Article Text

Abstract
Background and aims There is a need to safely achieve conscious sedation during endoscopic retrograde cholangiopancreatography (ERCP). We evaluated the safety and feasibility of a mainstream capnometer system to monitor apnoea during ERCP under CO2 insufflation.
Methods Non-intubated adult patients undergoing ERCP-related procedures with intravenous sedation were enrolled. End-tidal CO2 (EtCO2) was continuously monitored during the procedure under CO2 insufflation using a mainstream capnometer system, comprising a capnometer and a specially designed bite block for upper gastrointestinal endoscopy and ERCP. Oxygen saturation (SpO2) was also monitored continuously during the procedure. In this study, we evaluated the safety and feasibility of the capnometer system.
Results Eleven patients were enrolled. Measurement of EtCO2 concentration was possible from the beginning to the end of the procedure in all 11 cases. There was no measurement failure, dislocation of the bite block, or adverse event related to the bite block. Apnoea linked to hypoxaemia occurred five times (mean duration, 174.4 s).
Conclusion This study confirmed that apnoea was detected earlier than when using a percutaneous oxygen monitor. Measurement of EtCO2 concentration using the newly developed mainstream capnometer system was feasible and safe even under CO2 insufflation.
- end-tidal carbon dioxide (EtCO2)
- endoscopic retrograde cholangiopancreatography (ERCP)
- endoscopic ultrasound (EUS)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- end-tidal carbon dioxide (EtCO2)
- endoscopic retrograde cholangiopancreatography (ERCP)
- endoscopic ultrasound (EUS)
Summary box
What is already known about this subject?
End-tidal capnography during endoscopic retrograde cholangiopancreatography (ERCP) is reported to be useful. However, the detection of EtCO2 during full endoscopic procedures using currently available sidestream-style products has been reported to be difficult because of the blockage of the sampling tube with saliva or secretions, undetectable shallow breathing, or tachypnoea, with sampling errors caused by high oxygen concentration.
What are the new findings?
The newly developed mainstream capnometer system for ERCP under CO2 insufflation is useful and reliable based on this pilot study.
How might it impact on clinical practice in the foreseeable future?
Based on this research, reliable detection of respiratory arrest during ERCP treatment under sedation is expected to be possible. This has an impact on patient management during endoscopic treatment.
Introduction
Given the continued increase in the complexity of interventional endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound (EUS) for pancreatobiliary disorders, endoscopists encounter a larger number of patients requiring procedural sedation.1 In Japan, conscious sedation during such procedures is mainly managed by endoscopists themselves, rather than by anaesthesiologists. Effective conscious sedation and analgesia during endoscopic procedures provides relief of suffering and frequently leads to a successful and shorter procedure. However, agents for sedation and/or analgesia can result in adverse effects. Therefore, significant attention has been paid to safely achieve conscious sedation during ERCP.
Hypoxaemia is the most frequent adverse effect of conscious sedation during endoscopic procedures.2 Causes of hypoxaemia are considered to be apnoea caused by respiratory depression or comorbid respiratory dysfunction, such as chronic obstructive pulmonary disease. Hypoxaemia can lead to unexpected cardiac arrest and/or brain injury. It has been reported that hypoxaemia follows apnoea during sedation, and as such, early detection of apnoea may decrease hypoxaemia.3
End-tidal capnography is a non-invasive method to detect depressed respiratory activity by optimal assessment of CO2 throughout the respiratory cycle. End-tidal capnometry has been reported to be useful in the intensive care unit.4 However, its reliability and safety during endoscopic procedures have not been confirmed because of insufficient evidence.5–10 Detection of end-tidal CO2 (EtCO2) during full endoscopic procedures using currently available sidestream-style products has been reported to be difficult owing to blockage of the sampling tube with saliva or secretions, undetectable shallow breathing, or tachypnoea, with sampling errors caused by high oxygen concentration.11 New endoscope-dedicated capnometer systems are expected to improve these weaknesses.
Recently, a mainstream capnometer system for patients undergoing upper endoscopy and requiring oxygen was developed with the technological innovation of CO2 detector miniaturisation.12 13 A sidestream capnometer transports a portion of the patient’s respired gases from the sampling site, through a long sampling tube, to a sensor, whereas a mainstream capnometer does not transport gas away from the sampling site (figure 1). The CO2 concentration is measured directly by a sensor on the nose, and its usefulness has been reported.11 Therefore, we applied this mainstream capnometer system to endoscopic procedures. The sensor on the bite block can measure mixed CO2 from the mouth and nose through the airway of the bite block. Because there is neither obstruction by saliva nor time lag, this newly developed mainstream capnometer is expected to measure CO2 more accurately than a conventional sidestream capnometer. In this pilot study, we examined the safety and feasibility of this new capnometer system in the clinical setting.
