Article Text

Abstract
Objective Data on patterns and correlates of opioid and benzodiazepines prescriptions among patients with chronic conditions are limited. Given a diminished capacity for hepatic clearance, patients with cirrhosis represent a high risk group for use. The aim of this study was to characterise the patterns and correlates of prescription opioid, benzodiazepine and dual drug prescriptions among individuals with common chronic diseases.
Design Analysis of Truven Marketscan database to evaluate individuals with drug coverage with cirrhosis (n=169,181), chronic hepatitis C without cirrhosis (n=210 191), congestive heart failure (n=766 840) or chronic obstructive pulmonary disease (n=1 438 798). Pharmacy files were examined for outpatient prescriptions.
Results Patients with cirrhosis had a significantly higher prevalence of opioid prescriptions (37.1 per 100 person-years vs 24.3–26.0, p≤0.001) and benzodiazepine prescriptions (21.3 per 100 person-years vs 12.1–12.9, p<0.001). High dose opioid prescription (>90 daily oral morphine equivalents) (29.1% vs 14.4%, p<0.001) and dual opioid and benzodiazepine prescription (17.5% vs 9.6%–10.5 %, p<0.001) were also significantly more prevalent in cirrhosis. High dose opioid prescription was greater in men, individuals ages 40–59, in the Western USA, and among those with a mental health or substance abuse condition. Dual opioid and benzodiazepine prescription were highest among those with alcoholic cirrhosis and middle aged-adults.
Conclusion Persons with cirrhosis have significantly higher rates of prescription opioid and benzodiazepine prescription compared to others with chronic diseases despite their high risk for adverse drug reactions. Demographics and mental health or substance abuse history can help identify high risk groups to target interventions.
- alcoholic liver disease
- chronic liver disease
- cirrhosis
- hcv
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Prescription opioid and benzodiazepine use is highly prevalent and associated with increased morbidity and mortality in the general population.
Impact of these medications among patients with chronic liver disease (CLD) may differ due to their hepatic based metabolism.
There are very limited data on patterns and correlates of use of prescription opioids and benzodiazepines in chronic conditions including CLD.
What are the new findings?
In this large, nationwide database of insured US patients, we demonstrate that prescription of opioids, benzodiazepines and dual prescription are significantly higher in patients with cirrhosis than in individuals with other common chronic conditions (congestive heart failure and chronic obstructive pulmonary disease).
High dose opioid prescription is also most common in cirrhosis and aetiology of liver disease also appears to drive patterns of prescription.
How might it impact on clinical practice in the foreseeable future?
Patients with CLD, particularly those with alcoholic liver disease, are high utilisers of prescription opioids and benzodiazepines.
This prescription, particularly at the high doses used in this population, has been associated with higher rates of adverse clinical outcomes and thus targeted interventions to curb use in this high risk population should be implemented.
Introduction
Approximately 70.6 opioid prescriptions are filled per 100 persons in the USA each year.1 The overall rates of opioid prescriptions quadrupled between 1999 and 2015 with annual increases in associated adverse outcomes such as unintentional overdoses.2 While patterns of opioid use around acute conditions and surgical procedures have been extensively studied, little is known about opioid use among patients with chronic disease. In addition, many patients with chronic opioid use are also prescribed benzodiazepines, which when prescribed in combination with opioids, can increase the propensity for adverse clinical outcomes.3 4 Available data have suggested increases in rates of combined opioid and benzodiazepine use over the past few years at the population level.3 To date, however, there has been little to no characterisation of the prevalence of dual opioid and benzodiazepine use in chronic disease. A patient population at particular risk for harms associated with opioid and benzodiazepine use includes individuals with cirrhosis due to the hepatic-based clearance of both medications. As such, characterisation of rates and correlates of prescription opioid and benzodiazepine prescriptions in this cohort is of particular clinical importance.5
Multiple studies have identified liver disease as a primary risk factor for opioid-related overdose, respiratory and central nervous system depression.6 7 Opioid use among patients with cirrhosis has been associated with higher rates of hospital readmissions, concern for worsening hepatic encephalopathy and higher overall mortality.8 Despite the potentially higher risk for adverse side effects, in clinical practice patients with cirrhosis may be frequently prescribed these medications. Given the patterns of associated sociodemographic characteristics and comorbid conditions among many individuals with cirrhosis, these factors may also contribute to differential prevalence and patterns of use in this patient population compared with other relevant chronic conditions and thus warrant further investigation.
