Article Text

Abstract
Background Since direct-acting antivirals (DAAs) have been approved for the treatment of hepatitis C virus (HCV) infection, a small series of patients with new-onset neuropsychiatric alterations have been referred to us. We therefore set out to study neuropsychiatric function in relation to DAAs prospectively.
Methods Ten patients with cirrhosis and 12 post-liver transplant (post-LT) patients were enrolled. All underwent wake electroencephalography (EEG) and a neuropsychological evaluation (paper and pencil battery, simple/choice reaction times, working memory task) at baseline, at the end of treatment with DAAs and after 6 months. At the same time points, full blood count, liver/kidney function tests, quantitative HCV RNA, ammonia and immunosuppressant drug levels were obtained, as appropriate.
Results Patients with cirrhosis were significantly older than post-LT patients (65±12 vs 55±7 years; P<0.05). Neuropsychological performance and wake EEG were comparable in the two groups at baseline. At the end of a course of treatment with DAAs, a significant slowing in choice reaction times and in the EEG (increased relative delta power) was observed in patients with cirrhosis, which resolved after 6 months. In contrast, no significant changes over time were observed in the neuropsychiatric performance of post-LT patients. No significant associations were observed between neuropsychiatric performance and stand-alone/combined laboratory variables.
Conclusion Some degree of neuropsychiatric impairment was observed in relation to treatment with DAAs in patients with cirrhosis, but not in post-LT patients, suggesting that the former may be sensitive to mild DAA neurotoxicity.
- chronic hepatitis
- chronic liver disease
- drug toxicity
- hepatitis c
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this topic?
Limited information is available on the effects of direct-acting antivirals on cognitive performance.
What are the new findings?
We report mild, transient worsening in cognitive and neurophysiological performance in patients with cirrhosis at the end of a course of treatment with a sofosbuvir-based regimen.
No such changes were observed in a group of younger but otherwise comparable patients treated for post-liver transplantation hepatitis C recurrence.
How might it impact on clinical practice in the foreseeable future?
Caution may be needed when treating patients with cirrhosis with sofosbuvir-based regimens, especially if there is a history of hepatic encephalopathy and/or neurological or psychiatric comorbidity.
Introduction
The recent approval of highly effective and well-tolerated direct-acting antiviral (DAA) regimens has dramatically changed the approach to hepatitis C virus (HCV) infection management. Over the last few years, several prospective trials have proven the effectiveness of DAAs in both patients with cirrhosis1–3 and transplanted patients with HCV recurrence.3–5 For the majority of the all-oral anti-HCV DAAs approved regimens, sofosbuvir (SOF) represents the pangenotypic backbone of the combination therapy, acting as a nucleotide analogue that inhibits the NS5B protein of HCV.6
In Italy, SOF was approved at the end of December 2014, and over the subsequent year two further drugs were approved, namely simeprevir and ledipasvir. Over the first few months after the introduction of DAAs in our clinical practice, a number of patients on antiviral therapy (eight with cirrhosis and one postliver transplant (post-LT)) were referred to author SM for formal neuropsychiatric evaluation because of new-onset alterations/hepatic encephalopathy. While no obvious causal relationships could be established, it is of interest that all eight patients with cirrhosis had no history of overt hepatic encephalopathy, and only two had experienced some degree of deterioration in liver function while on DAAs. Referrals came from four different clinicians working in different departments, three of whom raised the possibility of drug-related neurotoxicity based on the observed time course of symptoms development. We therefore set out to study neuropsychiatric function in relation to DAAs prospectively.
Patients and methods
Twenty-two consecutive patients, 10 with HCV-related cirrhosis (40% male; age 65±12, all Child A, average model for end-stage liver disease (MELD) 8±1) and 12 post-LT patients with HCV recurrence (75% male; age 55±7, none with cirrhosis), were enrolled between January 2015 and June 2016, when they were scheduled to start treatment with DAAs (SOF+ribavirin (n=6 cirrhosis; n=9 post-LT), SOF+simeprevir (n=3 cirrhosis; n=3 post-LT) or SOF+ledipasvir (n=1 cirrhosis)), based on the Italian Drug Agency directives at the time. All were studied immediately prior to treatment commencement (baseline), at the end of the treatment course and after 6 months. At each time point, a full blood count, liver/kidney function tests, quantitative and qualitative HCV-RNA and venous ammonia levels were obtained. The Child-Pugh and MELD scores were calculated in patients with cirrhosis and the levels of immunosuppressants measured in post-LT patients. A summary of demographic and laboratory values is presented in table 1.
