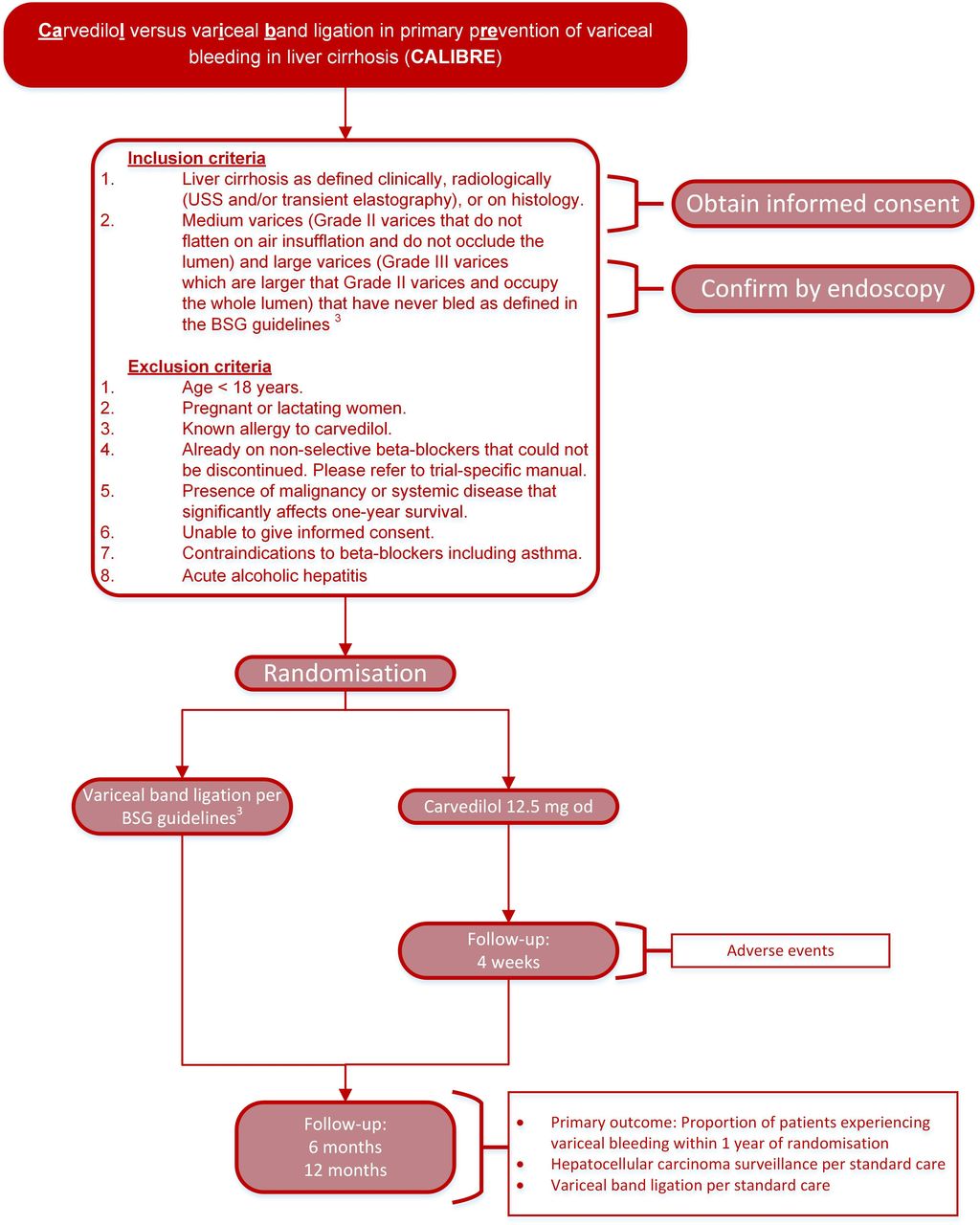
To be eligible for CALIBRE, a patient must have cirrhosis, and medium varices (Grade II varices that do not flatten on air insufflation and do not occlude the lumen) or large varices (Grade III varices which are larger than Grade II varices and occupy the whole lumen) that have never bled as defined in the BSG guidelines.3 Detailed inclusion and exclusion criteria are illustrated in figure 1. Patients with portal vein thrombosis of any grade can be included in CALIBRE. Patient who are on propranolol, carvedilol or nadolol for primary prevention or those that have had band ligation will be excluded.

