Article Text

Abstract
Introduction and purpose Patients with pancreatic cancer (PC) have long been known to have high rates of depression. Depression in patients with PC can be linked to sleep disturbance. The American College of Sports Medicine notes that physical exercise is safe for most patients with cancer and physical inactivity should be avoided. However, clinical impacts of exercise interventions (EIs) on patients with PC have been poorly investigated. We aim to prospectively examine the effect of EIs on sleep disturbance in patients with PC using actigraphy, which is an objective measurement of motor activity and sleep.
Methods and analysis This trial is a non-double blind randomised controlled trial. Standard therapy for each patient with PC will be allowed. When registering study subjects, a thorough assessment of the nutritional status and the daily physical activities performed will be undertaken individually for each participant. Study subjects will be randomly assigned into two groups: (1) the EI and standard therapy group or (2) the standard therapy group. In the EI and standard therapy group, physical activities equal to or higher than walking for 60 min/day will be strongly recommended. The primary outcome measure is the sleep-related variable using actigraphy (activity index) at 12 weeks.
Ethics and dissemination The trial received approval from the Institutional Review Board at Hyogo College of Medicine (approval no. 2769). Final data will be publicly announced. A report releasing the study findings will be submitted for publication to an appropriate peer-reviewed journal.
Trial registration number UMIN000029272; Pre-results.
- pancreatic cancer
- pancreas
- nutritional status
- quality of life
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Pancreatic cancer (PC) is an aggressive disease, representing the fourth cause of cancer-related deaths worldwide.1–4 Majority of patients with PC have unresectable, locally advanced or metastatic disease at the time of diagnosis and the 5-year overall survival (OS) rate in patients with PC with advanced tumour status is extremely low.1–4 The proportion of patients with PC who can proceed with curative intent (eg, surgery) is less than 20%.1–4 Currently, there is no standard programme for screening patients at high risk of PC.1–4 For more than a decade, gemcitabine has been the cornerstone for the treatment of patients with advanced PC, despite a small advantage in terms of OS.5 6 On the other hand, patients with PC have long been known to have high rates of depression.7 8 The aetiology of depression in patients with PC may be traced to more than the poor prognosis of PC and the pain it causes.7 8 In addition, depression in patients with PC can be linked to sleep disturbance.9 Appropriate symptomatic management is therefore critical for patients with PC.
Regular physical activity favourably influences the risk for disease onset and the progression of several malignancies.10–19 Cancer survivors who exercise can potentially benefit from reduced levels of fatigue and improved quality of life (QOL) and physical function.20 The American College of Sports Medicine notes that exercise is safe for most cancer survivors and physical inactivity should be avoided.21 However, clinical impacts of exercise interventions (EIs) on patients with PC have been poorly investigated.
Decreased QOL in patients with PC can cause sleep disturbance, and poor sleep quality can further negatively influence QOL. Sleep disruptions have been extensively examined through the use of actigraphy, which is an objective measurement of motor activity and sleep.22–25 The nature of sleep disturbance often varies as a function of objective versus subjective evaluation.26 Actigraphy is the most frequently used brand by investigators, and it is a non-invasive and cost-effective medical device used to assess the sleep quality compared with polysomnography, since it is the size of a wristwatch and can be worn without interfering daily activities.22–25 27
Despite clinical benefits of EI on patients with cancer, there are limited data available with regard to patients with PC undergoing EI on sleep disturbance. There is therefore urgent need to examine this issue. In this study, we aim to prospectively examine the effect of EI on sleep disturbance in patients with PC using actigraphy.
Eligibility of study subjects
In patients with PC with poor nutritional status, EI may be accompanied with increased health risks, as EI may cause further protein catabolism and muscle mass decline.28–30 When registering study subjects, a thorough assessment of the nutritional status and the daily physical activities performed will be done individually for each participant. For all potential study subjects, the researchers will explain in detail the study purposes, procedures and potential relevant benefits and risks of this trial in a written informed manner. The researchers must let every potential study subject know that they have the right to withdraw consent at any time throughout the study period. All potential study subjects must be given sufficient time for careful consideration prior to making decision. All study subjects must sign the consent before they can participate in the study. Written informed consents will be kept as a part of the clinical trial documents.
Inclusion criteria
Both sexes.