The true scope of this problem remains unknown however, as the precise prevalence and patterns of opioid and benzodiazepine use in patients with cirrhosis, particularly in comparison to rates seen in other common chronic diseases, has not been clearly characterised to date. Current estimates are highly variable and predominantly generated from small, single-centre retrospective studies. The prevalence rates for prescription opioid use in cirrhosis range from 25% to 77% and encompass heterogeneous patient subgroups including analyses restricted to hospitalised patients.8–13 Moreover, there has not been a clear evaluation of opioid and benzodiazepine use across different forms of chronic liver disease. As such, the aim of this study is to characterise opioid and benzodiazepine prescription among patients with cirrhosis and compare this with rates and patterns of prescription in other chronic diseases. In addition, we aimed to identify correlates of opioid and benzodiazepine prescription in patients with chronic disease.
Patients and methods
Study population
A nationwide longitudinal study was conducted using the 2009–2015 Truven Health Marketscan Commercial Claims and Encounters Database and the Medicare Supplemental Database. These data included patients in all 50 states who received health insurance coverage from a range of employer-based health plans. Deidentified outpatient pharmacy insurance claims were linked to ascertain medical encounters and medication prescription among insured employees and their dependents. For this study, we included patients with diagnoses codes indicating cirrhosis from any aetiology, chronic hepatitis C (HCV) without cirrhosis, congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD). Codes used for case identification are listed in the (online appendix 1). For this study, single ICD-9 codes were used to identify patients with cirrhosis based on validated algorithms using this approach that have been shown to have positive predictive values of ≥80%.14 15 Disease groups were mutually exclusive; there were no overlapping diagnoses across these four main categories of diseases in order to optimise comparison of rates of prescription. All patients included had continuous drug coverage over their inclusion period in the study. This study was determined to be exempt for requiring institutional review board approval and overall complies with ethical aspects of clinical research.
Supplemental material
Study outcomes and other covariates
Pharmacy files were examined for the use of prescription opioids and benzodiazepines. Opioids were identified as prescriptions found in the therapeutic drug class (inclusive list can be found in the Appendix). Daily opioid morphine equivalents (OME) were calculated based on the number of pills prescribed, the strength of the prescription and the morphine-equivalent conversion factor. OME has been recommended by the CDC to assess total opioid burden. High dose prescriptions were of interest and therefore, daily OMEs of 90 or greater were determined for each patient based on CDC categorisation for opioid prescription dosing.16
Demographics including age at the time of enrolment, gender and geographic region were included. There were no age restrictions, with age categorised by ≤18, 19–39, 40–59 and ≥60 years. Among individuals with cirrhosis, patients were further subcategorised according to aetiology of liver disease: alcoholic cirrhosis with HCV, alcoholic cirrhosis without HCV, non-alcoholic cirrhosis with HCV and all other types of cirrhosis. Clinical variables of interest included the Charlson comorbidity index, and presence of a mental health or substance abuse diagnosis occurring in the year before the index disease diagnosis (codes used for case identification outlined in online appendix.
Statistical analysis
Prevalence rates of opioid and benzodiazepine drug prescription (per 100 person-years) were calculated with Poisson exact CIs. The number of people prescribed opioids and benzodiazepines constituted the numerator with person-years of observation as the denominator (ie, enrolment period in healthcare coverage) for each of the disease categories. Median number of high-dose prescriptions (>90 daily OME) were determined, with IQR. Percentages of patients using high-dose prescriptions by disease category were evaluated by Pearson χ² tests. Correlates of the numbers of high dose (>90 daily OME) opioid prescriptions were assessed using negative binomial regression, offset by the natural log of the years under observation. For correlates of opioid and benzodiazepine prescription, the following variables were assessed: age, gender, region, history of substance abuse or mental health conditions, Charlson comorbidity index and aetiology of cirrhosis (among those with cirrhosis). Alpha was set at 0.05, 2-tailed. Analyses were conducted in Stata/MP 15.1 (College Station, Texas, USA).