Trial schema.
Recruitment
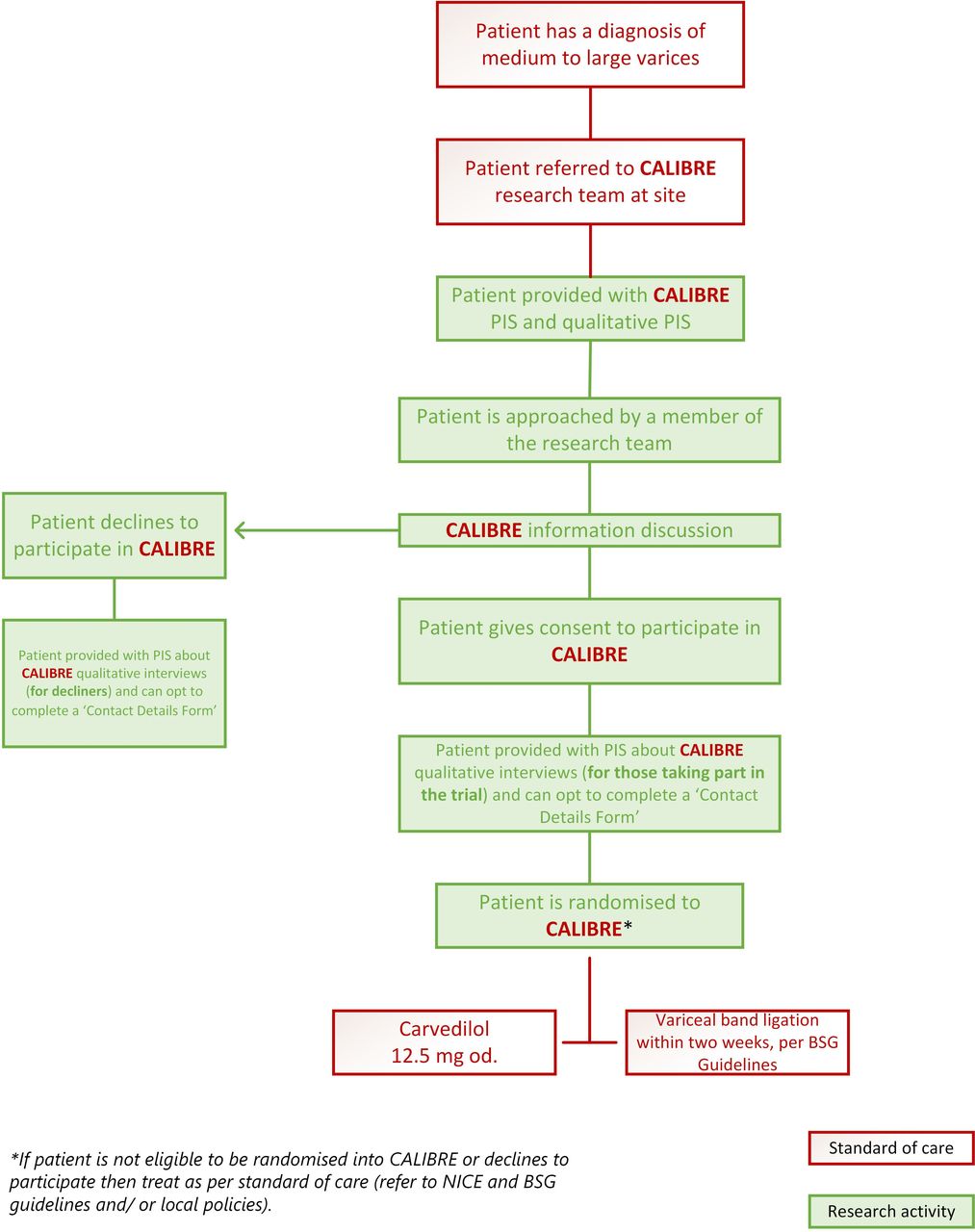
Participants may be identified and recruited in one of the following ways (figures 2–4):

Consent process (planned endoscopy where no diagnosis of varices has yet been made).
