Article Text

Abstract
Background The Chicago Classification (CC) defines oesophagogastric junction outflow obstruction (EGJOO) as the presence of an elevated integrated residual pressure (IRP) together with preserved oesophageal body peristalsis but its clinical significance is evolving.
Aims To describe the clinical and manometric characteristics in patients with EGJOO and propose a new classification.
Methods In this retrospective cohort study, patients with functional oesophageal symptoms underwent clinical and endoscopic assessment and oesophageal high-resolution manometry (HRM). The CC V.3 was used to define and redefine abnormalities.
Results Of 478 HRM studies performed, EGJOO, defined as median IRP >15 mm Hg, was diagnosed in 116 patients; 17 underwent a follow-up HRM. Forty-four patients had otherwise normal oesophageal motility, with the only finding being EGJOO; 14 had achalasia, 19 had EGJOO plus ineffective oesophageal motility (IEM), 28 had EGJOO plus diffuse oesophageal spasm (DES) (n=25) or jackhammer oesophagus (n=3), and 11 had EGJOO plus IEM and DES. Patients with EGJOO+IEM had lower distal contractile integral (DCI) while those with EGJOO+DES had higher DCI. All groups exhibited high percentages of incomplete bolus clearance. On repeat studies, EGJOO preceded or followed another HRM diagnosis and remained permanent in 2/17 patients. Only one patient transitioned to achalasia.
Conclusions The new classification further defines EGJOO by considering abnormalities in the body of the oesophagus that could contribute to symptoms or require therapy. Most patients with EGJOO have a coexisting motility disorder and do not have isolated EGJOO. There is a fluidity of the HRM diagnosis that needs to be considered prior to therapy.
- oesophageal disorders
- oesophageal motility
- dysphagia
- manometry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The wider use of oesophageal high-resolution manometry (HRM) increasingly recognises oesophagogastric junction outflow obstruction (EGJOO) but the clinical significance of this condition and its relationship to other oesophageal motility abnormalities is evolving.
What are the new findings?
This retrospective cohort study of patients with dysphagia, regurgitation and EGJOO, concomitant motility abnormalities, such as ineffective oesophageal motility (IEM), diffuse oesophageal spasm (DES) and achalasia were recognised, contributing to incomplete bolus clearance.
EGJOO preceded or followed another manometric diagnosis and remained permanent only in few patients.
How might it impact on clinical practice in the foreseeable future?
A proposed new scheme of HRM starts with the recognition of EGJOO, then proceeds to assess the oesophageal body contractility as normal or abnormal, such as achalasia, IEM, DES (including jackhammer oesophagus) or combined IEM+DES. This way, several subtypes of EGJOO, each potentially with their own therapeutic implications, are recognised.
Introduction
The widespread clinical use of high-resolution oesophageal pressure topography (HREPT) and the recent introduction (version 3) of the Chicago Classification (CC V.3) have led to our increasing refinement of several manometric patterns and new diagnostic classifications, but their clinical significance and implications are still uncertain.1 Oesophagogastric junction outflow obstruction (EGJOO) is one such pattern that is characterised by preserved peristalsis in conjunction with an elevated integrated residual pressure (IRP).2 EGJOO may result from specific anatomic or functional variants or may be a prestage of classic achalasia.3 Symptoms in patients with EGJOO do not always require treatment and treatment response varies. A key challenge in management is deciding which patients will need intervention.4
In clinical practice, it is not uncommon to encounter patients with EGJOO and symptoms suggestive of oesophageal emptying delay, such as acid regurgitation and dysphagia, who—in addition to EGJOO—fulfil other CC criteria, such as diffuse oesophageal spasm (DES), jackhammer oesophagus (JE), ineffective oesophageal motility (IEM) or achalasia. Under these clinical circumstances, it becomes unclear which element of the abnormal manometric diagnosis is contributing to the patients’ symptoms (the EGJOO, the distal spasm or the ineffective peristalsis) and it becomes difficult to decide about therapy (relief of EGJOO, botulinum toxin injection or prokinetic therapy).
The aim of this study is to describe the clinical and manometric characteristics in our cohort of patients with EGJOO with and without other coexisting CC diagnoses. We hypothesised that patients with EGJOO may have concomitant oesophageal dysmotility, possibly contributing—at least in part—to their oesophageal symptoms, and that a new subclassification—a modification of the CC—would be more useful clinically.