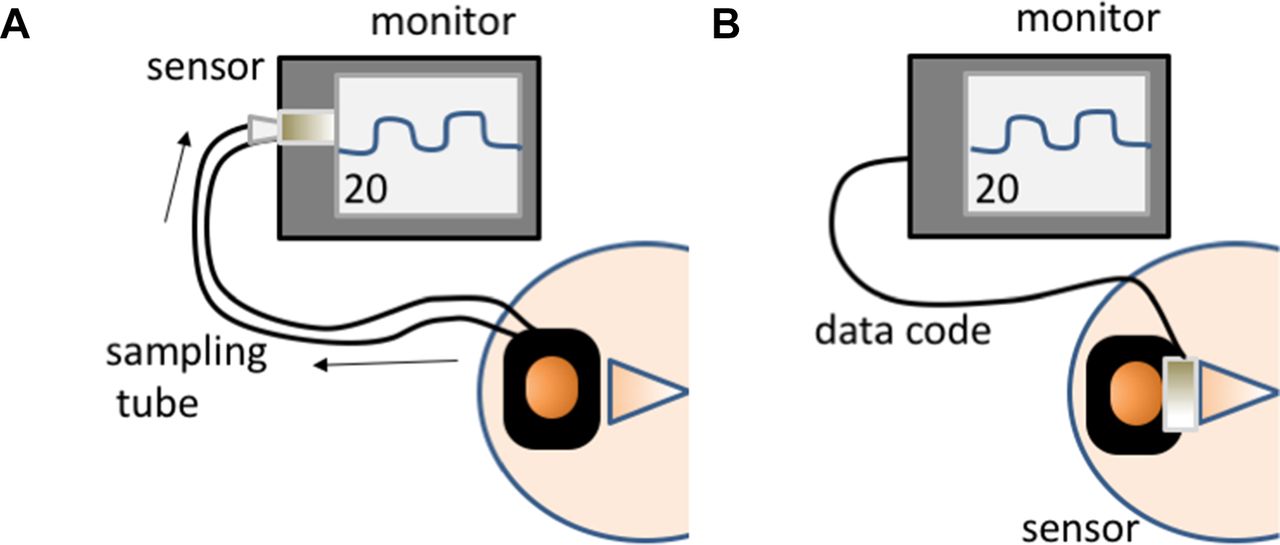
Schema of sidestream and mainstream capnography. (A) Sidestream capnography. Sidestream gas analysis uses a long plastic sampling tube connected to an adapter on the bite block. (B) Mainstream capnography. The CO2 detector is located on the bite block without gas transportation away from the sampling site.
Patients and methods
Patients and procedure
Patients undergoing ERCP-related procedures at our university hospital were enrolled with written informed consent. Endoscopic procedures under room air and CO2 insufflation were performed in the general endoscopy room without anaesthesiologists. All patients were administered flunitrazepam 0.2 mg and pethidine 35 mg intravenously under EtCO2, oxygen saturation (SpO2), electrocardiographic, and blood pressure monitoring. Investigators checked the monitors throughout the procedure and intervened with body shaking and O2 supply or antagonist for apnoea or hypoxaemia. Apnoea was defined as 15 s suspension of EtCO2 elevation. Hypoxaemia was defined as a 5% decrease before the procedure. Events within 3 min of each other were defined as a single event. The study was registered in UMIN (UMIN000029407), and the first patient was enrolled on 7 December 2016.
Newly developed capnometer
The cap-ONE bite block (YG-227T; Nihon Kohden, Tokyo, Japan) can deliver oxygen while measuring mainstream EtCO2 during endoscopic procedures (figure 2). It comprises the mainstream capnometer cap-ONE (TG-980P; Nihon Kohden), nasal adapter, oxygen cup, and mouthpiece. The nasal adapter collects exhaled nasal flow into a measurement cell, while the oxygen cup delivers oxygen through the patient’s nose and has a sponge to scatter oxygen for accurate CO2 monitoring. The mouthpiece has a double-layer conduit to open the patient’s mouth as well as to collect oral exhaled CO2. It also has an oxygen port, which can supply oxygen through the mouth.