Results
Study population
In this cohort, there were 169 181 patients with cirrhosis, 210 191 patients with HCV without cirrhosis, 766 840 with CHF and 1 438 798 with COPD. The median age of the overall cohort was 59 years (IQR: 50–70) with 50.7% being females. Both cirrhosis and HCV without cirrhosis were more prevalent in patients 40–59 years of age (table 1) whereas CHF and COPD occurred more often in older patients. Males were more likely to have HCV without cirrhosis than females, while COPD was more common in females.
Demographic characteristics of the patients
Opioid prescription
The prevalence of opioid prescription among patients with cirrhosis was 37.1 per 100 person-years and was significantly greater than in HCV without cirrhosis, CHF and COPD (table 2). The prevalence was 43% greater than in CHF [rate ratio (RR)=1.43, 95% CI 1.42 to 1.44] and 53% greater than in COPD (RR=1.53, 95% CI 1.52 to 1.54). Median daily OMEs among those with cirrhosis was 40 (IQR: 24–90), and for HCV without cirrhosis was 40 (IQR: 25–90). Among patients with cirrhosis, 29.1% (n=31 861) had high dose opioid prescriptions (>90 daily OME) during the study period compared with 14.4% (n=30 307) of patients with HCV without cirrhosis (p<0.001). Results were similar when analysis was restricted to individuals age 65 or younger in order to address the possibility of difficultly capturing opioid prescriptions in this dataset in patients with dual Medicare eligibility (online supplementary file 1). In terms of type of opioid prescribed, only a very small proportion consisted of buprenorphine (0.08%, 0.66%, 0.03%–0.05%) or methadone (0.49%, 0.81%, 0.25% and 0.33%) among patients with cirrhosis, HCV, CHF and COPD, respectively.
Prevalence of opioid and benzodiazepine prescription by chronic disease
Benzodiazepine prescription
The prevalence of benzodiazepine prescription among patients with cirrhosis was 21.3 per 100 person-years (table 2). This was significantly greater than benzodiazepine prescription in patients with HCV without cirrhosis (RR=1.73, 95% CI 1.71 to 1.75), CHF (RR=1.76; 95% CI 1.74 to 1.77) or COPD (RR=1.65; 95% CI 1.64 to 1.67).
Dual opioid and benzodiazepine prescription
The prevalence of dual benzodiazepine and opioid prescription was also greater in patients with cirrhosis compared with the other patient groups (p<0.001). Among those with cirrhosis, dual prescription was 17.5% compared with 9.6%, 9.7% and 10.5% among HCV without cirrhosis, CHF and COPD, respectively (table 2). This represents an 81% greater rate than in HCV without cirrhosis (RR=1.81; 95% CI 1.79 to 1.84) and in CHF (RR=1.81; 95% CI 1.79 to 1.82) and a 66% greater prescription than in COPD (RR=1.66; 95% CI 1.65 to 1.68).