Patients and methods
Patients
This retrospective cohort study was approved by the Institutional Research Board of El Camino Hospital and was conducted at the Neurogastroenterology and Motility Center of Silicon Valley Gastroenterology, in Mountain View, CA. The study was considered exempt from the need for individual informed consent from participating patients. We included all patients who underwent routine high-resolution manometry (HRM) at the Silicon Valley Neurogastroenterology and Motility Center and were diagnosed with EGJOO between January 2014 and June 2017. Eligible patients were recruited through a review of all our HRM records during the study period. Using the classic definition offered by the CC V.31 and for the purposes of this study, EGJOO was defined as incomplete EGJ relaxation. The incomplete EGJ relaxation was measured by a median IRP of 15 mm Hg or higher. All electronic patient records were reviewed in detail for medical history, standardised symptoms questionnaires and endoscopic or other clinical records. Based on these findings, patients were divided into patients with primary (idiopathic) EGJOO and those with secondary outflow obstruction, resulting from a mechanical aetiology. Because of clinical uncertainties, some patients in the cohort had repeat HRM studies performed and their data over time were also examined.
Inclusion criteria
On presentation, all patients were symptomatic with oesophageal and upper abdominal complaints that were recorded on questioning and formal questionnaire-based assessment. To meet entry criteria, patients had to have one or more oesophageal and upper abdominal symptoms (such as epigastric pain, acid regurgitation, postprandial bloating, nausea, vomiting, belching, dysphagia and/or weight loss) of at least a 2 months’ duration, and no evidence of mechanical obstruction by endoscopy and retroflexion at the cardia. Further, they had to have undergone an oesophageal HRM revealing EGJOO. A detailed history and physical examination was conducted to exclude any other plausible explanation for the patients’ symptoms and additional tests (eg, biopsies, oesophageal ambulatory pH monitoring, biliary imaging, contrast studies) were ordered as indicated for diagnosis (see study flow in figure 1 and table 1). Endoscopic ultrasound (EUS) was not used in any of the cases; barium contrast radiography was performed selectively in only three cases.
Exclusion criteria
Patients <16 years old, those with known obstructive oesophageal or gastric disease by endoscopy. On presentation and during evaluation, none of the patients were receiving medication affecting oesophageal motility. Of note, the study, although community based, was on a referral population to a gastroenterology practice with emphasis on motility disorders.

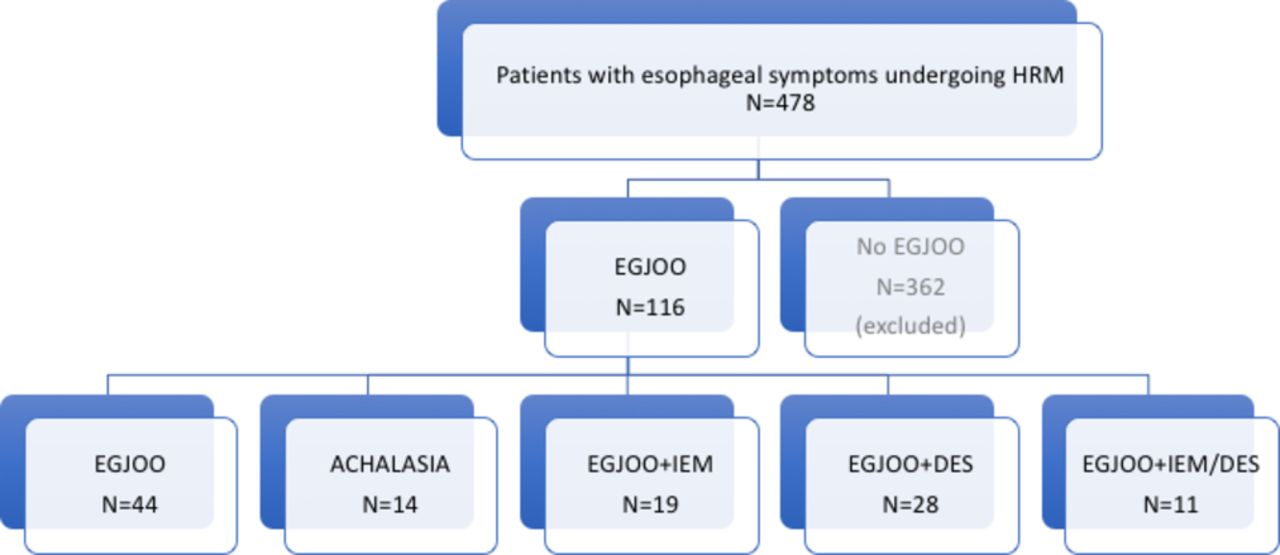
Study diagram. Of 478 oesophageal HRM studies, EGJOO was diagnosed in 116 patients; the remaining 362 patients were excluded from analysis. Forty-four of these patients had otherwise normal oesophageal motility, with the only HRM finding being EGJOO; 14 had Chicago Classification (CC) citeria for achalasia, 19 had EGJOO plus CC criteria for IEM, 28 had EGJOO plus DES, and 11 had EGJOO plus IEM and DES. DES, diffuse oesophageal spasm; EGJOO, oesophagogastric junction outflow obstruction; HRM, high-resolution manometry; IEM, ineffective oesophageal motility.