Structure and airflow dynamics of the cap-ONE bite block (TG-980P; Nihon Kohden,Tokyo, Japan). (A) Structure of the cap-ONE bite block. The cap-ONE bite block system comprises the mainstream capnometer, nasal adapter, mouthpiece, and oxygen cup. (B) Flow of O2 and CO2 through the cap-ONE bite block. The cap-ONE bite block system is attached on the patient's face as shown.
Results
Eleven patients were enrolled. Patient characteristics are shown in table 1.
Patient characteristics
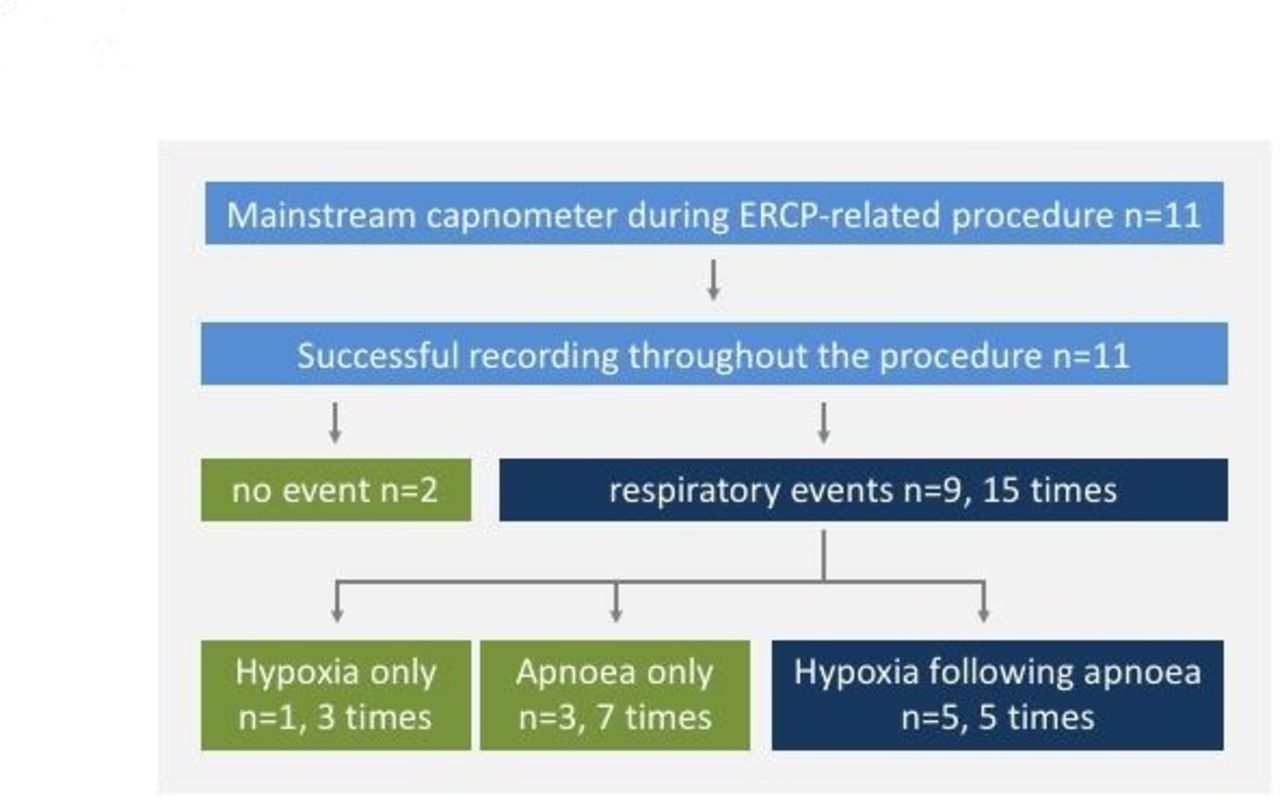
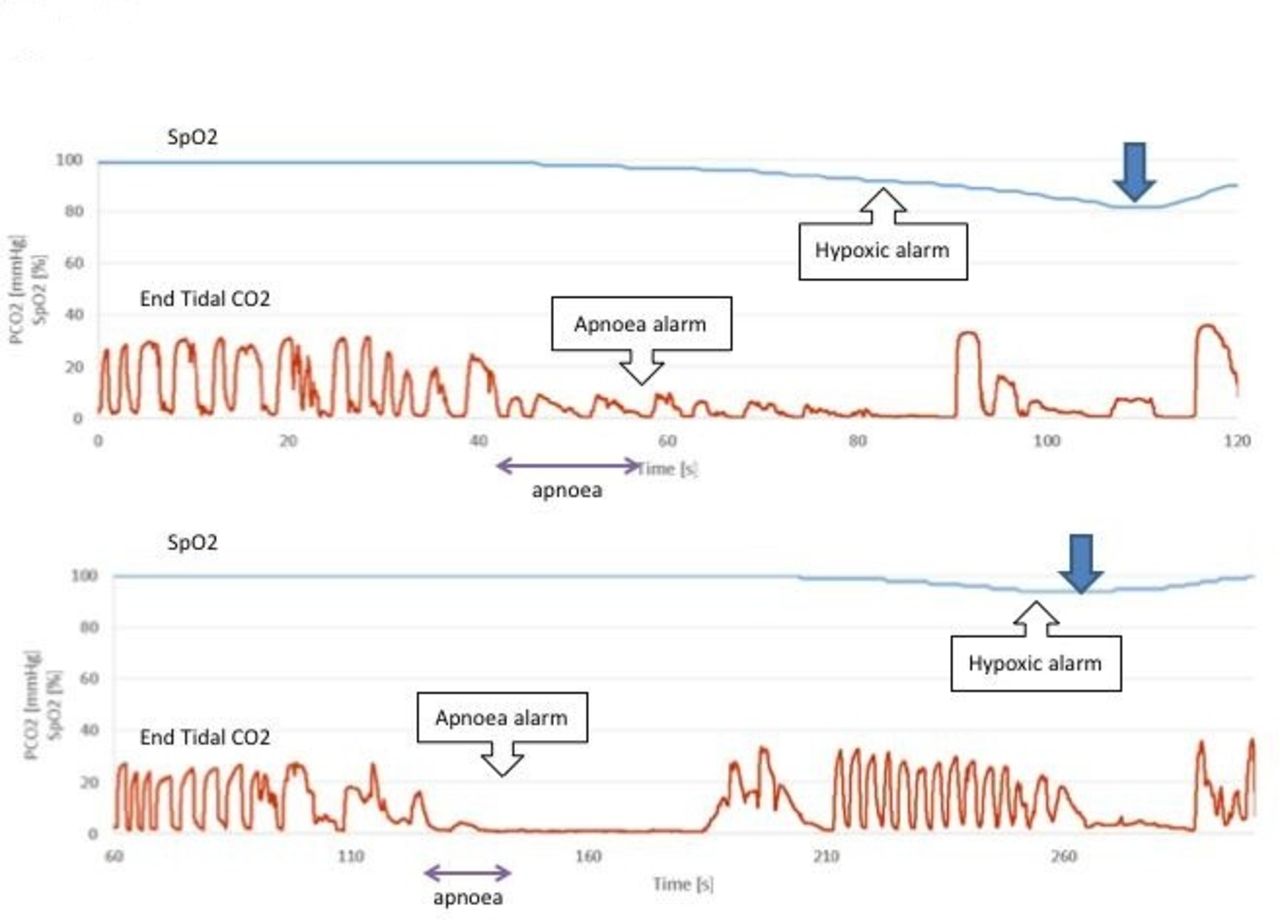
Measurement of CO2 concentration was possible from the beginning to the end of the procedure in all 11 cases, even though temporary spikes in CO2 were observed at the time of inserting and extracting the endoscope and belching (figure 3). There was no detection failure of the CO2 wave. There were no harmful capnometer-related complications, such as discomfort when wearing. Apnoea occurred seven times in seven patients, and hypoxaemia was linked to apnoea five times in five patients (figure 4). Mean delay from apnoea to hypoxaemia was 174.4±104.3 s. Hypoxaemia requiring intervention occurred five times in four patients. Hypoxaemia requiring intervention linked to apnoea occurred two times in two patients. Figure 5 shows a reduced view of the capnometer waveform in these two patients. Hypoxaemia without preceding apnoea occurred three times in two patients (table 2).
Data on apnoea and hypoxaemia events

Waveforms of the capnometer. This figure shows the waveforms of oxygen saturation (SpO2) and end-tidal CO2 (EtCO2). A transient increase in EtCO2 is seen when the endoscope is inserted, but it promptly returns to the normal level.