Demographic and laboratory values, by study group and study time
Neuropsychiatric assessment
Patients underwent comprehensive neuropsychiatric evaluation to include a detailed medical history, exclusion of concomitant neurological disorders and a clinical grading of the neuropsychiatric abnormalities according to the West Haven criteria (vide infra), where appropriate. Procedures were performed under standardised conditions in the morning, after breakfast, in a quiet and well-lit room.
Paper and pencil psychometry
Number Connection Tests A and B, as well as the Digit Symbol, Line Tracing and Serial Dotting tests, were administered, and the results were scored in relation to age-adjusted and education-adjusted Italian norms. Performance was classified as impaired if the sum of the SD for the individual tests, referred to as the Psychometric Hepatic Encephalopathy Score (PHES), was ≤−4; the mean of the z scores for each subtest was also used for purposes of correlation analysis.7 8
Computerised psychometry: the Scan package
Simple reaction time
The subject is required to press the spacebar in the keyboard in response to a series of visual stimuli. The number of correct responses is expressed as a percentage of the total number of stimuli (accuracy), and the accuracy-adjusted, average, simple reaction time (ms) is calculated.
Choice reaction time
The subject is presented with either the number 1 or 3 on the computer screen and is required to press 1 or 3 on the keyboard accordingly. The number of correct responses is expressed as a percentage of the total number of stimuli (accuracy), and the accuracy-adjusted, average choice reaction time (ms) is calculated.
Scan reaction time
This is a digit recognition task based on the Sternberg paradigm. The subject is presented with a series of 36 consecutive pairs of numbers and is asked to press 1 if they have common digits (ie, 3456 and 768) and 3 if not (ie, 123 and 789). The number of correct responses is expressed as a percentage of the total number of stimuli (accuracy), and the accuracy-adjusted, average Scan reaction time (ms) is calculated.
The overall result of the Scan test is expressed as a z score, which is corrected for age and educational attainment. z Scores ≤−2 are considered abnormal.9
Wake EEG
Electroencephalography (EEG) was recorded for 10 min, with eyes closed, in a condition of relaxed wakefulness, using a 21-electrode EEG cap. Electrodes were placed according to the International 10–20 system; the ground electrode was Fpz; the reference electrode was Oz; and impedance was kept below 5 k. Each channel had its own analogue-to-digital converter; the resolution was 0.19 lV/bit (Brainquick 3200, Micromed, Mogliano Veneto, Italy). One continuous 80–100 s period of artefact-free EEG tracing was selected for subsequent spectral analysis by fast Fourier transform. The following spectral parameters were calculated on the P3-P4 derivation: the mean dominant frequency, which is an estimate of the background frequency of the EEG, and the relative power of the spectral bands delta (1–3.5 Hz), theta (4–8 Hz), alpha (8.5–13 Hz) and beta (13.5–25.5 Hz). EEGs were classified as normal/abnormal based on the spectral criteria proposed by Van der Rijt et al 10 and subsequently modified by Amodio et al.11
In patients with cirrhosis, neuropsychiatric status was classified as unimpaired: no clinical evidence of hepatic encephalopathy (HE) and both normal PHES and normal EEG; covert HE: no obvious clinical abnormalities (grade 0 or grade I according to the West Haven criteria)12 but abnormal PHES and/or EEG; and overt HE: clinically obvious neuropsychiatric disturbances (grade II or over according to the West Haven criteria).12 13 Scan test package abnormalities were described singly, and so were any neuropsychological or EEG abnormalities in post-LT patients.
Statistical analysis
Results are expressed as mean±SD or ±95% CI. Variable distribution was tested using the Shapiro-Wilk’s test. Descriptive statistics and the Student’s t-test/Mann-Whitney U tests were used, as appropriate, to compare the two groups. Differences in neuropsychological and electrophysiological performance over time were compared by repeat-measures analysis of variance (ANOVA), by group. The latter analyses were performed for the six patients with cirrhosis/10 post-LT patients with available T1 and T2, and for the five patients with cirrhosis/seven post-LT patients with available T1, T2 and T3. In order to test for the possibility that ribavirin may have played a role, post-hoc factorial ANOVA (categorical predictors ‘patient group’ and ‘ribavirin yes/no’) was performed on the two variables (relative delta power and choice reaction time), which were shown to change significantly at T2.