Patients with PC aged 20 years and more. A diagnosis of PC will be based on the current Japanese guidelines.31 The severity for PC (clinical stage) will be determined based on Union for International Cancer Control classification system.32
Patients with Eastern Cooperative Oncology Group (ECOG) performance status (PS) 0 or 1.
Exclusion criteria
PC subjects with severe depression or psychiatric disorder such as those with high scores in patient health questionnaire.
PC subjects with far advanced tumour status with massive ascites that participation in this trial is anticipated to be difficult.
PC subjects with severe underlying diseases, such as severe infectious diseases, severe chronic heart failure and respiratory disorders.
Pregnant or lactating female patients with PC.
PC subjects who may be at a risk of falls.
PC subjects considered unsuitable for this trial due to the inability to participate in EI.
PC subjects considered unsuitable for this trial due to other reasons.
Study protocol
Study design: single-centre non-double blind randomised controlled trial
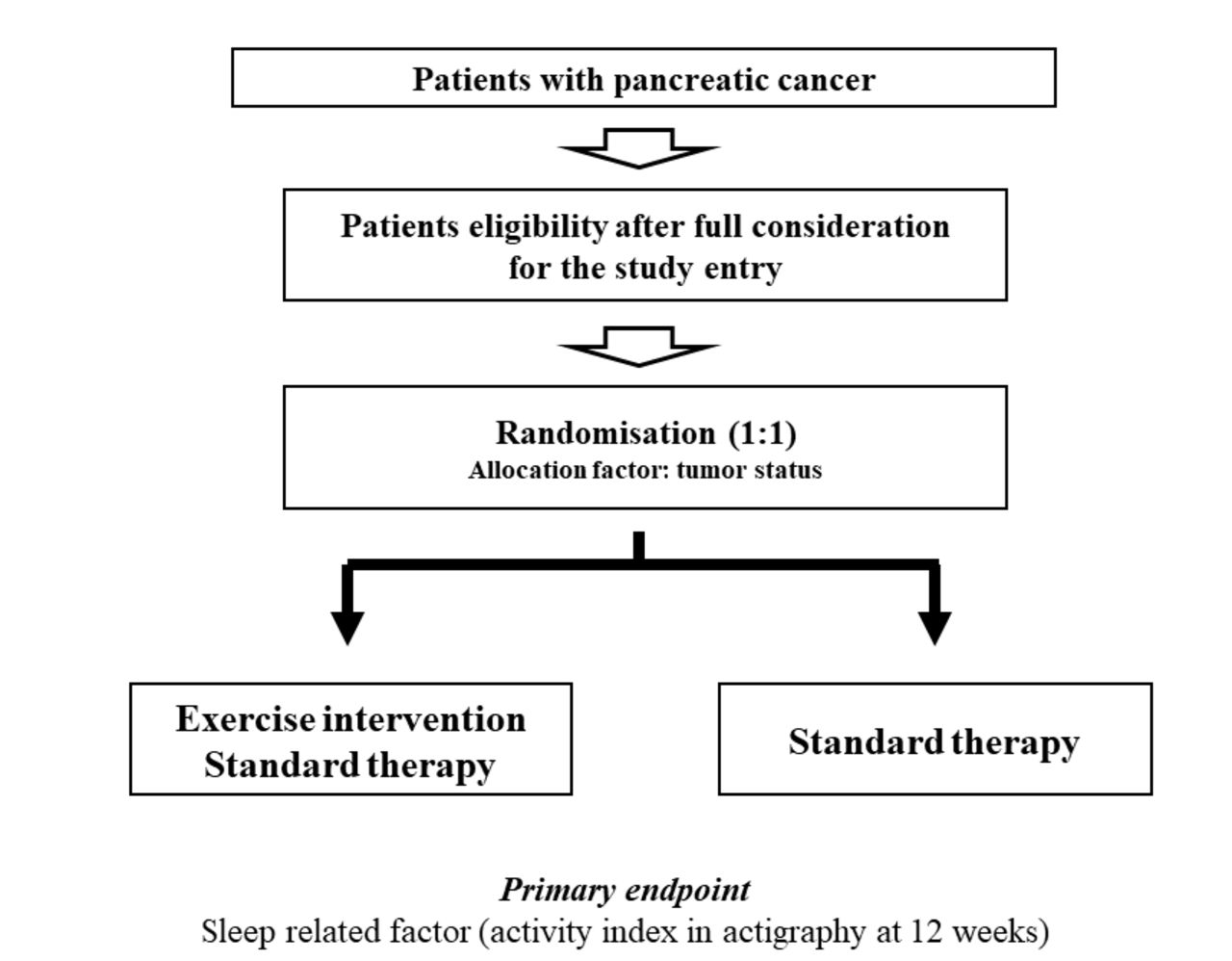
Our study subjects are patients with PC. All clinical stages (stages I, II, III and IV) of PC can be considered for participation in this study. Standard therapy for each patient with PC will be allowed. Study subjects will be randomly assigned into two groups: (1) the EI and standard therapy group or (2) the standard therapy group (figure 1). Standard therapies such as surgery and systemic chemotherapy will be selected according to tumour status and baseline characteristics in each patient through discussion with surgeons and oncologists.16 31 Adding new medicines for sleep disturbance during study period will not be allowed.

