Article Text

Abstract
Objectives To assess factors associated with renal dysfunction (RD) in hepatitis C virus (HCV) cirrhosis, correlate renal parameters with Child-Pugh score (CPS) and find a cut-off value of CPS to determine RD.
Materials and methods It was a cross-sectional study that included 70 cases of liver cirrhosis secondary to HCV from a period of 6 months at Combined Military Hospital, Multan. Diagnosis of HCV was confirmed by serological assay and liver cirrhosis by ultrasonography. CPS was determined and lab reports were taken. Patients were divided into two groups as not having RD (serum creatinine≤1.5 mg/dL) and having RD (serum creatinine≥1.5 mg/dL). Estimated glomerular filtration rate (eGFR) was calculated by chronic kidney disease epidemiology collaboration (CKD-EPI) formula. Data were analyzed using SPSS V.23.0. χ2, Kruskal-Wallis test and Pearson coefficient of correlation were applied. ROC curve was drawn to evaluate cut-off value of CPS for the presence of RD. Level of significance was set at p<0.05.
Results Patients with CP grade B or C develop RD as compared to patients with CP grade A (p=0.000). Mean age, urea, creatinine and eGFR varies significantly among patients who develop RD and patients who do not (p=0.02, p=0.000, p=0.000 and p=0.000, respectively). eGFR negatively correlates with CPS (r=−0.359, p=0.002). Creatinine, urea and ALBI score positively correlates with CPS (r=+0.417, p=0.000; r=+0.757, p=0.000; r=+0.362, p=0.002, respectively).
Conclusion Ascites and encephalopathy are associated with RD in HCV cirrhosis.
- hepatorenal syndrome
- liver cirrhosis
- hepatitis C
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Renal involvement in liver cirrhosis is a well-known phenomenon. Child-Pugh score (CPS) is used to predict the severity of liver dysfunction. However, creatinine levels are used to determine the severity of renal dysfunction (RD).
What are the new findings?
The present study has highlighted a correlation between RD and severity of liver dysfunction measured by CPS in patients with hepatitis C-related liver cirrhosis. A cut-off value of 8.5 of CPS has a sensitivity of 80% and specificity of 60% to predict renal involvement in hepatitis C-related liver cirrhosis.
How might it impact on clinical practice in the foreseeable future?
The cut-off value of 8.5 of CPS can be used to predict the need for diuretic prescription and to monitor the extent of RD.
Introduction
Hepatitis C is a liver disease that is caused by hepatitis C virus (HCV), which can cause both acute and chronic hepatitis.1 Hepatitis C is a major health problem worldwide.2 3 Approximately 170 million2,3 to more than 185 million4 people are infected globally with a worldwide prevalence of 2.8%.4 Hepatitis C is becoming an increasing social, economic and health burden.2 3 In Pakistan, the prevalence of HCV is from 5%5 to 6.8%,4 which is the second highest in the entire world.6 About 15%–30% of patients with hepatitis C progress to cirrhosis after 20 years of disease.1 Approximately, 399 000 people die from liver cirrhosis or hepatocellular carcinoma caused by hepatitis C.1 About 15%–45% patients infected with HCV recover within 6 months without any treatment whereas the rest 60%–80% become chronically infected.1
Renal failure is a common complication of decompensated liver cirrhosis.7–14 About 40%–49% of patients with liver cirrhosis requiring intensive care eventually develop renal failure.7 13 However, 24% of outpatients with liver cirrhosis develop renal failure within 1 year of developing ascites.11–14 According to healthcare personnel, the development of renal failure in patients with liver cirrhosis is associated with significant morbidity and mortality and hence, the diagnosis of renal failure in liver cirrhosis should be early and accurate so that specific treatment be initiated to improve the outcome.12 15 16
There is a spectrum of factors causing acute kidney injury (AKI) in liver cirrhosis including (1) prerenal AKI, which is caused by hypovolaemia due to gastrointestinal bleeding, aggressive diuretic treatment and lactulose-induced diarrhoea or infections, (2) the hepatorenal syndrome-type AKI (HRS-AKI), which is a potentially reversible decline in renal function unresponsive to volume resuscitation, (3) intrinsic causes, such as acute tubular necrosis, and (4) postrenal causes.15 17–20 In short, the mechanism of HRS has been explained by increased formation of vasoconstrictors and decreased formation of vasodilators and significant decline in glomerular filtration rate (GFR).21 22
Child and Turcotte first gave a scoring system to predict operative risk in patients undergoing portosystemic shunt surgery for variceal bleeding. Initially, it included ascites, hepatic encephalopathy (HE), nutritional status, total bilirubin and albumin but later, it was modified by Pugh et al who added prothrombin time or international normalised ratio and removing nutritional status. Child-Pugh score (CPS) has been useful to find the severity of liver dysfunction in the clinical setting.23 24
The objectives of this study were to determine:
the factors associated with renal dysfunction (RD),
the correlation between the severity of RD and extent of liver damage and
the cut-off value of CPS to predict RD in patients with HCV-induced liver cirrhosis.