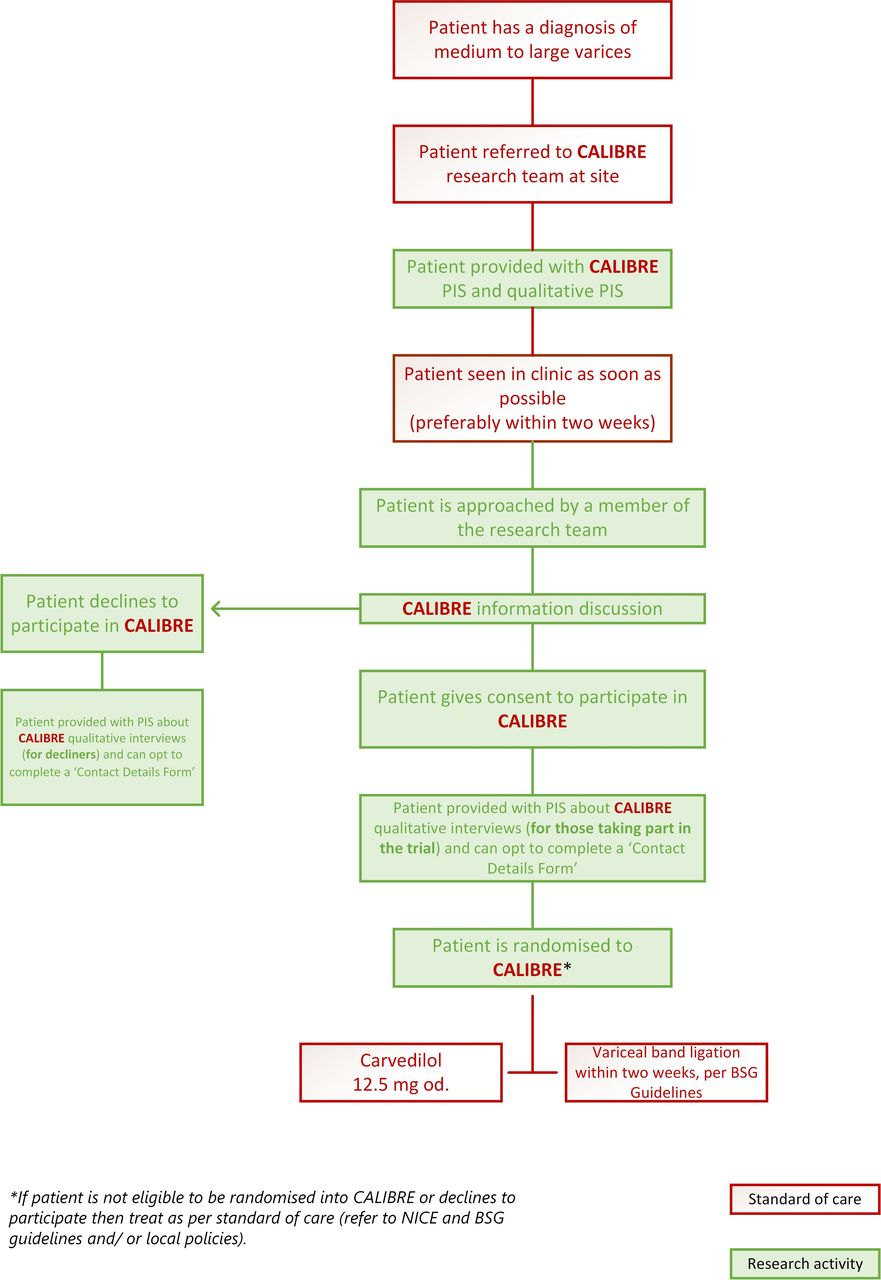
Consent process following referral from an outpatient clinic following diagnostic endoscopy.