Patient characteristics
Questionnaires
To qualify for inclusion into the study, patients had to be symptomatic on a simple and previously extensively used general questionnaire. In this questionnaire, the symptoms were graded with scores for epigastric pain, regurgitation, postprandial bloating, nausea, vomiting, dysphagia, belching and weight loss (0=no symptom, 1=mild symptom, 2=moderate symptom and 3=severe symptom, occurring at various frequencies (once a week=0; 2–6 times a week=1; 7–15 times a week=2; and more than 15 times a week=3)).5
Endoscopy and biopsies
Upper endoscopy with random proximal and distal oesophageal biopsies was performed as part of the structural assessment of the cohort. Patients were classified as normal, erosive esophagitis, eosinophilic esophagitis or Barrett’s oesophagus. Hiatal hernia (sliding, paraoesophageal or mixed) was defined endoscopically and confirmed by HRM and graded in centimetre length. Esophagitis was also independently assessed histologically using standard criteria.6
Oesophageal HRM
A solid-state HRM catheter with 4.2 mm outer diameter with 36 circumferential sensors located at 1 cm intervals was used for the study (Medtronic, Sunnyvale, CA). Manometric studies were performed with patients after at least a 6-hour fast. The HRM catheter was placed transnasally and positioned to record from the hypopharynx to the stomach. The manometric protocol included baseline recording and ten 5 mL water/saline swallows. The HREPT of each swallow was analysed for integrity of the 20 mm Hg incomplete bolus clearance (IBC). The length of the break within 20 mm Hg IBC was measured using the smart mouse tool in ManoView Software (Medtronic). Oesophageal peristalsis was defined as intact if no break longer than 5 cm was observed within the IBC. Individual swallows were excluded from analysis in case of double or multiple swallows that could lead to deglutitive inhibition of peristalsis. Oesophageal HRM measurements were analysed using ManoView Analysis software as previously described.7 First, the basal lower oesophageal sphincter pressure (LESP) during the baseline recording was automatically calculated, followed by the 10 swallows that were evaluated separately, with manual correction of the contractile deceleration point marker and the slope of the contractile front velocity, if necessary. Distal latency, distal contractile integral (DCI), average intrabolus pressure, maximum intrabolus pressure and IRP were automatically calculated. Preserved peristalsis was defined as some instances of intact peristalsis, or weak peristalsis with small breaks.
Elements of the CC V.3 were used to define the following manometric diagnsoses1: type I (classic achalasia): elevated median IRP (>15 mm Hg) with 100% failed peristalsis (DCI <100 mmHgscm); type II achalasia (with oesophageal compression): elevated median IRP (>15 mm Hg), 100% failed peristalsis, panoesophageal pressurisation with ≥20% of swallows; type III (spastic) achalasia: elevated median IRP (>15 mm Hg), no normal peristalsis, premature (spastic) contractions with DCI >450 mmHgscm with ≥20% of swallows, at times mixed with panoesophageal pressurisation; EGJOO: elevated median IRP (>15 mm Hg) with sufficient evidence of peristalsis; DES: ≥20% premature contractions with DCI >450 mmHgscm with intermittent normal peristalsis; hypercontractile JE: at least two swallows with DCI >8000 mmHgscm; IEM: ≥50% ineffective swallows. Ineffective swallows could be failed or weak (DCI <450 mmHgscm). For the purposes of this analysis, all three achalasia types were grouped together. EGJOO+DES included cases with combined EGJOO with DES or JE; EGJOO+IEM included cases with combined EGJOO with IEM; and EGJOO+IEM+DES included cases combining criteria for EGJOO with IEM and DES (no cases of JE were found in this group).
Statistics
Statistical analysis was performed using commercial statistical software (Minitab Express). The two-tailed t-test was used to compare continuous variables. For all statistical analyses, the level of significance was set at p<0.05. Results are depicted as tables, bar graphs and box plots, as needed.
Results
A total of 478 oesophageal HRM studies were performed in our outpatient, community-based unit in the 3.5 years of study. EGJOO was diagnosed in 116 patients (24%); the remaining 362 patients were excluded from analysis. Forty-four of these patients had otherwise normal oesophageal motility, with the only HRM finding being EGJOO; 14 had CC criteria for achalasia, 19 had EGJOO plus CC criteria for IEM, 28 had EGJOO plus DES (n=25) or JE (n=3), and 11 had EGJOO plus IEM and DES (figure 1). Of note, 58 patients (50%) had double classification using the CC V.3, that is, EGJOO plus another HRM diagnosis, and only 38% of patients had pure EGJOO and 12% had achalasia (which includes EGJOO in its definition).