Patient flow chart of mainstream capnometer during endoscopic retrograde cholangiopancreatography (ERCP).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Waveform of hypoxaemia linked to apnoea. These are representative data of apnoea preceding hypoxaemia.
Discussion
This study is the first pilot study on the feasibility and safety of a novel mainstream capnometer system during interventional endoscopy. This study showed that it was possible to measure EtCO2 throughout the endoscopic procedure and accurately detect apnoea using this capnometer. There were also no harmful complications related to the capnometer.
Conventional percutaneous CO2 monitors are not so effective during endoscopic procedures because of their low measurement accuracy and measurement failure; further, their set-up is labour intensive and they require a prolonged stabilisation time .14 Capnometer is considered to have a higher measurement accuracy than percutaneous CO2 monitors because it directly reflects changes in respiration.
Disadvantages of the currently used sidestream capnometer include delayed response due to the length of the sampling tube, obstruction by water or saliva, and measurement inaccuracies due to large oxygen flow.15 16 On the other hand, the newly developed mainstream capnometer system can measure exhaled CO2 directly around the mouth and nose without a delayed response and can prevent tube obstruction by water or saliva. Therefore, the mainstream capnometer is expected to be reliable with more accurate data, especially during ERCP, which is often performed in patients with shallow breathing and a lot of saliva. Fortunately, in this study, we successfully measured EtCO2 during the procedure under CO2 insufflation without detection failure. Conventionally, there was concern about discomfort wearing the mainstream capnometer because of its large size, but the cap-ONE is small enough to fit into the bite block.
Integrating capnography into patient-monitoring protocols for endoscopic procedures with moderate sedation, which typically consist of a benzodiazepine and narcotic analgesic, has not been shown to improve patient safety. However, there is evidence supporting its use in procedures targeting deep sedation. Also, use of a capnometer for EUS and ERCP has not been recognised as a standard method for monitoring in the American Society for Gastrointestinal Endoscopy guideline.1 In one trial comparing capnometer versus oximetry monitoring in patients undergoing EUS or ERCP, the frequency of hypoxaemia was significantly reduced in patients with capnography.7 However, there is another trial with contradictory results. In the latter study, per-protocol analysis excluding cases of mismeasurement due to capnometer problems revealed that the frequency of hypoxaemia was significantly reduced.8 The reliability of the mainstream capnometer is expected to be generalised based on more evidence.
Therefore, it is assumed that capnometry may reduce the incidence of hypoxaemia when applied correctly. There are some risk factors for hypoxaemia during endoscopy, which have been pointed out in previous studies, such as age, high body mass index, history of sleep apnoea, and increased doses of sedatives.9 Apnoea is also an independent risk factor for hypoxaemia, and a capnometer may reduce hypoxaemia due to apnoea. In our study, apnoea preceding hypoxaemia was detected in 5 of 11 cases, and it seems that intervention, such as physical stimulation or increased O2 inhalation, may prevent the subsequent decrease in SpO2.
The limitation of this research is that it included only a small number of cases. Thus, there is a possibility that cases of measurement failure may occur as the number of cases increases. In addition, because sedation depth during ERCP differs depending on the country and facility, our study reflects data under specific conditions. However, apnoea preceding hypoxaemia definitely exists. If we can properly apply the capnometer and receive accurate data, the use of a capnometer during ERCP procedures is useful for reducing hypoxaemia by detecting apnoea earlier.
Based on the result of this pilot study, a randomised controlled trial comparing capnometer monitoring and standard monitoring is currently in progress.
Conclusion
It is suggested that during ERCP, the mainstream method using our novel capnometer may be more accurate and useful than the sidestream method. Although this was a study of only a few cases, it suggests that a mainstream capnometer is useful for early detection of hypoxaemia by apnoea detection and its prevention. We would like to evaluate its usefulness in randomised trials of numerous cases in the future.
References
Footnotes
Contributors All authors had access to the data. EI, YT, and TM participated in the design of the study. YT performed statistical analysis and wrote the first draft of the manuscript. IE, TM, HO, and TK edited the draft. YT, EI, SF, SK, TS, TK, KM, YM, and HT performed endoscopy and participated in patient care. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TM received research grant from Nihon Kohden, Tokyo, Japan.
Patient consent Obtained.
Ethics approval Approval was obtained from the Ethics Committee of Keio University Hospital(8 August 2016; No 20160155, UMIN000024867).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.