Consent process following an inpatient referral.
By their Hepatologist, Gastroenterologist or Research Nurse in advance of standard of care variceal surveillance endoscopy.
Referral from an outpatient clinic following a diagnostic endoscopy.
Identification from inpatient referrals.
Patient enrolment is expected to start in early 2019 and expected to end in 2022.
Randomisation
Randomisation will be provided by a secure 24 hours online randomisation system at Birmingham Clinical Trials Unit (BCTU), supplemented by a telephone randomisation service.
After participant eligibility has been confirmed and informed consent has been received, the participant can be randomised into the trial. A randomisation form will be provided to investigators and will be used to collate the necessary information prior to randomisation. All questions and data items on the randomisation form must be answered before a trial number can be given. If data items are missing, randomisation will be stopped, restarting once the information is available. Only when all eligibility criteria and baseline data items have been provided will a trial number be allocated.
Participants will be randomised at the level of the individual in a 1:1 ratio to either treatment with 12.5 mg carvedilol once daily or variceal band ligation. Both of these treatments will start on the same day as randomisation or as soon as possible after. Patients randomised in clinic after a previous diagnostic endoscopy will be started on carvedilol 12.5 mg od or variceal band ligation within 2 weeks of randomisation. A minimisation algorithm will be used within the online randomisation system to ensure balance in the treatment allocation over the following variables: presence or absence of hepatic decompensation (ascites or encephalopathy), size of the largest varix (Grade II or Grade III), age of patient at randomisation (18–50, 51–70, >70) and presence or absence of alcohol-related liver disease.
A ‘random element’ will be included in the minimisation algorithm, so that each patient has a probability (unspecified here), of being randomised to the opposite treatment that they would have otherwise received. Full details of the randomisation specification will be stored in a confidential document at BCTU.
Trial treatment/intervention
Carvedilol
Participants will be prescribed 12.5 mg od. They will be seen in a follow-up clinic at 4 weeks to assess for any short-term adverse events such as symptomatic hypotension, gastrointestinal side effects like nausea, swelling of hands and feet, blurred vision, lethargy, headache, sexual dysfunction and shortness of breath.3 These patients will not be offered routine endoscopic surveillance, as per standard of care.3 Participants will be asked about adherence with their trial medication at each follow-up visit and their response documented in the medical notes and subsequently transcribed onto the Follow-Up Case Report Forms (CRFs).
Variceal band ligation
The procedure will be performed as per the BSG guidelines.3 Adherence to variceal band ligation will be documented on the Follow-Up CRFs using information available in the participant’s medical notes.
Treatment modification
Figure 5 outlines the process for treatment modifications in the event of intolerance. At clinician’s discretion, participants that are intolerant of carvedilol or variceal band ligation can be crossed over to the other arm at any point.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Process for treatment modifications in the event of intolerance.
Outcome measures and study procedures
Primary outcome
Any variceal bleeding within 1 year of randomisation. The first variceal bleed is defined as hematemesis and/or melena with either: (1) endoscopic evidence of variceal bleeding or stigmata of recent haemorrhage and at least a 2 g/L reduction in haemoglobin within 24 hours of admission or (2) massive upper gastrointestinal bleeding leading to death. The definition includes bleeding from banding ulceration.3
Secondary outcomes
Time to first variceal bleed in days (from randomisation).
Mortality at 1 year (from randomisation):
All-cause mortality.
Liver related mortality.
Cardiovascular mortality.
Transplant free survival at 1 year (from randomisation).
Adverse events related to treatment (up to 12 months after randomisation):
Dysphagia requiring discontinuation of treatment.
Symptomatic hypotension requiring change in treatment.
Dyspnoea.
Gastrointestinal upset.
Other complications of cirrhosis:
New onset ascites confirmed clinically or on imaging and graded as per International Club of Ascites recommendations.21
New onset encephalopathy defined using West Haven Criteria.22
Spontaneous bacterial peritonitis.
Hepatocellular carcinoma.