Table 1 describes the patients’ characteristics of the five subcohorts. There were no differences in age, gender or body mass index among the groups. The percentage of patients with sliding hiatal hernia (measured by HRM) was variable, ranging from 0% to 29%. The mean hernia length, measured manometrically, was 0.2 cm (range 0–3.5). Although an underlying endoscopic aetiology of the outflow obstruction could not be ascertained, table 1 also describes the number of ‘secondary’ EGJOO in each group, such as eosinophilic oesophagitis (EoE) (n=3), gastro-oesophageal reflux disease (GERD) validated by ambulatory pH monitoring (n=28), achalasia8 9 paraoesophageal herniation (n=4), postfundoplication (n=8), Parkinson’s disease (n=28) and gastroparesis (GP) (n=4). Since narcotic use is a known factor underlying EGJOO, we carefully examined all patients and none was found. Patients without underlying putative aetiology were considered having ‘primary’ or ‘idiopathic’ EGJOO and they were variably distributed among the five groups, ranging from 16% to 79%. The duration of follow-up ranged from 2 to 35 months, with a median of 20.5 months (95% median CI, 18 to 24).
Figure 2 displays the symptom prevalence in our five groups in our cohort. Although dysphagia (range 46%–80%) and regurgitation (64%–85%) were the leading symptoms, chest and epigastric pain was also prevalent (27%–64%) and there was no statistical predominance among any of the five groups. Figure 3 depicts the range and severity of symptoms that was similar among the groups but generally mild to moderate (symptom scores 1–2). These data suggest that patients with EGJOO, irrespective of the additional HRM subgrouping, are clinically indistinguishable from each other and—more importantly—from the well-characterised and accepted group of patients with achalasia of any type.
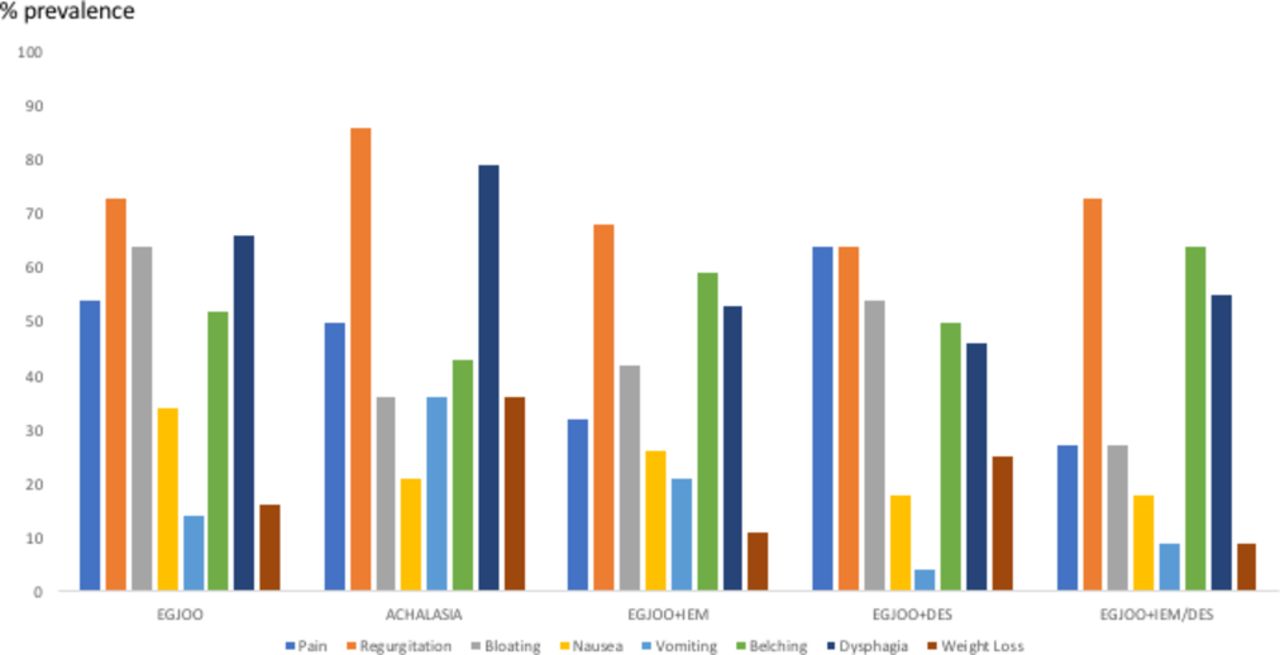
Symptom prevalence in the five groups. Although dysphagia and regurgitation were the leading symptoms, chest and epigastric pain was also prevalent and there was no statistical predominance among any of the five groups. DES, diffuse oesophageal spasm; EGJOO, oesophagogastric junction outflow obstruction; IEM, ineffective oesophageal motility.

Range and severity of symptoms in the five groups. In general, symptoms were mild to moderate (symptom scores 1–2). These data suggest that patients with EGJOO, irrespective of the additional high-resolution manometry (HRM) subgrouping, are clinically indistinguishable from each other. DES, diffuse oesophageal spasm; EGJOO, oesophagogastric junction outflow obstruction; IEM, ineffective oesophageal motility.