Study design.
Exercise interventions
The declines in physical abilities and physiological function that are commonly seen in patients with cancer can be minimised or prevented with a well-thought-out exercise programme.20 In the EI and standard therapy group, guidance for EI will be provided for each participant once a month at the outpatient nutritional guidance clinic. Participants will also be instructed to do exercises with ≥3 metabolic equivalents (mets; energy consumption in physical activities/resting metabolic rate) for 60 min/day and to do exercises >23 mets/week.10–15 In the EI and standard therapy group, physical activities equal to or higher than walking for 60 min/day will be strongly recommended for each study subject because insufficient patient education may contribute to the belief that exercise is not helpful. In both groups, standard therapies for PC will be permitted and we will ask all study subjects to self-declare their daily amount of exercise. Direct monitoring of EI will not be undertaken.
Evaluation using actigraphy
Actigraphy is a medical device for gathering objective sleep/awake data in the natural sleeping surroundings over an extended time period.22–25 The study subjects will be advised to wear a wrist actigraphy on their non-dominant wrist over a period of 3 days based on the manufacturer’s information.22–25 Evaluation by actigraphy will be carried out at 4-week intervals. The follow-up period in each subject will be 12 months. At the same time points, data for laboratory testing, questionnaire, and clinical symptoms will be also gathered. Principally, study subjects will be advised to visit our hospital in an outpatient basis.
Data in the actigraphy will be downloaded into a dedicated computer program. The following five sleep-related factors will be utilised for assessment as mentioned elsewhere: (1) sleep onset latency, (2) wake after sleep onset (defined as the minutes awake during the sleep period after the beginning of sleep (the first two continuous minutes scored as sleep)), (3) activity index (average amount of activity in sleep), (4) wake episodes (total number of wake counts between trying to start to sleep and wake-up times) and (5) sleep episodes in daytime (total number of sleep counts in daytime).23 The increase in each score suggests the worse sleep quality. Activity index will be assessed as a primary outcome measure because it can well reflect sleep quality.23 A representative case in actigraphy is presented in figure 2.

{kind=link}
{kind=link}
A representative case in actigraphy. Black thin line means activity level, red bold line means sleeping state and light blue rectangle means time in bed.
Time to start EI
In the EI group, when the general condition of study subjects is stable after the initial standard therapy and EI is judged to be enforceable safely by the attending physicians, EI will be initiated as soon as possible.
Primary endpoints (confirmatory)
Sleep-related variable using actigraphy (activity index) at 12 weeks.
Secondary endpoints (exploratory)
Questionnaire survey
Sleep rhythm and depressed state in daily life will be assessed using questionnaire surveys (the Beck Depression Inventory, Second Edition (BDI-II)33 and Pittsburgh sleep quality index34).
Changes over time in baseline characteristics
Changes over time to the following baseline parameters will be assessed: body weight, body mass index, white cell count, platelet count, serum albumin level, aspartate aminotransferase, alanine aminotransferase, total cholesterol, triglyceride, low-density lipoprotein, high-density lipoprotein, fasting blood glucose, haemoglobin A1c, homeostasis model assessment of insulin resistance and tumour markers.
Follow-up and standard of care
During the observation period and after completion of the trial, all study subjects will be seen in clinic every 4 weeks to address complications from PC and other comorbidities. In both groups, standard therapies for PC will be continued. Regular laboratory tests (haematology, biochemistry and coagulation) will be required at the trial entry and at the completion of this trial and on an as-needed basis.