Ethics
All participants provided written, informed consent. The study was conducted according to the Declaration of Helsinki (Hong Kong Amendment) and Good Clinical Practice (European) guidelines.
Results
Patients with cirrhosis were significantly older than post-LT patients (65±12 vs 55±7 years; P<0.05), while no differences were observed in terms of sex distribution (4/10 men in the cirrhosis group, 8/12 men in the post-LT group) and educational attainment (9.6±2.0 vs 9.6±1.8) in the two groups. Sustained virological response was achieved in 80% and 100% of patients with cirrhosis and post-LT patients, respectively (table 1).
Baseline (T1)
Seven out of the 12 post-LT patients had a history of overt HE prior to transplantation; none exhibited abnormalities on PHES, one had abnormal Scan test performance (z score) and one showed grade I EEG slowing. By contrast, none of the patients with cirrhosis had a history of overt HE, none had overt HE at baseline, none had an abnormal PHES, one had abnormal Scan test performance (z score) and three showed grade I EEG slowing. Average neuropsychological performances and EEG spectral parameters were comparable in the two groups at baseline, although slow EEG activity (theta) tended to be higher in patients with cirrhosis (<0.05<P<0.1) (tables 2–4).
Baseline Scan package performance, by patient group
Baseline electroencephalography spectral parameters (P3-P4 derivation), by patient group
Number of patients with abnormal neuropsychological/electrophysiological performance at different time points, by group
End of treatment (T2)
Out of 22 patients enrolled, 16 underwent the second assessment (out of the six who did not, four were patients with cirrhosis, two of whom had been transplanted in the meantime). Out of the 10 post-LT patients evaluated at the end of treatment, none had abnormal PHES, none had an abnormal Scan test performance and one had grade I EEG slowing (same patient as in T1). Out of the six patients with cirrhosis evaluated at the end of treatment, none had abnormal PHES, one had abnormal Scan test performance (same patient as in T1) and one had grade I EEG slowing (same patient as in T1). Taken as a group, patients with cirrhosis showed significant slowing in choice reaction times and increased extra-slow activity (relative delta power) on the wake EEG. In contrast, no significant changes were observed in the post-LT group (figure 1: 6 patients with cirrhosis and 10 post-LT patients; and figures 2–3: 5 patients with cirrhosis and 7 post-LT patients).

Mean (±95% CI) relative delta power at baseline and at the end of treatment in patients with cirrhosis (n=6, black circles) and post-transplant patients (n=10, grey squares). Patient group: P=0.031; time: P=0.025; patient group × time: P=0.011. EEG, electroencephalography.