Materials and methods
This cross-sectional study included 70 cases of liver cirrhosis secondary to hepatitis C infection from a period of January 2018 to June 2018 at Combined Military Hospital, Multan on patients recruited using consecutive non-randomized sampling technique. We included all the patients from inpatient and outpatient department having hepatitis C-induced liver cirrhosis who were aged ≥18 years. Patients having a history of diabetes, diuretic use, hypertension, chronic kidney disease, an abnormal urinalysis, abnormal renal ultrasound and liver cirrhosis secondary to other causes were excluded. There was no patient with alcoholic hepatitis in our study, so no difficulty was encountered in measuring serum creatinine in patients with high bilirubin levels. Diagnosis of HCV was confirmed by serological assay and liver cirrhosis was confirmed by ultrasonography. CPS was determined and lab reports were taken on the same day. RD associated with HCV-induced liver cirrhosis was detected in the patients on study inclusion by serum creatinine at the time of admission. Guidelines of the International Ascites Club’s definition were used to define patients having RD on the basis of serum creatinine.25 Patients were divided into two groups as having RD (serum creatinine≥1.5 mg/dL) and not having RD (serum creatinine<1.5 mg/dL). Estimated GFR (eGFR) was calculated by CKD-EPI collaboration formula.26 HE was diagnosed clinically by an experienced consultant. Grading of HE was done according to grades mentioned in Davidson’s Principles and Practice of Medicine.27 Ascites was detected by clinical examination and confirmed by ultrasonography.
Data were analysed using SPSS V.23.0. Normality of quantitative variables was checked by Kolmogorov-Smirnov and Shapiro-Wilk tests. Quantitative variables were described by means in case of normal distribution and medians in case of asymmetric distribution. Qualitative variables were described by their frequencies. χ2, Kruskal-Wallis test and Pearson coefficient of correlation was applied. ROC curve was drawn to evaluate cut-off value of CPS for presence of RD. Level of significance was set at p<0.05.
Results
Out of 70 patients with liver cirrhosis, 56 (80%) were males while 14 (20%) were females. The median age was 55 years (IQR=15 years). A total of 40 out of 70 (57%) had ascites while the rest 30 (43%) did not develop ascites. About 30/70 (43%) had HE while the rest 40 (57%) did not. Out of 70 patients, 30 (43%) patients developed RD and 40 (57%) did not develop RD. Demographic details of the patients are presented in table 1. The distribution of patients having HE into the four grades is presented in table 2.
Demographic details (n=70)
Distribution of grades of hepatic encephalopathy in patients with HCV-induced liver cirrhosis (n=30)
Patients with ascites and encephalopathy are prone to develop RD (p<0.000, OR=32.6; p=0.012, OR=3.5, respectively). Frequency of RD is significantly higher in CP grade B or C patients as compared with patients with CP grade A (p<0.000). RD showed no significant association with gender (p≥1.00). These associations are presented in table 3.
Factors associated with renal dysfunction
Quantitative variables presented in table 4 were asymmetrically distributed, and their medians are reported and compared by Kruskal-Wallis test. The difference in medians of urea, creatinine, eGFR, age and CPS between patients who had developed RD and patients who did not was significant (p<0.000, p<0.000, p<0.000, p=0.02 and p=0.001, respectively), whereas the difference in serum total bilirubin and albumin was insignificant (p=0.064 and p=0.18, respectively).