Case registration period
From October 2017 to March 2021.
Data collection
A study assistant will collect data elements from medical records in each patient, including:
Baseline data:
Sex and age.
Height and body weight.
Vital signs and ECOG-PS.
History of alcohol consumption and history of smoking.
Disease severity of PC (clinical stage).
Previous treatment and medication.
Comorbid conditions.
Baseline laboratory tests.
Presence or absence of ascites or distant metastases on radiologic findings.
Statistical methods
Descriptive statistics
Data will be subjected into JMP software (SAS Institute, Cary, North Carolina, USA), and all relevant data will be checked to confirm consistency. Data at each time point will be compared. Quantitative factors will be compared using a paired or an unpaired t-test. Categorical factors will be compared using Pearson χ2 test or Fisher’s exact test, as appropriate. We will perform statistical analyses on an intention-to-treat basis, by which all study subjects will be analysed in the group which they are assigned to. Multivariate analysis for the improvement of activity index in actigraphy will also be performed.
Sample size estimation
Based on results of our preceding study regarding actigraphy, supposing that the α error (type 1 error) is 0.05, the detection power (β) is 0.8, the difference in the two groups to be detected and measured using bioimpedance analysis (BIA) is 10 and the SD of outcome is 10, the number of required participants in both groups will be 17 (total of 34 participants) in order to randomly allocate one to one.17 Randomisation will be performed using the clinical stage of PC as an allocation factor for matching baseline characteristics between the two groups. We anticipate that a number of participants may drop out of the study; therefore, a total of 40 participants will be necessary to confirm our hypothesis.
Discussion
Cancer therapies cause profound debilitation that leads to reduced physical function and impairs QOL.20 EIs benefit patients with cancer.35 A recent study reported that EI may have a potential favourable impact on tumour outcome by reducing insulin resistance.36 The clinical significance of EI has recently gained considerable attention due to the multiple health benefits of EI.10–19 In that sense, our current study protocol and relevant data may be worth reporting. To the best of our knowledge, this is the first prospective interventional clinical trial that will objectively assess the influence of EIs on sleep disturbance in patients with PC.
From a clinical practice perspective, we highlight the potential safety risks of EIs in patients with PC with poor nutritional status or poor PS, because EI may risk promoting further protein catabolism and muscle mass loss. An appropriate nutritional assessment will be needed prior to starting EIs and patients with PC with PS 2 or more will be excluded.
One of the major strong points in our study is that this will be a RCT. We acknowledge one relevant study limitation; this study will be based solely on a Japanese population. Additional research in different ethnic populations will be required to further verify the efficacy of EI in sleep disturbance and to extrapolate our results to other ethnicities. However, if the clinical efficacy of EI for sleep disturbance in patients with PC is confirmed in this RCT, the information we provide may be beneficial to clinicians.
Ethics and dissemination
Research ethics approval
Ethical approval for this trial was granted by the Institutional Review Board at Hyogo college of medicine (approval no.2769). The study protocol, informed consent form and other submitted documents were reviewed and approved. Throughout the trial period, Declaration of Helsinki will be strictly followed in order to guarantee the right of the study subjects. Trial registration number is UMIN000029272 (https://upload.umin.ac.jp/); pre-results. No patient is registered at the submission of our manuscript.
Confidentiality
All study subjects data will be stored securely. All relevant documents will be locked up and preserved at the Department of Hepatobiliary and Pancreatic Disease, Department of Internal Medicine, Hyogo College of Medicine, Hyogo, Japan, in accordance with data protection procedures. For each study subject, all data collected during the study period will be identified by a serial number and a name acronym in the case report forms.
Dissemination policy
Final data will be publicly disseminated irrespective of the study results. Results will be presented at relevant conferences and submitted to an appropriate peer-reviewed journal following trial closure and analysis.
References
Footnotes
Contributors KY designed the study and wrote the initial draft of the manuscript. HN and HE contributed to the analysis and interpretation of data and assisted in the preparation of the manuscript. NI, YI, AI, YY, YM, KH, CN, RT, TN, NA, YS, NIk, TT, HI and SN contributed to data collection and interpretation, and critically reviewd the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.