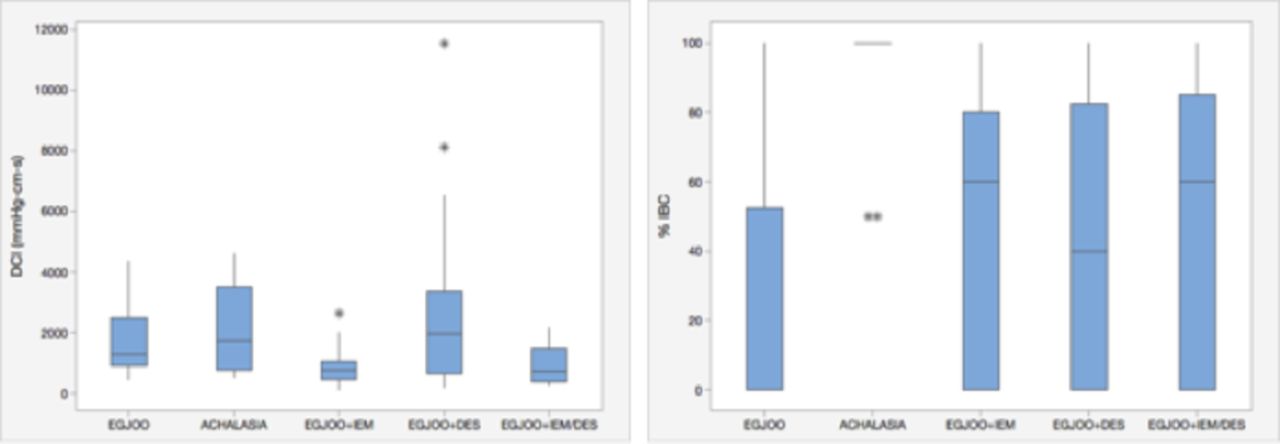
Figure 4 shows box plots of two HRM parameters assessed: the LESP and residual pressure (both in mm Hg); there were no differences among the five groups in our cohort. Figure 5 shows box plots of DCI and % incomplete bolus clearance (IBC). Not surprisingly, patients with EGJOO+IEM had statistically lower DCI while those with EGJOO+DES had higher DCI (p<0.002 between EGJOO+IEM and EGJOO+DES; p<0.001 between EGJOO and EGJOO+IEM). Even the group EGJOO+IEM+DES had statistically lower DCI, when compared with EGJOO+DES (p<0.003). All groups exhibited high percentages of IBC (40%–100%), suggestive of significant oesophageal stasis. This suggests that EGJOO may be the primary process responsible for poor oesophageal clearance, irrespective of associated abnormalities of the oesophageal body peristalsis (normal, ineffective or spastic).

Box plots of two high-resolution manometry (HRM) parameters assessed, the lower oesophageal sphincter pressure (LESP) and the integrated residual pressure (IRP) (both in mm Hg). There were no differences among the five groups. The box plots represent minimum and maximum values (vertical lines), first and third quartiles (boxes) and median values (horizontal line). Asterisks represent outlier values. DES, diffuse oesophageal spasm; EGJOO, oesophagogastric junction outflow obstruction; IEM, ineffective oesophageal motility.
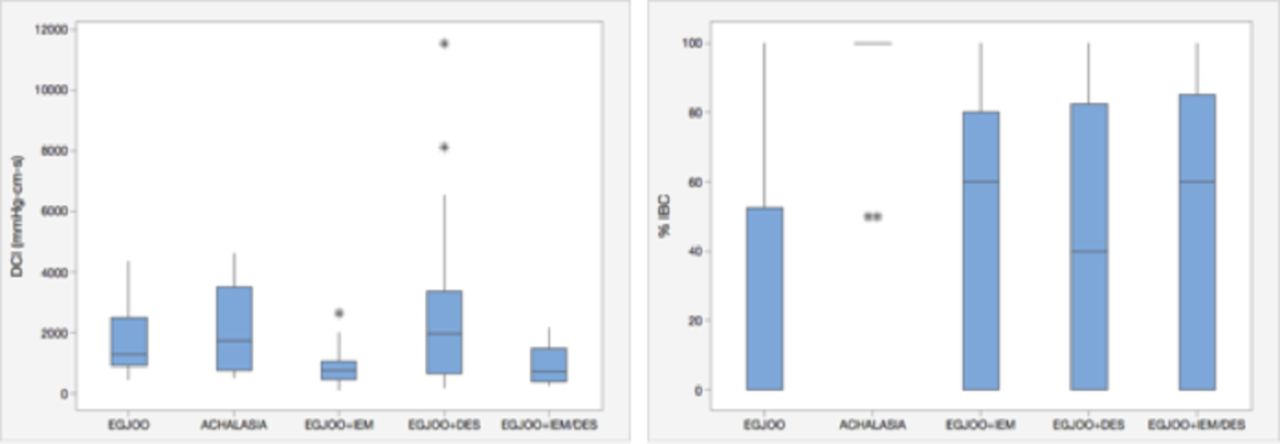
Box plots of the distal contractile integral (DCI) and % incomplete bolus clearance (IBC). Box plots represent minimum and maximum values (vertical lines), first and third quartiles (boxes) and median values (horizontal line). Asterisks represent outlier values. Patients with EGJOO+IEM had statistically lower DCI, while those with EGJOO+DES had higher DCI (p<0.002 between EGJOO+IEM and EGJOO+DES; p<0.001 between EGJOO and EGJOO+IEM). Even the group EGJOO+IEM+DES had statistically lower DCI, when compared with EGJOO+DES (p<0.003). All groups exhibited high percentages of IBC (40%–100%), suggestive of significant oesophageal stasis. DES, diffuse oesophageal spasm; EGJOO, oesophagogastric junction outflow obstruction; IEM, ineffective oesophageal motility.