Comparison of quantitative variables according to renal dysfunction
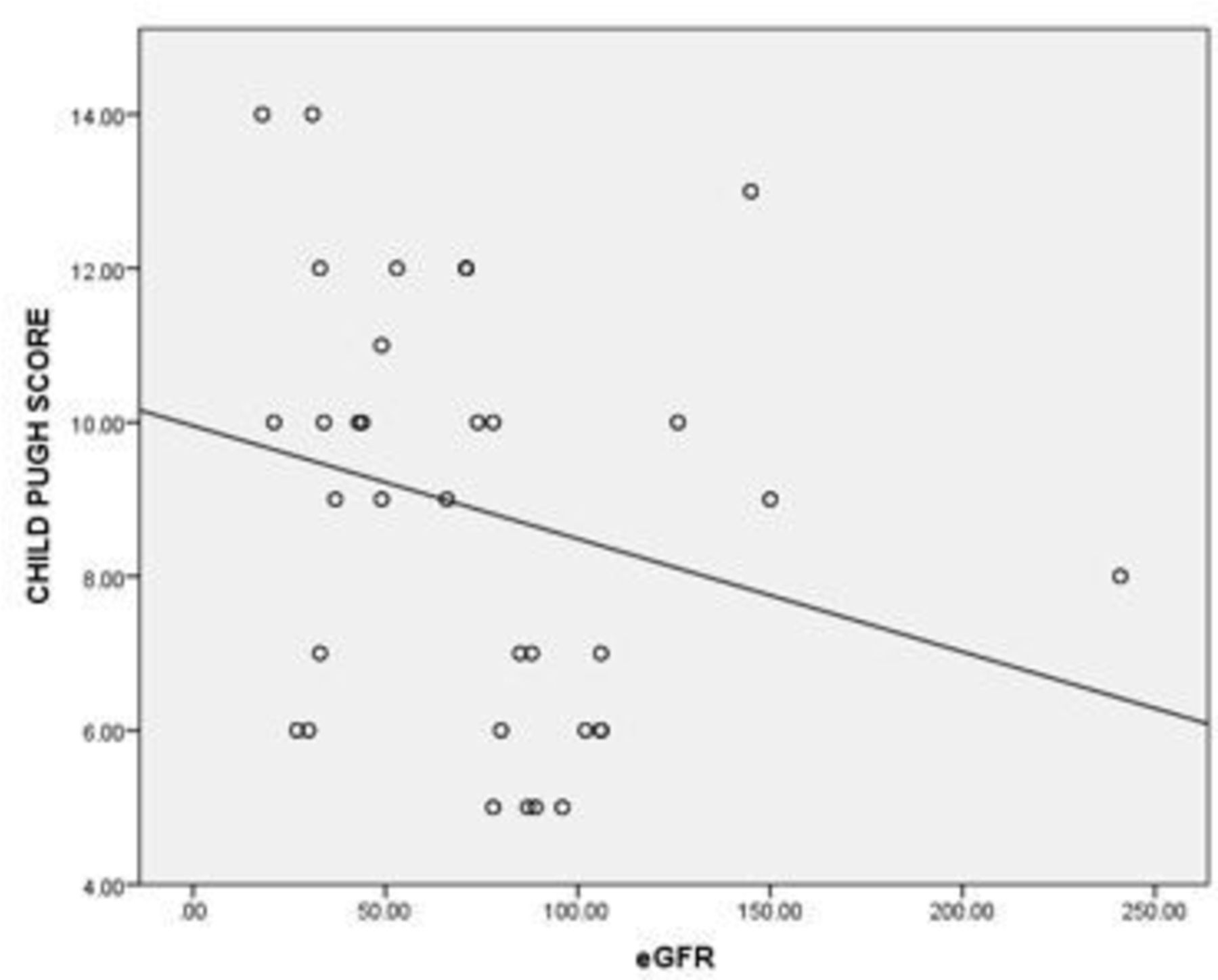
There was a strong positive correlation between serum creatinine and CPS (r=+0.757, p<0.000) (table 5) and inverse correlation between eGFR and CPS (r=−0.359, p=0.002) as shown in figure 1.

Correlation between eGFR and Child-Pugh score. eGFR, estimated glomerular filtration rate.
Correlation of eGFR and creatinine levels with Child-Pugh score
ROC curve was constructed for finding cut-off value of CPS at which RD develops. Area under ROC curve was 0.730 (p=0.001) for 95% CI. Cut-off value of 8.5 shows 80% sensitivity and 60% specificity as shown in figure 2.

{kind=link}
{kind=link}
ROC for cut-off point for Child-Pugh score for renal dysfunction (AUC=0.730).
Discussion
In countries where viral hepatitis is a health burden, liver cirrhosis has become an important health problem.28 Liver cirrhosis is accompanied by RD, especially in advanced liver disease. Reduced effective arterial blood volume and peripheral vasodilation cause haemodynamic alterations, which are followed by activation of vasoconstrictors, such as renin, aldosterone, vasopressin, endothelin and increased activity of neurohormonal systems.25
In our study, liver cirrhosis was more frequent in males (80%) than in females (20%). This was consistent with the study conducted by Siregar and Gurning, where 56.4% of males developed liver cirrhosis as compared with 43.6% females.29 However, according to another study, males with liver cirrhosis comprised 68.8% of total patients.30 This may be due to the fact that men are two times more likely to die from chronic liver disease as compared with women31 and women clear HCV infection more readily as compared with men.32 There is also a decreased risk of decompensated liver cirrhosis due to HCV in women as compared with men.33 However, there were only 14 females in our study as compared with 56 males so there may be a lack of sufficient power to strongly support this outcome. Hence, more studies should be conducted with an equal number of cases from both genders to support this.