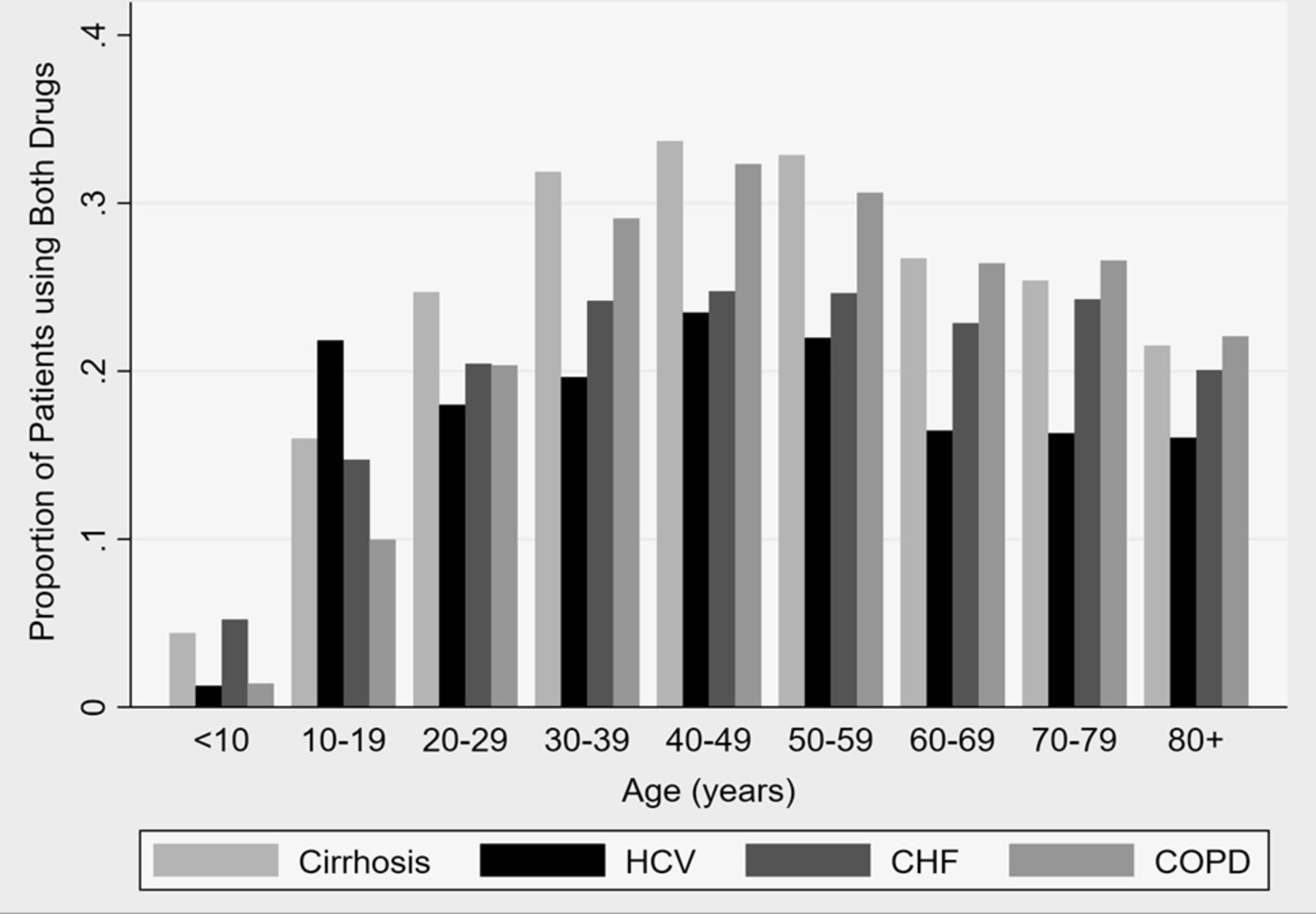
The proportion of patients receiving both benzodiazepines and opioids over the study period 2009–2015 is illustrated by age categories in figure 1. Combined drug prescription was greater in ages 30–59 for those with cirrhosis. Dual drug prescription was quite high in those with HCV without cirrhosis for patients who were 10–19 years of age. For patients with CHF, combined drug prescription was somewhat uniform across ages 30–79. For patients with COPD, combined drug prescription peaked in ages 30–59 years and disproportionately affected older adults.

{kind=link}
Proportion of patients using both opioids and benzodiazepines, years 2009–2015, by age and type of disease. CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HCV, hepatitis C virus.
Drug prescription by type of cirrhosis
Opioid prescription was rather uniform across all subtypes of cirrhosis, from prevalence rates of 35.5 to 38.0 person-years (table 3). Benzodiazepine prescription was greatest in those alcohol contributing to their liver disease compared with those without alcohol abuse. Similarly, rates of dual opioid and benzodiazepine prescription were highest among those with alcohol as a contributing cause of their cirrhosis.
