Article Text

Abstract
Introduction Squamous cell carcinoma of the oesophagus is a common cancer among South Africans. Due to the absence of effective screening and surveillance programme for early detection and late presentation, squamous cell carcinoma of the oesophagus is usually diagnosed at an advanced stage or when metastasis has already occurred. The 5-year survival is often quoted at 5%–10%, which is poor.
Objectives To determine the association between oesophageal squamous cell carcinoma (OSCC) and non-acid gastro-oesophageal reflux disease.
Study design A cross-sectional case–control analytical study of patients referred to the Gastroenterology Division of Steve Biko Academic Hospital in Pretoria, South Africa. All patients had combined multichannel impedance and pH studies done and interpreted after upper gastroscopy using the American College of Gastroenterology guidelines by two clinicians.
Results Thirty-two patients with OSCC were recruited: non-acid reflux was found in 23 patients (73%), acid reflux in 2 patients (6%) and 7 patients (22%) had normal multichannel impedance and pH studies.
Forty-nine patients matched by age, gender and race were recruited as a control group. Non-acid reflux was found in 11 patients (22%), acid reflux in 31 patients (63%) and 7 patients (14%) had normal multichannel impedance and pH monitoring study.
Conclusion The significance of the association between non-acid reflux and OSCC was tested using χ2, and simple logistic regression was used to adjust for the effects of potential confounders.
The OR of developing OSCC in patients with non-acid gastro-oesophageal reflux was 8.8 (95% CI 3.2 to 24.5, P<0.0001) in this South African group.
Alcohol and smoking had no effect on these results.
- oesophageal squamous cell cancer
- gastroesophageal reflux disease
- pH impedance monitoring
- non-acid gastroesophageal reflux
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- oesophageal squamous cell cancer
- gastroesophageal reflux disease
- pH impedance monitoring
- non-acid gastroesophageal reflux
Summary box
What is already known about this subject?
It is common in South African black men.
It presents too late for curative therapy.
Helicobacter pylori infection is common among patients with SCCE.
What are the new findings?
SCCE is associated with H. pylori infection.
SCCE is associated with extensive gastric atrophy.
Most patients with SCCE have no preceding symptoms of gastro-oesophageal reflux.
Non-acid gastro-oesophageal reflux is associated with the development of SCCE.
How might it impact on clinical practice in the foreseeable future?
Non-acid reflux may be the gateway to how risk factors ultimately lead to the development of SCCE.
Patient with non-acid reflux may need to be treated and followed-up to prevent oesophageal squamous cell carcinoma.
H. pylori, which causes extensive gastric atrophy, will need to be eradicated.
Patients with extensive gastric atrophy will need a surveillance program to identify non-acid reflux and SCCE early.
Literature overview
Gastro-oesophageal reflux is defined as the retrograde flow of gastric contents into the oesophagus. It occurs even in healthy individuals and is regarded as physiological as long as it does not cause oesophageal mucosal damage, symptoms and complications. Gastro-oesophageal reflux is defined as an acid if the pH of the refluxed gastric contents is below 4 and non-acid when it was above 4.
Oesophageal cancer is one of the cancers given the least attention as far as studies are concerned, and yet it is one of the deadliest worldwide.1
Despite recent advances in diagnosis, staging and treatment of this neoplasm, only a small but significant improvement in survival has been achieved.1 Further evaluation is needed if we are to win the war against this cancer.
The lifetime risk of oesophageal squamous cell carcinoma (OSCC) is estimated to be 0.8% for men and 0.3% for women.2 The risk is reported to increase with age, with a mean age at diagnosis of 67–68 years.2–4 Approximately 0.3 of the cases were diagnosed between the ages of 20 and 34 years, 2.3% between 35 and 44 years, 12.2% between 45 and 54 years, 26.1% between 55 and 64 years, 27.4% between 65 and 74 years, 23.7 between 75 and 84 years and 8.0% in 85 years and older.2 It is reported to be more common among black men.2 4 Worldwide, oesophageal cancer is reported to be the sixth leading cause of death from cancer.5 The 5-year survival is often quoted at 5%–10%, which is poor considering the figures above.3 6
Ninety per cent or more of oesophageal cancers are either squamous cell carcinoma or adenocarcinoma with squamous more common in developing countries like South Africa.1 3
The pathogenesis of oesophageal carcinoma remains unclear.1 In most cases, at the time of diagnosis of squamous cell oesophageal carcinoma, 50% or more of patients have either unresectable tumours or radiological demonstrable metastases.1 There is a need to develop strategies that will help prevent this cancer and pick it up early in those where prevention failed.
