Article Text

Abstract
Pseudoachalasia, or secondary achalasia, is a clinical condition that must be distinguished from primary achalasia. Both diagnoses may present similarly, but the aetiology and management for each are drastically different. Most significantly, pseudoachalasia carries a high association with malignancy, most often with primary adenocarcinoma of the oesophagus or cardia. Our case involves a patient with signs and symptoms consistent with pseudoachalasia due to metastatic bladder cancer.
- pseudoachalasia
- bladder cancer
- achalasia
- dysphagia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Achalasia is a clinical diagnosis referring to incomplete relaxation of the lower oesophageal sphincter (LES) with impairment of oesophageal motility.1–5 There are two types of achalasia: primary and secondary. Primary achalasia is an idiopathic motility disorder. However, pseudoachalasia, or secondary achalasia, is primarily caused by malignancy or another secondary aetiology. Therefore, it necessitates early consideration and a timely diagnosis. Pseudoachalasia is generally found in older-aged patients (>60 years), with acute onset of dysphagia (<1 year), rapid progression of symptoms, and significant weight loss.1 5–9 Most cases of pseudoachalasia due to malignancy are from a gastrointestinal (GI) primary. However, there are a few cases that have reported pseudoachalasia secondary to a non-GI neoplasm via a paraneoplastic process. Herein this report, we discuss an atypical case of pseudoachalasia due to metastatic bladder cancer rather than primary GI malignancy.
Case report
An elderly female with a medical history significant for bladder cancer previously treated with BCG and chemoradiation presented with a 3-day history of worsening dysphagia to both solids and liquids. She was initially evaluated at an outside hospital where a non-contrast chest CT scan reportedly demonstrated a dilated oesophagus with a 4.3×2.7 cm mass at the gastro-oesophageal (GE) junction associated with retrocrural adenopathy concerning for an oesophageal malignancy. Oesophagogastroduodenoscopy (EGD) performed at the outside hospital revealed retained food in the mid-oesophagus with minor dilation of the proximal oesophagus and reported difficulty passing the upper endoscope through the GE junction. However, no masses or strictures were noted and no biopsies were taken at that time. The patient was then transferred to our institution for further management.
Repeat EGD performed on day 2 of admission showed similar findings to the outside hospital, including oesophageal dilation in the proximal and mid portions with a ‘tight’ LES and blanching of the GE junction mucosa—a release was felt as the scope passed into the stomach (popping sensation) (figure 1A,B). Biopsies taken from the GE junction showed focal intestinal metaplasia, yet again no signs of dysplasia/malignancy (figure 1C). The patient subsequently underwent a CT chest with intravenous contrast. The CT image demonstrated moderate dilation of the thoracic oesophagus tapering to the GE junction with thickening in the distal oesophagus/GE junction and an enhancing nodule along the anterior peritoneum/omentum concerning for carcinomatosis.