Any renal dysfunction as per International Club of Ascites—Acute Kidney Injury (ICA-AKI) definitions.23
Health-related quality of life (EQ-5D-5L) from randomisation to 6 and 12 months.
Use of healthcare resources, costs and cost-effectiveness based on the outcomes of cost per variceal bleeding avoided within 1 year of randomisation, cost per Quality-adjusted Life-year (QALY) estimated using the EQ-5D-5L and cost per death avoided at 1 year.
Patient preference. We will conduct qualitative interviews with patients and staff during the pilot phase. These interviews will explore patients’ experience of and preferences related to treatment (Carvedilol or VBL). This will provide the basis to describe qualitatively patients’ experience of the trial interventions. These qualitative data will complement quantitative outcome assessment.
Use of alternative therapies.
Crossover therapies.
Statistical considerations
Sample size
The sample size calculation has been based on published data from both a Cochrane review and meta-analysis of variceal banding versus beta-blockers4 and data from the first UK RCT of carvedilol published in this disease area.17 The Cochrane meta-analysis reported an overall 1-year variceal bleeding rate of 12% in the variceal banding ligation group. The 1-year bleeding rate was chosen for the primary outcome as Kaplan-Meier curves suggest that the majority of variceal bleeding occurs in the first year after treatment.17 To detect a 33% proportional difference in variceal bleeding rates (ie, from 12% to 8%, a 4% absolute difference) between groups using a 2-sided test for comparison of proportions with a 1:1 allocation ratio, 90% power and a type I error rate of 5% (ie, α=0.05), requires 2362 participants (1181 per group). Assuming and adjusting for a 10% attrition/loss to follow-up rate (based on the similar patient population,17 which is thus a conservative estimate due to our shorter duration of follow-up), increases the required sample size to 2630 participants in total (1315 per group).
Analysis of outcome measures
A separate Statistical Analysis Plan (SAP) will be produced and will provide a more comprehensive description of the planned statistical analyses. A brief outline of these analyses is given below.
The primary comparison groups will be composed of those randomised to carvedilol versus those randomised to variceal band ligation. All analyses will be based on the intention-to-treat principle, that is, all participants will be analysed in the group to which they were allocated irrespective of compliance with the randomised allocated treatment or other protocol violations. For all major outcomes, summary statistics and differences between groups (eg, mean differences, relative risks) will be presented, with 95% CIs and p values from 2-sided tests also given. Treatment effects will be adjusted for the minimisation variables. P<0.05 will be considered statistically significant and there will be no adjustment for multiple testing.
Primary outcome measures
The primary outcome measure of the study is variceal bleeding within the first year after randomisation. This outcome is a binary outcome (ie, yes/no). The number and percentage of participants experiencing variceal bleeding within 1 year of randomisation will be reported by treatment group. An adjusted relative risk and 95% CI will be estimated from a log-binomial model to take into account the minimisation variables.
The p value from the associated χ² test will be produced and used to determine statistical significance.
Secondary outcome measures
The secondary outcomes for the trial include continuous, categorical and time-to-event data items.
Time-to-event outcomes (eg, time to first variceal bleed)
Time to event outcomes will be compared between treatment groups using standard survival analysis methods. Kaplan-Meier survival curves will be constructed for visual presentation of time-to-event comparisons. Cox proportional hazard models will be fitted to obtain adjusted treatment effects which will be expressed as HRs with 95% CIs.
Categorical outcomes (eg, dysphagia requiring discontinuation of treatment)
For binary secondary outcomes, the number and percentage of participants reporting each outcome will be reported by treatment group. An adjusted relative risk and 95% CI will be estimated from a log-binomial regression model. The p value from the associated χ² test will be produced and used to determine statistical significance.
Continuous outcomes (EQ-5D-5L)
Continuous outcomes will be reported using means and SD. The EQ-5D-5L will be compared between treatment groups with adjusted mean differences and 95% CIs estimated using linear regression models. Change in EQ-5D-5L score from baseline will also be modelled.