Several risk factors have been found to be associated with oesophageal cancer:
Tobacco smoking has been found to be associated with an increase of squamous cell carcinoma and adenocarcinoma of the oesophagus.7 8 Carcinogens of tobacco, including nitrosamines, come into direct contact with oesophageal mucosa during smoking.9 The risk of oesophageal cancer is reported to increase with both quantity and duration of smoking.7 8 Tobacco smoking also increases the risk of gastro-oesophageal reflux, which in turn increases the risk of both types of cancers.
A past history of radiotherapy to the mediastinum for the treatment of lymphoma, breast or other cancers is thought to also predispose to both histological types of cancer. Oesophageal cancers are reported to typically develop 10 or more years after exposure to radiation.1 10 The mechanism of how radiotherapy leads to the development of oesophageal cancer is not known, but radiation is a risk factor for many other cancers such as thyroid.
Known etiological risk factors for OSCC
Chronic oesophageal irritation
Any factor that increases oesophageal mucosal irritation appears to increase the risk of developing squamous cell carcinoma of the oesophagus. Included is alcohol and tobacco smoking especially in combination7 8 11–19 and may account for 90% or more of all cases of squamous cell carcinoma of the oesophagus in the developed world.4
Other causes of chronic irritation included achalasia, a well-established risk factor,20–25 and oesophageal diverticula, where food retained in the oesophagus is decomposed by bacteria releasing various chemical irritants.26 27 This retention and fermentation lead to chronic inflammation. Ingestion of lye and other caustic substances is also reported to increase the risk.28
Achalasia is a rare, chronic oesophageal motility disorder estimated to occur in 1 per 100 000 subjects in Western communities.29 The disease occurs at any age, but the incidence is reported to increase with age. The pathology is the inability of the lower oesophageal sphincter to relax, leading to oesophageal dilatation and loss of normal peristalsis of the oesophageal body. These abnormalities lead to oesophageal distension with retention of foods, fluids and bacterial overgrowth resulting in impaired clearance of regurgitated gastric contents. This leads to inflammation of the oesophageal mucosa, dysplasia and ultimately oesophageal cancer.30 31
Genetic predisposition
Several genomes have been identified. Wu et al identified a total of seven susceptibility loci on the following chromosomes, 5q11. 6p21, 10q23,12q24 and 21q22, which suggested the involvement of multiple genetic loci and gene–environment interaction in the development of OSCC.
There are several other polymorphisms that have been studied that showed a suggestive association (P<0.05), which are ADH1B Arg48His (rs1229984), COX-2-1195G>A (rs689466), CASP8 Asp302His (rs1045485) and MGMT Leu84Phe (rs2234767). Haplotype analysis suggested previously that the FAS polymorphism-670A>G (rs1800682) and −1377G>A (rs 2234767) were associated with OSCC in mixed race populations of South Africa (P=0.006 and P=0.004, respectively) and CASP8 (−652 6Ndel:302His) haplotype (P=0.0013).32
This study indicated several instances of population-specific differences in the genetic aetiology of OSCC between the high-risk populations and the two South African populations; this may reflect differences in their Ancestry and environmental exposures.