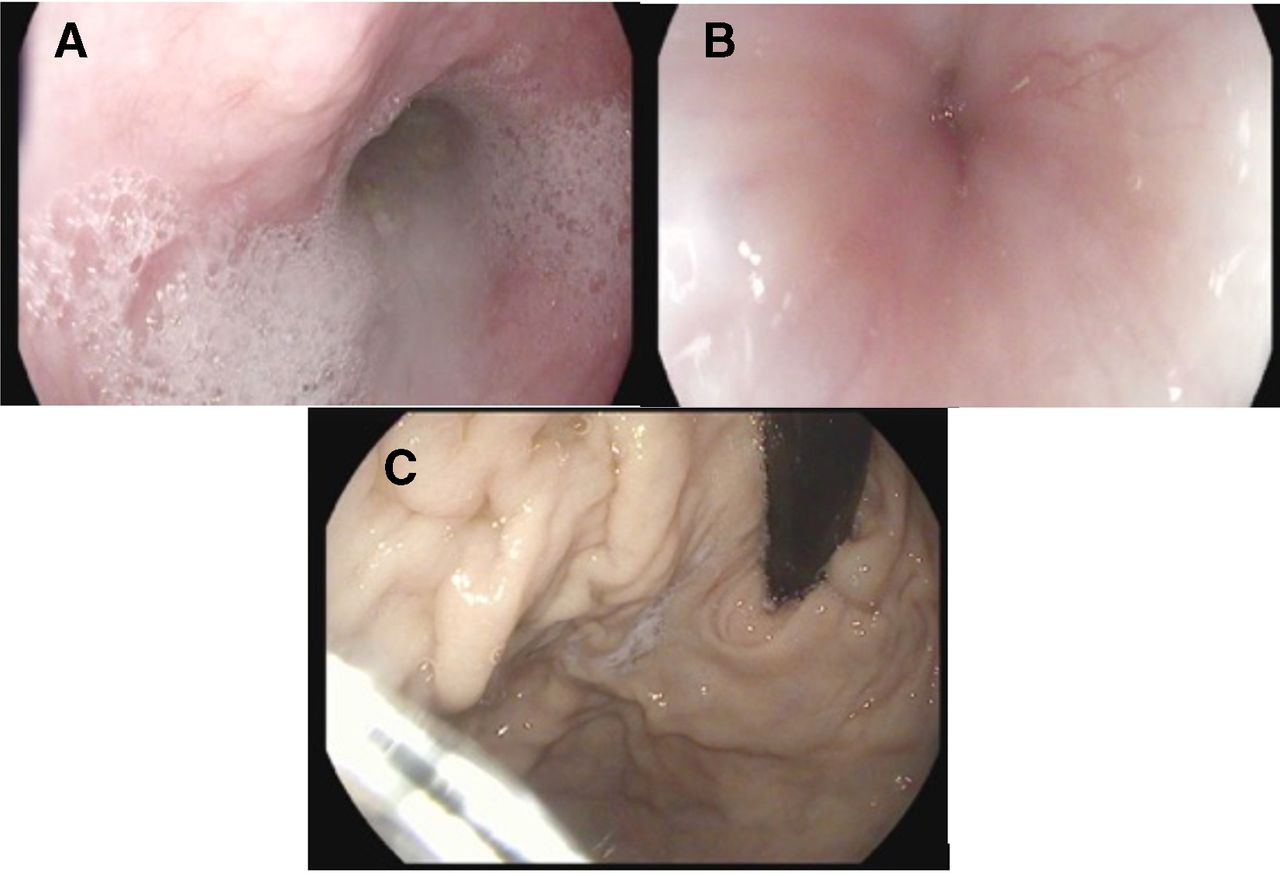
Oesophagogastroduodenoscopy (EGD) on admission. (A) EGD demonstrated dilation in the proximal and mid portions of the oesophagus. (B) EGD showed a narrowed lower oesophageal sphincter. (C) No masses were seen on retroflexed views of the stomach. Gastric biopsies showed focal intestinal metaplasia.
A follow-up endoscopic ultrasound (EUS) was performed on day 10 to better evaluate these radiographic findings. EUS revealed a ‘tight’ GE junction with near normal oesophageal wall layers. The radial EUS scope was unable to traverse the GE junction, so a standard upper endoscope was used. Gastric mucosa appeared normal. With the above negative findings, the patient underwent pneumatic dilation with a 30 mm Rigiflex balloon (figure 2). During the dilation, the gastric mucosa was noted to have thickened folds; however, biopsies were negative for dysplasia/malignancy at that time as well. Other secondary causes of achalasia were excluded including a negative western blot for Anti-Hu antibodies for paraneoplastic syndrome. Due to continued symptoms and still no confirmed malignancy, a follow-up EGD was performed. This EGD showed narrowing in the distal oesophagus extending from 34 to 41 cm from the incisors. This time, the area could not be traversed with the standard upper endoscope, a significant difference from the prior endoscopy (figure 3A). A paediatric scope was then used to pass into the stomach revealing significantly thickened, hypertrophied gastric folds in the body, with biopsies showing poorly differentiated adenocarcinoma consistent with her primary bladder cancer (figure 3B).