Economic evaluation
A separate Health Economics Analysis Plan will be produced, providing a comprehensive description of the planned economic evaluation. Briefly, a within-trial analysis will be conducted from a National Health Service and Personal Social Services (NHS/PSS) perspective to calculate cost per variceal bleed avoided, cost per QALY gained and cost per death avoided. If evidence from the trial shows differences in terms of important outcomes (eg, rebleeding or mortality) that have significant cost or outcome implications beyond the trial period, a model-based economic evaluation will additionally be conducted.
Analysis of qualitative data
During the internal pilot, interviews will be recorded with the consent of participants and transcribed clean verbatim for analysis. Analysis will be conducted with reference to recordings, transcripts and field notes taken at the time of data collection. A thematic analysis of content will be informed by the Framework analytical approach.24 Following initial familiarisation with the interview data, development of thematic frameworks and data coding will proceed in an iterative manner. Data collection and analysis will run concurrently so that emergent analytical themes can inform further data collection, and particularly comparative analytical questioning between patients allocated to carvedilol and variceal band ligation.
Planned subgroup analyses
Subgroup analyses will be limited to the same variables used in the minimisation algorithm. Subgroup analyses will be limited to the primary outcome. Tests for statistical heterogeneity will be performed prior to any examination of effect estimates within subgroups. The results of subgroup analyses will be treated with caution and will be used for the purposes of hypothesis generation only.
Missing data and sensitivity analyses
Every attempt will be made to collect full follow-up data on all study participants, and it is thus anticipated that missing data will be minimal. Participants with missing primary outcome data will not be included in the primary analysis in the first instance. This presents a risk of bias, and sensitivity analyses will be undertaken to assess the possible impact of the risk. In brief, this will include worst-case assumptions and/or multiple imputation methods. Further sensitivity analyses will include an analysis on the per-protocol population and an unadjusted analysis. Any sensitivity analyses will not, irrespective of their differences, supplant the planned primary analyses. Full details will be included in the SAP.
Planned interim analyses
Interim analyses of major outcome measures and safety data will be conducted and provided in strict confidence to the independent DMC. Details of the agreed plan will be written in the SAP.
Planned final analyses
The final analysis for the study will occur once all participants have completed the 1-year assessment, and the corresponding outcome data have been validated as ready for analysis.
Ethics and dissemination
Ethical considerations
CALIBRE was granted ethical approval by the North East—York Research Ethics Committee (REC), reference number: 18/NE/0296. The trial will be conducted in accordance with the UK Policy Framework for Health and Social Care Research 2017, the applicable UK Statutory Instruments (which include the Medicines for Human Use Clinical Trials 2004 and subsequent amendments and current UK Data Protection Regulations). This trial will be carried out under a Clinical Trial Authorisation (CTA) in accordance with the Medicines for Human Use Clinical Trials regulations.
Dissemination
Results of this trial will be submitted for publication in a peer reviewed journal. The manuscript will be prepared by the CI or delegate and authorship will be determined by the trial publication policy. Participants will be informed of the outcome of the trial via a link to a preview of the publication. A lay summary will also be provided via email or posted to participants prior to publication.
Acknowledgments
We would like to thank the British Society of Gastroenterology (BSG) and British Association for the Study of the Liver (BASL) for supporting CALIBRE and reviewing the protocol.
References
Footnotes
Contributors DT is Chief Investigator and involved in all aspects of protocol design and lead author of the manuscript. PH, PR, IR and JF assisted in design of the protocol in particular clinical aspects. PD is lead for patient involvement in protocol design, with particular contributions to clinical aspects and consent pathways. In this role, he was assisted by JWF. JM is lead for the qualitative aspects of the protocol. In this role, he was assisted by CP. SJ is lead for heath economic aspects of the protocol. PB is involved in all aspects of protocol design, with particular attention to methodology. KH is lead for the statistical aspects of the protocol. MG, GS and KA reviewed the protocol with particular attention to management and operations. All authors reviewed and approved the final manuscript.
Funding This paper presents independent research funded by the UK National Institute for Health Research (NIHR) Health Technology Assessment (HTA) programme.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the National Health Service (NHS), the NIHR or the Department of Health and Social Care.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.