Non-epidermolytic palmoplantar keratoderma syndrome (tylosis)
This has been found to predispose patients to the development of squamous cell carcinoma of the oesophagus. It is an autosomal-dominant disorder with a genetic abnormality at chromosome 17q25.1 33 In members of affected families, it increases the risk of developing OSCC by up to 95% by the age of 70 years.1 34 There are two types of this condition. Tylosis (type A), which begins in older patients is reported to be associated with high incidence of oesophageal carcinoma, and the early-onset tylosis (type B), which affect younger patients, appears to be a benign disorder.35
Other associated risk factors
Squamous cell carcinoma of the oesophagus is associated with low socioeconomic status.
The Plummer-Vinson syndrome, characterised by dysphagia, iron deficiency anaemia and oesophageal web, is also reported to be associated with squamous cell carcinoma of the oesophagus.36
Extensive gastric atrophy
A large number of squamous cell carcinoma of the oesophagus develops without the above risk factors, indicating that there could be other factors for the development of OSCC. A study conducted in Sweden demonstrated that serological gastric atrophy induced by Helicobacter pylori infection may increase the risk of developing squamous cell carcinoma of the oesophagus.11
The same authors reported elsewhere that the risk of OSCC was significantly increased in a cohort of patients with pernicious anaemia, who have type A atrophic gastritis.11
Extensive gastric atrophy was found to be a risk factor for OSCC in Japan.11 Similar results were found in Finland. These observations suggest that extensive gastric atrophy is associated with OSCC in Sweden, Japan and Finland.37 38 These findings need to be confirmed among other different ethnic groups.
In our study from South Africa, histological extensive gastric atrophy was found in only 25% of patients with OSCC, which is less than half of that found in Sweden and Japan, suggesting that it may not be a significant factor in our region.39
Helicobacter pylori
H. pylori infection is an important causative factor in gastric carcinogenesis, and its role in extragastric gastrointestinal cancers is controversial. In a case–control study, Uno et al40found that H. pylori infection had an opposite association with oesophageal adenocarcinoma and oesophageal gastric junction adenocarcinoma but had a direct association with OSCC. de Vries et al41reported that H. pylori infection increased the risk of developing squamous cell carcinoma of the oesophagus by a factor of 2.1. Nie et al found no association between oesophageal cancers and H. pylori cytotoxin-associated gene A (Cag A)-positive strains. They concluded that Cag A-positive strains may have a positive association with OSCC in populations of non-Asian origin and an inverse association in Asian population.42 43 Xie et al44 looking at H. pylori infection and oesophageal cancer risk, concluded that H. pylori infection is associated with an increased risk of OSCC in Eastern population and a decreased risk of oesophageal adenocarcinoma in the overall population. Islami and Ramanga found no overall association between H. pylori and OSCC risk. They, however, found a statistically significant association between H. pylori and OSCC in Western studies, with an OR (95% CI) of 1.65 (1.17 to 2.32).45 When they classified studies by geographic region, there was a statistically significant association between H. pylori and OSCC in Western studies, with an OR (95% CI) of 1.65 (1.17 to 2.32).45 Kgomo et al46 in their study in Iran concluded that H. pylori infection decreases the risk of OSCC and that this is not related to a Cag A-positive status. In a study performed in South Africa, we found that H. pylori infection was associated with an increased risk of developing OSCC with (CI 95%) OR of 2.4.47
There are not enough studies evaluating the relationship between gastro-oesophageal reflux of non-acid type and advanced OSCC published so far, and a small Japanese study of 14 patients with early OSCC suggested a causal relationship.40
Aims and objectives
Primary objectives
To determine whether non-acid gastro-oesophageal reflux is associated with OSCC in a large cohort of patients in South Africa.
Methods
Study design
This is a cross-sectional case–control analytical study of patients referred to the Gastroenterology Division of Steve Biko Academic hospital in Pretoria.
Patient’s smoking and alcohol history was recorded.
Those patients with obstruction of the oesophagus due to cancer was relieved by dilatation, stenting and biopsy of the antrum and corpus were send for H. pylori and extensive gastric atrophy, and a prevalence of 25% was found, previously published.39 46 Those who needed stents inserted were excluded from having multichannel impedance testing.