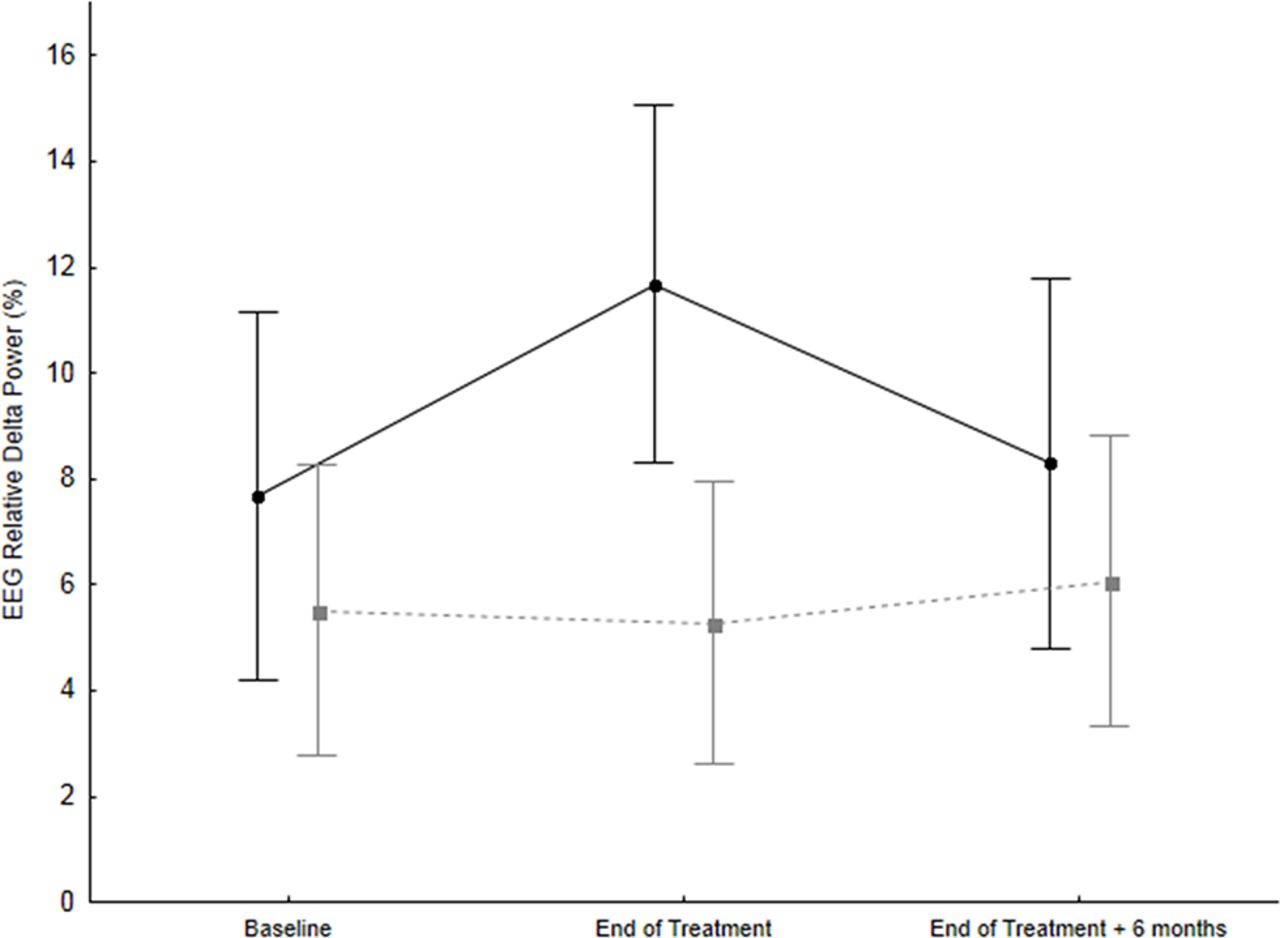
Mean (±95%CI) relative delta power at baseline, at the end of treatment and 6 months after the end of treatment in patients with cirrhosis (n=5, black circles) and post-transplant patients (n=7, grey squares). Patient group: P=0.069; time: P=0.063; patient group × time: P=0.016. EEG, electroencephalography.
{kind=link}
{kind=link}
{kind=link}
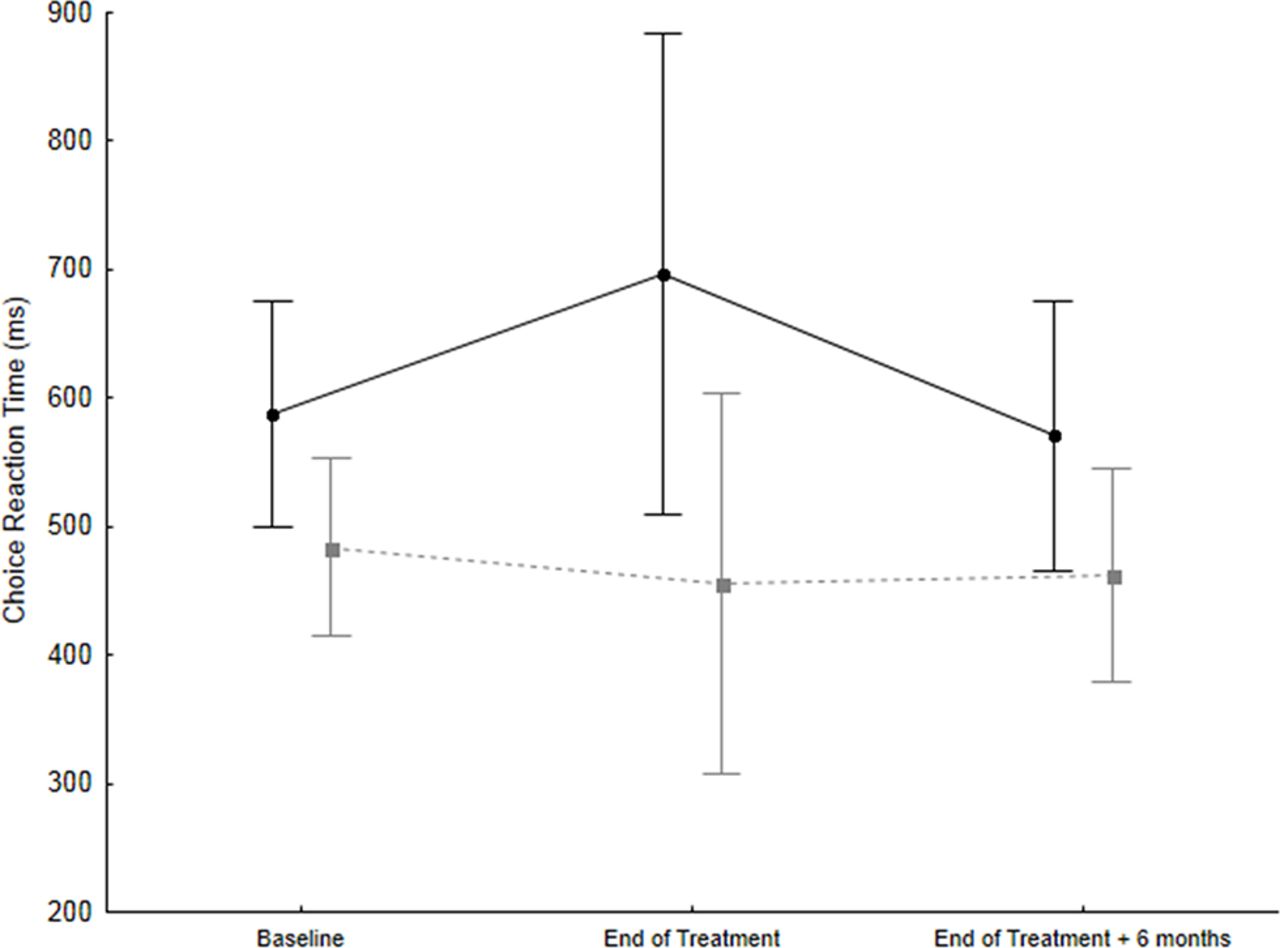
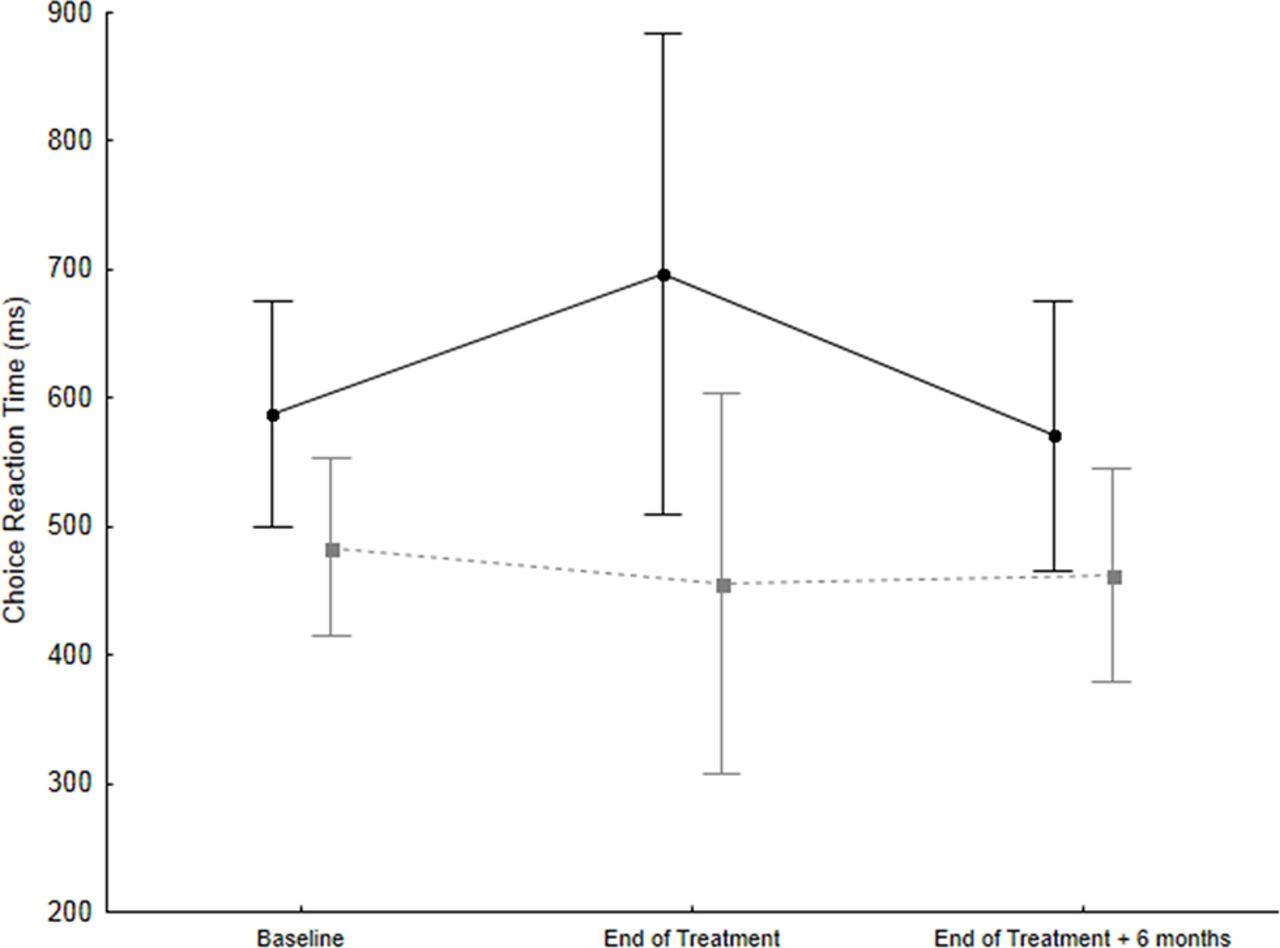
Mean (±95%CI) choice reaction time on the Scan package at baseline, at the end of treatment and 6 months after the end of treatment in patients with cirrhosis (n=5, black circles) and post-transplant patients (n=7, grey squares). Patient group: P=0.048; time: P=0.200; patient group × time: P=0.083.
End of treatment + 6 months (T3)
Out of 22 patients enrolled, 16 underwent the third assessment (10 post-LT patients and 6 patients with cirrhosis). Out of the 10 post-LT patients evaluated at the end of treatment, none had abnormal PHES, Scan test or EEG. Out of the six patients with cirrhosis who were evaluated at T3, none had abnormal PHES, one had an abnormal Scan test performance (same patient as in T2) and none showed EEG slowing.
All three assessments were available for 12 patients (five with cirrhosis and seven post-LT). When quantitative neuropsychiatric measures were analysed over time, at T2 (the end of the course of DAAs treatment) patients with cirrhosis exhibited a significant slowing in choice reaction times and the EEG (increased relative delta power), which resolved after 6 months (P=0.01) (figures 2–3: five patients with cirrhosis and seven post-LT patients). At T2, three patients (two with cirrhosis and one post-LT) reported tiredness/irritability during the course of treatment. Their performance did not appear to be different compared with that of patients who did not report symptoms, although formal subgroup analysis was not possible due to insufficient power.
No significant associations were observed between neuropsychiatric performance and stand-alone/combined laboratory variables. In particular, no increase in ammonia levels was observed in patients with cirrhosis at T2 (table 1). Similarly, no changes were observed in immunosuppressive drug levels (all within the range) at different time points and no correlation was observed between such levels and neuropsychiatric performance in post-LT patients. Finally, while only two patients (both with cirrhosis) did not achieve sustained virologic response (SVR), their performance did not appear to be different compared with that of patients who did, although formal subgroup analysis was not possible due to insufficient power.