Seventeen patients in our cohort agreed to a follow-up (f/u) HRM that was performed over a 2-year period and allowed us to assess the HRM diagnosis over time (table 2). Only three patients who had repeat studies had sliding hiatal hernias, measuring 0.6, 1.2 and 1.5 cm in length, respectively. We were surprised to find transition from one diagnosis to the other, with EGJOO preceding or following another diagnosis and remaining as a permanent HRM diagnosis only in 2/17 patients. Only one patient transitioned to achalasia. Figure 6 attempts to summarise the various probabilities when encountering EGJOO with or without associated oesophageal body contractility abnormalities. However, based on table 2, there is a fluidity of the HRM diagnosis that needs to be kept in mind prior to therapeutic decision-making.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
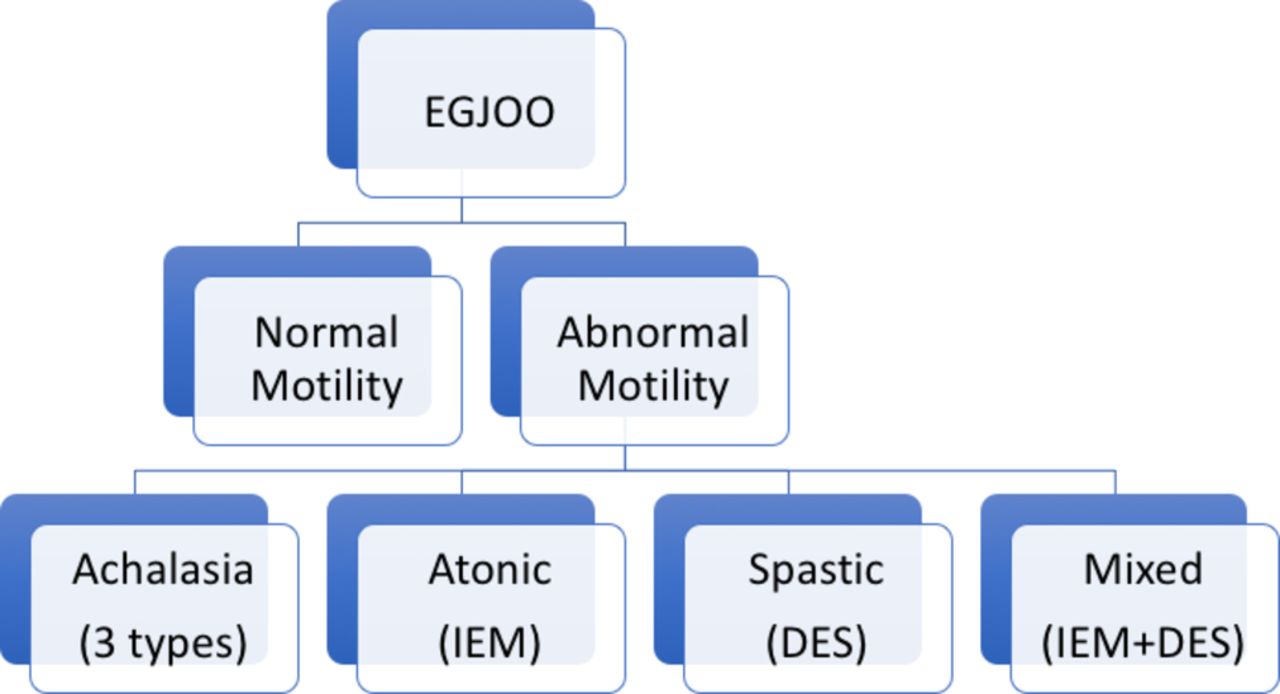
Summary outline of the various probabilities when encountering EGJOO, with or without associated oesophageal body contractility abnormalities, using Chicago Classification (CC) V.3 criteria. In this proposed scheme, we start with the recognition of EGJOO using median integrated residual pressure (IRP) >15 mm Hg as an essential high-resolution manometry (HRM) criterion. We then proceed to independently assess the oesophageal body contractility using CC V.3 criteria and classify it as normal or abnormal, such as achalasia, IEM, DES (including jackhammer oesophagus) or combined IEM+DES. DES, diffuse oesophageal spasm; EGJOO, oesophagogastric junction outflow obstruction; IEM, ineffective oesophageal motility.