Patients had combined intraluminal multichannel impedance and pH studies done and interpreted after upper gastroscopy, according to the American College of Gastroenterology guidelines.47
Statistical consideration
This study aims to primarily determine the association of non-acid GER and OSCC in the high-risk Black South African male patient population referred to the Gastroenterology Department at Steve Biko Academic Hospital.
Inclusion criteria
All patients who are 18 years and older referred to the Gastroenterology Department at Steve Biko Academic Hospital for gastroscopy.
Patients with histologically confirmed squamous cell carcinoma of the oesophagus.
Patients who were in a good clinical condition to withstand gastroscopy.
Patients with OSCC who had adequate oesophageal patency.
Exclusions
The following group of patients was excluded:
Associated achalasia as demonstrated by motility studies.
Those in whom histology of the oesophagus also showed human papilloma virus.
Patients with a history of caustic fluid ingestion.
Patients with a history of proton pump inhibitor usage in the last 4 weeks.
Patients with a history of use of antihistamines in the last 2 weeks.
Patients with a history of antibiotic use in the last 2 weeks.
Patients with associated gastric adenocarcinoma.
Patients who had prior radiation therapy.
Patients with cancer lesion in the lower third of the oesophagus.
Patients with oesophageal stents.
Pregnant patients.
Patients who previously had two or more oesophageal dilatations.
Control group
Forty-nine patients of comparable age, race and sex patients with no oesophageal cancer referred to Gastroenterology division for upper gastrointestinal endoscopy for dyspeptic or other benign symptoms were recruited. These were patients attending our clinic for dyspepsia who were enrolled after stopping their proton pump inhibitors for 1 month, those referred for investigation of iron deficiency anaemia and patients referred for screening or surveillance. The upper endoscopy was done as part of the management of the patient’s disease they are referred for, and not for study purposes. The 24-hour multichannel impedance and pH monitoring were done for study purposes for which their consent was sought.
It was made clear to them that some of these procedures are merely for research and may not necessarily benefit them at this point, but lesions detected at endoscopy and biopsy thus received standard therapy.
Multichannel impedance and pH studies
Using digi-trapper high-definition multichannel impedance and pH medical measurement system, a test catheter with multiple sensors (high definition) was passed through the nose into the lower oesophagus. Lower oesophageal sphincter was identified by high pressures on manometry. A chest radiograph was done to confirm the position of the catheter in those in whom manometry failed to identify the lower oesophageal sphincter position. The bottom sensor was placed 5 cm above the oesophogogastric junction. Patients were then advised to continue with their usual daily activities, including eating and drinking as normal for 24 hours. The monitor was then retrieved after 24 hours of recording. Those in whom recording was interrupted or faulty were excluded.
Results
Results were read using the table of normal values from the American guidelines, as shown in table 1.
Table of normal values for oesophageal multichannel and pH monitoring47
A cut-off threshold total of 4.0%, recumbent of 2% and upright of 6.3% was used. Symptom index was not used as it would not work in patients with cancer. Eighty-one patients were recruited, most of whom were in-hospital patients with different non-cancer illnesses because of the 24 hours needed to complete this test and lack of transport. They consisted of 49 controls and 32 study patients with histologically confirmed squamous cell carcinoma of the oesophagus. There were 9 women (28%) and 23 men (72%) in the cancer group, and 36 men (73%) and 13 women (27%) in the control group. The racial distribution was 30 black patients (94%) and 2 white patients (6%) in the cancer group and 42 black patients (86%) and 7 white patients (14%) in the control group. The mean age for cancer group was 61.7+−5.3 and 54.3+–5.1 for control group, as shown in table 2.
Demography
Reflux episodes consisted of liquid, gas and mixed types in both groups.