Day 10 oesophagogastroduodenoscopy for pneumatic dilation using a 30 mm Rigiflex balloon. The stomach had thickened folds with pale mucosa. Biopsies consistent with mild chronic inflammation but no evidence of malignancy.

{kind=link}
{kind=link}
{kind=link}
Day 16 oesophagogastroduodenoscopy (EGD). (A) EGD showed thickening of the distal oesophagus with narrowing of the lower oesophageal sphincter necessitating a paediatric scope to traverse the narrowing. (B) The gastric folds were thickened with areas of white streaks and the stomach was not easily distensible. Biopsies were consistent with poorly differentiated adenocarcinoma.
The patient rapidly deteriorated due to hypoxic respiratory failure and required transfer to the intensive care unit of hospital on day 22. The patient was found to have malignant bilateral pleural effusions with pathology also confirming metastatic bladder cancer. She had a rapid clinical deterioration and, unfortunately, expired during this hospital admission.
Discussion
Pseudoachalasia is a rare disease accounting for a small subgroup of patients with dysphagia. Most cases are associated with primary neoplasia at the GE junction, with greater than 50% of these cases being adenocarcinoma.6–8 Other primary malignancies reported include pancreatic, hepatocellular, prostatic, lung, mesothelioma, and lymphoma.5 10 Up to 25% of patients will have a false negative diagnostic biopsy on initial EGD, just as seen in this case.3 For this reason, it is important to recognise the constellation of symptoms for pseudoachalasia and perform follow-up biopsies to help guide therapy.
The proposed mechanism of pseudoachalasia is infiltration of the oesophageal wall by tumour cells that in turn cause malignant strictures at the LES. This results in proximal oesophageal dilation or secondary impairment of the inhibitory neurons of the oesophageal myenteric plexus. A secondary mechanism, that is much rarer, is a paraneoplastic syndrome with antineuronal nuclear antibodies involving the interaction of tumour factors with the oesophageal neuronal plexus without direct infiltration of the GE junction.6–8
While primary and secondary achalasia can both present with dysphagia, there are important distinguishing characteristics between the two diagnoses.9 As mentioned previously, pseudoachalasia is more often seen in an older population (>50 years) presenting with acute onset of symptoms that rapidly progress in addition to significant weight loss.1 5–9 Barium swallow can also provide clues to differentiate. As opposed to those with achalasia, pseudoachalasia typically has a narrowed distal oesophageal segment greater than 3.5 cm yet the degree of dilation above the narrowed segment is less than 4 cm. This is attributed to the long-standing obstruction in primary achalasia. Additional imaging of those with pseudoachalasia will often find a primary gastric adenocarcinoma or infiltrating metastatic carcinoma near the GE junction.6 Additionally, pseudoachalasia often demonstrates difficulty passing an endoscope through the GE junction and is associated with failure of conventional therapies for primary achalasia such as pneumatic dilation or amyl nitrite administration.1 4 6 Worth noting, pneumatic dilation can be dangerous in these patients due to increased risk for perforation and should be used sparingly.11 Interventions such as prophylactic percutaneous gastrostomy can be considered as both a bridge to chemotherapy or as palliation.
A review of the literature shows only two cases of primary bladder cancer causing pseudoachalasia, and our case would theoretically be the third reported example. Secondary achalasia in this patient is supported by her lack of response to pneumatic dilation, high resistance with passing of the upper endoscope through the GE junction, radiographic findings, and finally, the rapid progression of acuity of symptoms. In our case, we discovered the mass prior to the diagnosis of achalasia; however, we recommend strong awareness for pseudoachalasia in patients who meet criteria for achalasia but fail conventional therapy.
Footnotes
Contributors WH is responsible for writing and submitting the case report. SS performed both EGDs during hospitalisation and assisted in writing of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Author note Images are original to this case.