Repeat studies and HRM diagnoses using CC V.3.
Discussion
In this study, we describe the clinical and manometric characteristics of our cohort of patients with EGJOO with and without other coexisting CC diagnoses. We hypothesised that patients with EGJOO may have concomitant oesophageal body dysmotility, possibly contributing—at least in part—to their oesophageal symptoms, and that a new subclassification—a modification of the CC—would be more useful clinically. In our proposed scheme, we start with the recognition of EGJOO using median IRP >15 mm Hg as an essential HRM criterion. We then proceed to independently assess the oesophageal body contractility using CC V.3 criteria and classify it as normal or abnormal, such as achalasia, IEM, DES (including JE) or combined IEM+DES (figure 6). In this fashion, we recognise several subtypes of EGJOO, each with variable symptoms of oesophageal dysfunction and each potentially with their own therapeutic implications. This results to two key differences: (1) we incorporate achalasia (all three types) into the five subgroups of EGJOO; (2) in contrast to the hierarchical CC classification, we allow for dual diagnoses, one pertaining to EGJ malfunction, the other to oesophageal dysmotility.
We do not propose to term achalasia as EGJOO. We are using EGJOO as a starting point in defining EGJ physiology and, in its full version, we get achalasia (all three types). We are simply suggesting that the HRM interpretation starts with EGJ assessment that may or may not turn out to be achalasia. We (and others) also acknowledge the possible evolution of EGJOO to achalasia; hence our proposal is not entirely without substance. As for the subcategories and their value, we already have three types of achalasia that are well accepted without knowing for certain if such subcategorisation helps us manage the condition better and much more outcomes research will be needed in this regard. It is because of such clinical and manometric heterogeneity of EGJOO that we propose this new scheme. Specifically, if the EGJOO is associated with DES, treatment with botulinum toxin in the distal oesophagus and the EGJ could improve clinical outcomes. If in contrast, EGJOO is associated with IEM, injection of the EGJ with Botox may precipitate or aggravate acid reflux. Since achalasia may be preceded by the EGJOO diagnosis in some cases and since many authors in the field recommend an f/u HRM to look for achalasia, why not simplify things and start out with EGJ assessment. If present, one can look at the body motility and classify it as achalasia or not and classify it, again using elements of the CC, as the other types of EGJOO that we propose.
EGJOO, a relatively new diagnosis, established by the CC and based on HRM parameters, such as median IRP >15 mm Hg, and is considered relatively rare, ranging from 1.6% to 11%, with few reports in the literature, is mostly retrospective in nature.2 10–12 The condition is characterised by high prevalence of dysphagia (80%), regurgitation (90%) or chest pain (65%), as already reported. In our series of 478 HRM studies performed in symptomatic patients, the prevalence of EGJOO was 24% with more than 50% being associated with other motility disorders, such as DES, JE, or IEM. In addition to the well-described structural abnormalities reported in other series (such as hernia, fundoplication), we encountered many patients suffering from functional (idiopathic) EGJOO associated with Parkinson’s disease, GERD and EoE, which ranged from 16% to 79% and possibly explains the intermittent nature of this condition.
In our cohort and like other studies, symptoms in patients with EGJOO did not always require treatment and treatment response was variable, suggestive of a considerable degree of heterogeneity.2 4 Because of inherent biases in the assessment of therapeutic response to intervention in a retrospective study without the use of specific endpoint assessment, we were not able to decipher any differences among the five subtypes. Nevertheless, surgery (primary or reparative), endoscopic injection or botulinum neurotoxin to the EGJ, distal oesophagus or both, and endoscopic balloon dilation of the EGJ were used. In our cohort and despite observation of longer than 2 years, we only observed evolution of EGJOO to achalasia in one patient, unlike prior studies.4 11 However, this possibility needs to be considered and repeat evaluation because of the efficacy and availability of established treatment options for any of the subtypes of achalasia.13 Our study was also enriched by several patients who, despite the discomfort of HRM, underwent repeat (second and third) HRM over the course of 2 years (table 2). These data suggested a fluidity of the manometric diagnosis over time, questioning our ability to firmly establish the diagnosis and emphatically decide on therapy. For these reasons, longitudinal follow-up and repeat HRM should be suggested to recognise evolution towards achalasia, and towards regression or recharacterisation to another diagnosis. We believe that our proposed classification, matched by a repeat assessment 3–6 months later, may allow a better characterisation and hopefully lead to better therapeutic outcomes.