In order to test for the possibility that ribavirin may have played a role, post-hoc factorial ANOVA (categorical predictors ‘patient group’ and ‘ribavirin yes/no’) was performed on the two variables (relative delta power and choice reaction time), which were shown to change significantly at T2. This did not confirm a role for ribavirin, but power does not allow to reach definite conclusions in this respect.
Discussion
Some degree of neuropsychiatric impairment was observed in relation to treatment with SOF-based regimens in patients with cirrhosis, but not in post-LT patients, suggesting that the former may be more sensitive to mild SOF-based regimens neurotoxicity.
At the end of a course of treatment with an SOF-based regimen, patients with cirrhosis exhibited an increase in extra-slow EEG activity and a slowing in their reaction times. None of them presented clinical features of overt hepatic encephalopathy and they showed no variations in either ammonia levels or MELD/Child-Pugh scores. Thus, it is unlikely that the cognitive changes recorded can be ascribed to hepatic encephalopathy. The alterations recorded at the end of treatment resolved at 6 months, possibly indicating mild SOF-based regimen neurotoxicity. Unfortunately, no evaluations were planned over the treatment period (eg, at 4 or 8 weeks) for this study, which may have been of value. These may be considered for future research on the topic. Interestingly, it has been recently demonstrated that HCV eradication with DAAs leads to an improvement in neuropsychiatric performance over time (12 weeks from the end of treatment), suggesting that viral clearance itself may play a role.14 15 This, however, would not explain the transient neuropsychological and electrophysiological worsening observed in our case series. Side effects such as weakness (30%–59%), headache (20%–30%), irritability (10%–16%) and depression (1%) have been reported in relation to treatment with SOF and may suggest mild neurotoxicity.16 In addition, while studies focusing specifically on the neuropsychiatric side effects of DAAs are lacking, preliminary data indicate, for example, that DAAs confer a minimal risk of additional side effects when taken together with antipsychotic drugs.17 There is a possibility that treatment with ribavirin may have also played a role. Ribavirin has been associated with headache and fatigue,18 and also with mood changes such as anxiety and depression. This case series does not support a role for ribavirin, but power does not allow to reach definite conclusions.
In contrast to patients with cirrhosis, post-LT patients showed no significant variation in their neuropsychiatric performance over time. These differences may be explained by several factors: (1) age, as patients with cirrhosis were significantly older than their transplanted counterparts; (2) blood–brain barrier alterations, which are present in patients with cirrhosis19; (3) the known extreme sensitivity to the neurotoxic effects of both psychoactive and non-psychoactive drugs of patients with cirrhosis20 21; and (4) hepatic metabolism and hypoalbuminaemia,16 which may increase free drug levels. Finally, while the direct neurotoxicity of HCV infection remains debatable,22 23 it may be more likely to translate into a clinical phenotype in patients with cirrhosis rather than in healthier individuals with HCV infection only.
While cognitive impairment has been documented in transplanted patients and attributed to either immunosuppressive therapy24 or to the sequelae of previous liver failure/its aetiology,25 no significant cognitive alterations were detected in post-LT patients in this study at any time point.
In conclusion, we report mild, transient worsening in cognitive and neurophysiological performance in patients with cirrhosis at the end of a course of treatment with SOF-based regimens. Caution/monitoring may be needed in this group, especially if there is a history of overt hepatic encephalopathy and/or any neurological/psychiatric comorbidity. No such changes were observed in a group of younger but otherwise comparable patients treated for post-LT HCV recurrence. Our study has limitations, the main one being its size, which did not allow for subgroup and adjusted analyses. However, the presented results, together with the clinical experience of a small case series, suggest that further research into the neuropsychiatric effects of SOF-based regimens is worthy of further study. In particular, repeated neuropsychological and electrophysiological evaluations during the course of treatment might be of value.
References
Footnotes
Contributors SV: data acquisition/analysis, manuscript drafting. SM: study design, data acquisition/analysis, manuscript drafting. AZ: patient screening/referral, data acquisition. MT: data acquisition/analysis. MDR: data acquisition/analysis. AF: patient screening/referral, data acquisition. PA: study design, draft revision for important intellectual content. GG: patient screening/referral, data acquisition. MS: patient screening/referral, data acquisition. MG: patient screening/referral, data acquisition. FPR: patient screening/referral, data acquisition. PB: study design, draft revision for important intellectual content, responsible for the overall content as guarantor.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study was approved by the Padova University Hospital Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.