The median age of cirrhotic patients in our study was 55 years. This is comparable to Siregar and Gurning, where the mean age was 51.51 years.29 However, according to another study, the mean age was 56.12 years.30 It has been shown in several studies that ageing increases the risk of liver fibrosis in hepatitis C infections.34–36
In our study, 43% of patients with liver cirrhosis developed RD, whereas in case of Siregar and Gurning,29 29.1% of patients developed RD and Mohan et al37 reported 22% of patients with RD in liver cirrhosis. Another study by Cheyron et al38 showed that AKI occurs in approximately 19% of hospitalised patients with cirrhosis.
Our study shows that patients with ascites and encephalopathy are prone to develop RD (p=0.000, OR=32.6; p=0.012, OR=3.5, respectively). About 30% of the patients with ascites and 60% of the patients with the encephalopathy developed RD. In the study by Siregar and Gurning,29 34.2% of the patients with ascites and 62.5% of the patients with HE developed RD (OR=1.28 and OR=5.45, respectively). These results are quite comparable to ours. Presence of ascites and encephalopathy are strong indicators of liver cirrhosis, which leads to kidney failure due to HRS. The activation of RAAS and sympathetic nervous system in the kidney causes sodium retention, which, in turn, causes ascites.25 Thus, both decrease synthesis of albumin by the liver in decompensated liver disease and development of HRS converge to produce fluid retention and thus, causing ascites.
RD showed no significant difference among gender because RD was equally prevalent in both males and females(43% in both genders). This was confirmed by Siregar and Gurning,29 where 29% males and 29.2% females with liver cirrhosis developed RD and gender was insignificantly associated with RD in liver cirrhosis. The difference in serum bilirubin (median=35.91 in RD and 23.47 in patients with no RD) and albumin (median=3.2 in RD group and 3.3 in non-RD group) between the patients who developed RD and those who did not develop it was also statistically insignificant in our study. However, Siregar and Gurning29 reported that mean serum bilirubin was insignificant among patients with and without RD (median=2.25 and 1.3, respectively) but the distribution of serum albumin (mean=2.7 and 1.92, respectively) was statistically significant between two groups. Our study shows that median levels of urea, creatinine, eGFR, age and CPS between patients who had developed RD and patients who did not was significant. Siregar and Gurning29 also showed that mean urea, creatinine and eGFR were significantly different among the patients with and without RD.
Our study showed a significant relationship between CPS and RD. RD was significant in patients with CP grade B and C (58%) as compared with those with grade A (0%). Siregar and Gurning29 also found that no one (0%) in grade A of liver cirrhosis developed RD whereas 37.2% of patients with grade B or C developed renal failure. This shows that higher the severity of cirrhosis greater will be the risk of renal injury. To prove this, we correlated the CPS with serum creatinine and eGFR and found a significant direct correlation between serum creatinine with CPS (r=0.757, p=0.000) and an inverse correlation with eGFR (r=−0.359, p=0.002). Siregar and Gurning29 also reported a positive correlation between serum creatinine and CPS (r=0.359, p=0.007) and an inverse correlation between eGFR and CPS (r=−0.308, p=0.022). This proves that higher the CPS greater will be the kidney injury, so greater will be the serum creatinine and lower will be the eGFR. Das et al39 also found that CPS and serum creatinine are significantly correlated with each other. Choi et al40 also showed that RD was much more common in patients with higher severity of liver cirrhosis.
In our study, we made an ROC curve to find the cut-off point of CPS at which RD can be predicted at maximum sensitivity and specificity and found that CPS of 8.5 shows 80% sensitivity and 60% specificity for detecting a disturbance in kidney function in patients with liver cirrhosis.
Conclusion
Ascites and encephalopathy are associated with RD in HCV cirrhosis. Patients with CP B and C are more prone to have RD as compared with CP A. Greater the CPS greater is the extent of renal injury. A cut-off value of CPS 8.5 is highly sensitive to predict RD in HCV-related liver cirrhosis and can be used as screening test due to high sensitivity. This may help in diuretic prescription for the patients and monitoring the extent of RD.
References
Footnotes
Contributors HWB planned and designed the study, and contributed in manuscript writing as well. UT contributed in data collection, entry and manuscript writing. NAC analysed the data, contributed in manuscript writing and reviewing the paper. SB contributed in data collection and quality assurance. MH contributed in data collection, technical supervision and patient selection. ZAR submitted the manuscript and did final review of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study is approved by the Institutional Research Forum of Rawalpindi Medical University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.