Prevalence of opioid and benzodiazepine prescription by type of cirrhosis
Correlates of high dose prescription opioid prescription
Correlates of opioid prescription among those with liver disease are shown in table 4. High dose opioid prescription was more common in adults ages 40–59 years (for both cirrhosis and HCV without cirrhosis) than at other ages. High dose opioid prescription was 26% greater in men than women for patients with cirrhosis, and 30% greater for those with hepatitis C without cirrhosis. High dose opioid prescription was greater in the western USA for both cirrhosis and hepatitis C without cirrhosis. Having a diagnosis of substance abuse or mental health condition was associated with a 62% greater prevalence of high dose opioid prescription in those with hepatitis C without cirrhosis. For those with cirrhosis, it was associated with a 29% greater prevalence. Individuals with two or more comorbidities were more likely to prescription high dose opioids than those with 0–1 comorbidities. For those with cirrhosis, the subtypes most associated with high dose opioid prescription were alcoholic cirrhosis with HCV and non-alcoholic cirrhosis with HCV.
Correlates of the number of high dose (>90 daily OME) opioid prescriptions
Discussion
In a large, nationally representative database, we demonstrated that despite a propensity for adverse drug-related side effects, individuals with cirrhosis had the highest rates of opioid, benzodiazepine and dual opioid and benzodiazepine prescription. Individuals with cirrhosis are being frequently prescribed opioids, and a significant proportion of individuals with cirrhosis are being prescribed opioids at very high doses (≥90 OMEs). Among individuals with cirrhosis, those with alcoholic liver disease appeared to have the highest rates of benzodiazepine and dual opioid/benzodiazepine prescription, and those with HCV were most likely to have high dose opioid prescription. Overall, patterns of opioid and benzodiazepine prescription appeared to be correlated with demographic factors and comorbid conditions, with variable rates based on age, sex, geographic region and the presences of mental health conditions and other substance abuse history.
Highest rates of opioid, benzodiazepine and dual prescription in cirrhosis
In this study, we have added to the existing literature by confirming in a large, nationally representative database the very high rates of prescription opioid and benzodiazepine use in cirrhosis, occurring in one-third and one-fifth of patients, respectively. Importantly, in this study, we have been able to place these rates and patterns of prescription in context relative other comparator chronic diseases that have similarly high overall healthcare utilisation.17 The reasons for this discrepant patterns of prescription in cirrhosis remain largely unknown and represent an important area for future investigation. Chronic pain is a common symptom across these disease states and thus variable rates of prescription would not be anticipated to reflect the burden of symptomology.18–20 In clinical practice, there remains prevalent misconceptions regarding safety of acetaminophen among individuals with chronic liver disease, and this may in part drive higher use of alternative forms of analgesics, but this has not been definitively shown in prior studies.21 22 Additionally, this factor alone is unlikely to explain this degree of discrepancy in rates of prescriptions and thus dedicated evaluation of patient and provider perceptions and other factors influencing pain management in cirrhosis is needed. Relatedly, another important finding of note was the rates of high dose (≥90 OMEs) opioid prescription among patients with cirrhosis, which occurred in 29% of individuals with cirrhosis. Prevalence of high dose opioid prescription was higher in this cohort compared with a large recent VA cohort where>100 OME occurred in 21% of patients, though the overall prevalence of opioid prescription was much higher in that VA population (77%).13 Given that it is well established that risk of adverse drug effects parallels OMEs, further understanding of these prescribing patterns is urgently warranted.23
Variable patterns of prescription by demographics and comorbidities
Another key finding of our study is the identification of correlates of opioid and benzodiazepine prescription among individuals with chronic disease. Middle-aged individuals had significantly higher rates of high dose opioid prescription as well as dual opioid-benzodiazepine prescription. Men were also noted to have much higher rates of opioid prescription. This variation in terms of age and sex has been inconsistently shown in prior studies.24 25 Differences in risk profiles according to these demographic features may be explained by subgroups of patients evaluated. Of note, in this study, we also found significant differences in rates of prescription according to geographic region, with highest rates of opioid prescription among individuals in the western USA. Geographic variations in opioid prescribing in the USA has been noted prior, particularly as it relates to disproportionate prescription in southern and western states, with the reasons for this variation remaining unclear.1 26