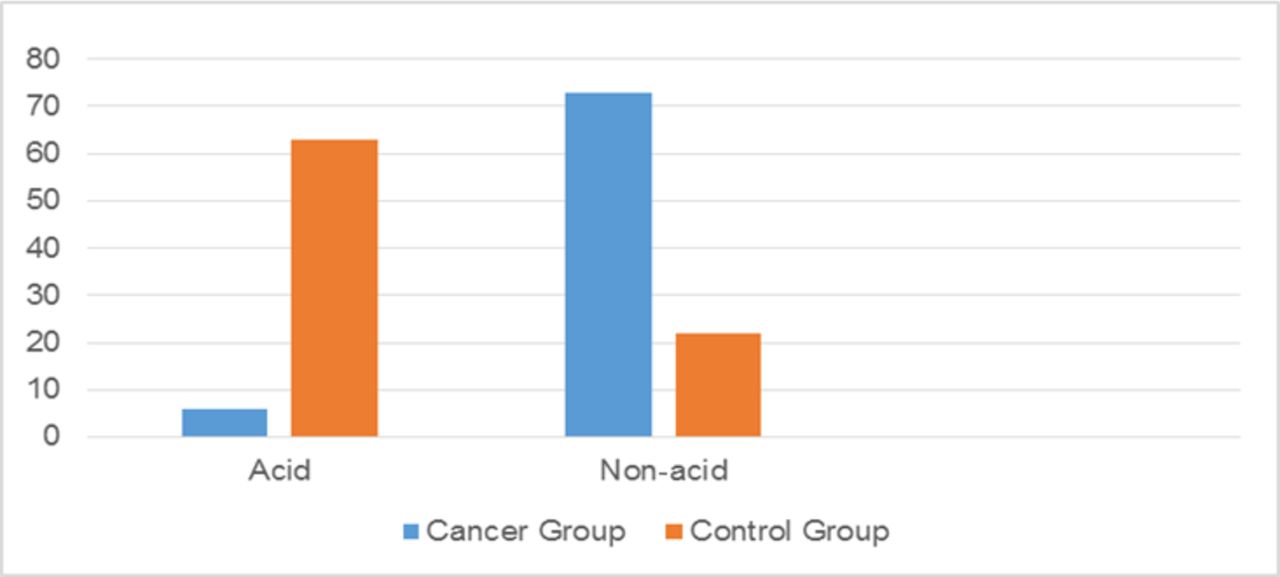
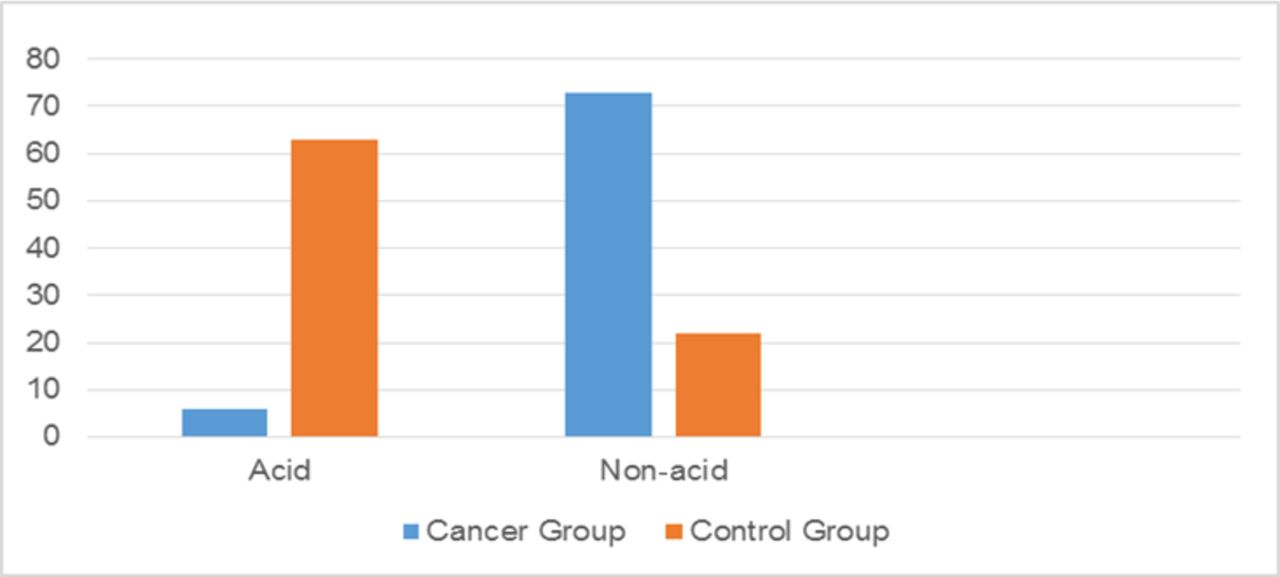
Thirty-two patients with histologically proven OSCC were recruited. Non-acid gastro-oesophageal reflux was found in 23 patients (73%), acid reflux was found in 2 patients (6%) and 7 patients (22%) had normal combined intraluminal multichannel impedance and pH studies.