Oesophageal body and/or EGJ dysmotility may be primary or secondary to other conditions that structurally or functionally involve the oesophagus. As shown in table 1, a significant number of our patients had GERD and Parkinson’s disease. To what degree these conditions coexist or are causally related to the EGJOO and the exact mechanism(s) by which such relationship exists or evolves is unclear, but both have the potential to alter muscle function intermittently and variably over time, thereby potentially explaining the variability of the HRM diagnosis seen or repeat testing (table 2).14 15 For example, it is possible that episodic EGJOO with or without associated oesophageal body alterations, such as DES, IEM or both, could explain the well-known phenomenon of chest pain or non-obstructive dysphagia that have been well described in GERD.8 9
Our findings and our proposed new approach are in complete agreement with the study of Zheng et al who sought to determine the frequency of abnormal body motility and/or abnormal bolus movement in patients with EGJOO.16 In their series of patients, 56 (40%) were diagnosed with an abnormal motility pattern to liquids (IEM=28, DES=19, JE=6), of which 44 (76%) had abnormal bolus transit to liquids, viscous or both. Among patients with abnormal bolus transit, dysphagia and heartburn were common, like in our cohort. They concluded that a significant percentage of patients with EGJOO have abnormal oesophageal body motility and/or abnormal bolus transit and suggested that current criteria do not allow for the description of other abnormalities in oesophageal motility and bolus transit among patients who are given the diagnosis of EGJOO.
There are several strengths and limitations in our study. First, although cohort and observational in nature, our study involved many patients presenting with various oesophageal symptoms who were studied in detail and highlights the possibility of a link between oesophageal body and EGJ motor dysfunction heretofore unexplored. Second, the study population—the largest series to date—was community based, who mostly suffered by frequent but mild to moderate symptoms of oesophageal dysfunction. Therefore, our findings are generalisable and not limited to those patients with severe or protracted disease referred to tertiary centres. Third, this is the only study where repeat manometric evaluation was performed in a cohort of patients with EGJOO, highlighting the fleeting nature of this diagnosis. Some limitations need to be kept in mind. First, oesophageal impedance/pH-metry was not used in all subjects; therefore, the presence of pathologic acid/non-acid reflux could not always be ascertained or quantified. Second, our population was not assessed using elaborate and well-validated GP questionnaires but instead, through our simpler, general and practical tool previously validated and used in many previous studies in our practice setting.5 14 Third, given the retrospective nature of our study, we could not quantify the impact of selected therapy, if any. Fourth, we did not use EUS or barium radiography in the vast majority of our cohort since we were able to clarify structure based on endoscopy and, at times, CT imaging. Fifth, it is possible that the patients who underwent HRM testing represented a select group of patients with EGJOO with higher prevalence and severity of oesophageal symptoms that justified the performance of HRM, resulting in overestimation of our results. This may be particularly true of the patients with Parkinson’s disease (n=28), who comprised a significant subset of this study population (table 1). Given the uncertain evolution of EGJOO, it has been our practice to encourage patients to undergo f/u HRM; a fraction of them comply mostly because they remain symptomatic and not responding to any effort at therapy. Those with mild symptoms or those who improve are not (understandably) interested in repeat studies. A prospective study would be important to clarify this issue and eliminate selection bias. Finally, we have scattered information of variable therapies applied but in order to validate their impact one needs standardisation of outcome assessments. This was a retrospective first effort to subclassify the patients with EGJOO into groups in a way similar to achalasia subgrouping and then look at therapeutic outcomes. Therapies to be explored would be EGJ balloon dilation (variable sizes), Botox injection of the EGJ ± the lower oesophagus, prokinetics, and so on.
In summary, we believe that EGJOO is an intermittent manometric finding within a heterogeneous group of patients and is associated with other—overlapping—HRM diagnoses which, in this study, we tried to subcategorise. Symptoms may or may not reflect this additional diagnosis and management may vary, including medications, endoscopic interventions or avoidance of treatment. EGJOO was not persistent in the majority of patients retested. This temporal variability and prominent coexistence with other motility diagnoses raise questions as to the clinical significance of EGJOO. Going forward, we suggest that EGJOO not be characterised as a major motility disorder and future classification schemes should specify whether EGJOO is in isolation or linked with another motility diagnosis. A lot more work can be done looking at correlations between timed barium studies, impedance/pH, EndoFLIP, EUS, and so on, and the point of this work was to highlight some useful features to clinicians and to further research. Prospective studies will be needed to validate such subgrouping of EGJOO or further modifying it into clinically relevant clinical entities.
References
Footnotes
Contributors GT: Planning and/or conducting the study; collecting and/or interpreting data; drafting the manuscript and revision; JOC: Collecting and/or interpreting data; drafting the manuscript and revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval El Camino IRB.
Provenance and peer review Not commissioned; externally peer reviewed.