As expected, among individuals with cirrhosis and HCV without cirrhosis, those with a higher overall disease burden as indicated by a higher Charlson Comorbidity Index had a RR of 1.25 for high dose opioid prescription. Presence of a mental health or other substance abuse condition was particularly high risk (RR 1.29) in terms of likelihood of high dose opioid prescription. This higher rate of opioid prescription among individuals with other mental health conditions has been well described in the general population, with prior retrospective and cross-sectional studies highlighting the disproportionate prescription of opioids among patients with mood and anxiety disorders.27 28
Patterns of prescription by aetiology of liver disease
A finding of particular interest was the variations in opioid and benzodiazepine prescription by aetiology of cirrhosis. Rates of opioid prescription were generally similar across different aetiologies of cirrhosis, but high dose opioid prescription was more common among patients with HCV as a cause of their cirrhosis. Interestingly, benzodiazepine prescription was markedly different across aetiologies of cirrhosis, with individuals with alcohol contributing to their cirrhosis having the highest rates of benzodiazepine and dual opioid and benzodiazepine prescription (22%–25% vs 19% and 19% vs 16%, respectively). This type of examination of rates of opioid and benzodiazepine prescription by type of liver disease has not been previously described. It has been hypothesised based on observations in clinical practice that individuals with prior alcohol use disorders increase uptake of benzodiazepines, in part due to counselling about need for alcohol cessation.29 This change in use of substances is particularly relevant among individuals with liver disease whose access to liver transplantation is restricted based on alcohol use and thus may drive increased use of alternative agents with neuropsychiatric effect, though this concept has not been the subject of dedicated investigation.
Contextual factors and limitations of this study
There are several limitations to note related to this study. The primary limitation stems from the use of a secondary database which relies on diagnosis codes for categorisation of chronic disease. There is inherent potential for misclassification with both undercoding and overcoding. Marketscan has been analysed extensively for the purpose of clinical research and diagnosis codes for these common conditions have been applied in multiple studies for evaluation of outcomes in chronic disease. Another point to highlight includes the lack of evaluation of inpatient or emergency room prescriptions and potential inciting events (such as surgeries or other acute inciters including delirium tremens) and their impact on overall prevalence of use. Similarly, given the nature of this dataset, we were only able to investigate a limited set of variables as correlates of opioid and benzodiazepine prescription.
Clinical and health policy implications and conclusion
In conclusion, we demonstrated high rates of prescription opioid, benzodiazepine and dual opioid and benzodiazepines among individuals with chronic disease, with markedly higher rates of prescription among individuals with cirrhosis. Rates of prescriptions are high in cirrhosis, and dosages among patients with cirrhosis are also markedly higher, further compounding potential for adverse clinical outcomes in this high risk patient population. Rates of prescription varied by age, sex geographic region and aetiology of liver disease highlighting important variations in prescribing patterns that may be amenable to targeted interventions.
References
Footnotes
Contributors MAK: study design and drafting of manuscript. MR: statistical analysis. BK: statistical analysis and revision of manuscript. AGS: study design, revision of manuscript. ET: revision of manuscript. PS: revision of manuscript. SS: revision of manuscript. BN: study design and revision of manuscript. AW: study design and revision of manuscript.
Funding AW’s research is funded by a VA HSR&D CDA-2 Career Development Award (1IK2HX000775). AW and BN also receive support from Michigan Institute for Data Science (MIDAS) at the University of Michigan. AGS’s research is funded by RO1MD12565 and R01 CA12008.
Disclaimer These funding sources did not have any role in the design, conduct, collection, management, analysis, interpretation, preparation, review or approval of the manuscript. This content is solely the responsibility of the authors and does not necessarily represent the official views of the healthcare centres, the NIH or the VA.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party (Truven Marketscan) and are not publicly available. Data are deidentified.