Forty-nine patients were recruited as a control group, and non-acid reflux was found in 11 patients (22%), acid reflux was found in 31 patients (63%) and 7 (14%) patients had normal multichannel impedance and pH monitoring study, as shown in table 3 and figure 1.
Results of multichannel impedance and pH monitoring
{kind=link}
Combined multichannel impedence and pH monitoring.
Reflux episodes consisted of both liquid and mixed types in both groups. Non-acid was defined as pH above 4 and acid pH below 4. The number of non-acid reflux in patient with cancer ranged from 11 to 47 episodes in a 24-hour period.
Statistical analysis
The significance of the association between acid or non-acid gastro-oesophageal reflux and oesophageal cancer was tested using χ2 test, and simple logistic regression was used to adjust for the effects of potential confounders.
Non-acid gastro-oesophageal reflux had OR 8.8 (95% CI 3.2 to 24.5) P<0.0001, and acid reflux had OR 0.04 (95% CI 0.009 to 0.189) P<0.0001. This study suggests that achlohydria may play a role, but we failed to demonstrate extensive gastric atrophy to explain this occurrence shown in our previous publication.41
Smoking and alcohol had no effects on these results.
Conclusion
In this group of patients with OSCC, OSCC was associated with non-acid gastro-oesophageal reflux. The OR of 8.8 (95% CI 3.2 to 24.5) with a significant P value of <0.0001 implies a relative risk increase of 140%. This study confirms it to be a disease of black middle-aged to elderly patients. H. pylori infection has an additive role to this association, but extensive gastric atrophy played no significant role as we found the histological prevalence of only 25% in our patients with cancer.39. This study suggests that we should attempt to develop more effective and universal antireflux therapy that will prevent all types of reflux, as any type of reflux leads to one or the other form of oesophageal cancer in the long run.
Discussion
This study confirms the association of non-acid reflux and squamous cell carcinoma in the oesophagus. Acid reflux is a known risk factor for the development of Barrett’s oesophagus and adenocarcinoma of the oesophagus. Therefore, any type of reflux needs to be prevented.
The development of squamous cell carcinoma of the oesophagus is a complicated process, in that genetic factors differ even in the same ethnic groups including different South African populations. Environmental factors are also different in different parts of the world where squamous cell carcinoma of the oesophagus is common and yet its presentation is the same. Non-acid reflux may be the point where all these factors converge to lead to OSCC development. Non-acid gastro-oesophageal reflux may, therefore, be the important point of intervention for stopping the development of OSCC as it seems to be the point of conversion for all other risk factors leading to the development of OSCC in South African population.
It is important that studies evaluating the relationship between non-acid gastro-oesophageal reflux and OSCC be performed in other population groups to confirm this relationship, as this may be an important point of intervention.
To our knowledge, this is the largest and only study conducted in patients with squamous cell carcinoma of the oesophagus in the world. The only other study previously conducted was performed in Japan with a small a group of patients with early OSCC.
References
Footnotes
Contributors MK was involved in conception of the study, write up, conduction of the study and collation of results. TRM was involved in conception and write up of this paper. JAK was involved in conception and write up.
Competing interests None declared.
Ethics approval University of Pretoria Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.