Article Text

Abstract
Background The British Society of Gastroenterology guidelines recommend taking at least four duodenal biopsy specimens at the time of upper gastrointestinal (UGI) endoscopy if coeliac disease (CD) is suspected and it has been shown to increase the diagnostic yield of CD. We assessed the compliance to these guidelines within our institution. We then applied measures to improve our compliance rate and assessed the resulting impact on our diagnostic rate of CD.
Methods We performed a retrospective audit of electronic records for all patients, with no prior diagnosis of CD, who underwent UGI endoscopy with duodenal biopsies between August 2014 and May 2015. We implemented measures to raise awareness among endoscopy users at our institution and carried out a reaudit between February and May 2016.
Results 924 patients were found to be eligible in the first part of the study and 278 in the second part. The proportion of patients who had ≥4 biopsy specimens submitted increased from 21.9% to 60.8% (p<0.001). The diagnostic rate of CD increased from 3.5% in the audit group to 7.6% in the reaudit group (p=0.004). A positive serology result and suspected CD as an indication for biopsy were found to be independent predictors of the likelihood of complying with guidelines.
Conclusions Our study suggests that taking <4 duodenal biopsy specimens to assess for the presence of CD may lead to the diagnosis of CD being missed. Simple measures can improve the local compliance rate to current guidelines.
- COELIAC DISEASE
- ENDOSCOPY
- DUODENAL MUCOSA
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
▸ Mucosal changes can be patchy in coeliac disease (CD).
▸ The British Society of Gastroenterology (BSG) recommends taking at least four biopsy specimens if CD is suspected at the time of endoscopy.
▸ Previous studies have shown that this increases the diagnostic rate of CD.
▸ Despite existence of clear BSG guidance, compliance to this is quite poor in our unit, which may reflect a more widespread problem.
▸ This may be due to a lack of awareness of guidelines, or other barriers.
▸ Simple interventional measures may help to improve compliance and potentially improve the diagnostic rate of CD.
▸ Our results should prompt other units to audit their practice and implement measures to improve adherence to current recommendations, and thus the care of patients with potential CD.
Introduction
Coeliac disease (CD) is a common condition with a prevalence of at least 1% in the UK.1 CD can present with a range of symptoms including vague and non-specific abdominal symptoms similar to irritable bowel syndrome.2 With time, the proportion of patients presenting with atypical symptoms has also increased.3 Thus, it is important to ensure that when CD is considered as a potential diagnosis, patients are adequately investigated to avoid missing the diagnosis. The lifetime risk of malignancy, especially intestinal lymphoma and other gastrointestinal cancers, in fact, slightly increased in CD4 with studies quoting an incidence of lymphoma of 8%.5
Endoscopy remains the mainstay of adult CD diagnosis. As histological changes in CD can be patchy, several biopsies should be taken from the bulb and more distal duodenum at the time of endoscopy. Updated guidelines from the British Society of Gastroenterology (BSG) on the management of adult CD recommend taking at least four duodenal biopsies, including one from the bulb, if CD is suspected.6 This is based on a large study involving 132 352 patients without known CD, which showed that taking ≥4 duodenal biopsy samples resulted in a doubling of the diagnostic rate of CD compared with when <4 samples were taken.7 This is further supported by evidence from a retrospective study involving patients with known CD, which showed that the sensitivity for a diagnosis of CD increased with incremental biopsies, and the diagnosis could be confirmed in 100% of patients when four biopsy specimens were taken.8
We carried out a study to assess our compliance to the BSG guidelines in patients without known CD. Following implementation of measures to improve compliance, we also aimed to determine the influence of better compliance to guidelines on our local diagnostic rate of CD.
Methods
A list of all patients who had endoscopic duodenal biopsies submitted for histopathological analysis to the Barnsley General Hospital NHS Foundation Trust (UK) pathology laboratory over a 10-month period from August 2014 to May 2015 was retrieved from the laboratory database using coding. For each set of specimens submitted, the date of specimen collection, the clinician performing the biopsy, and patient age and sex were also available. Using the Integrated Clinical Environment (ICE—the online system for pathology reporting), we obtained information on the main indication for biopsy, the number of biopsy samples for each specimen, histopathology report and results of IgA anti-tTG antibody tests if performed (as this is the most widely available serology test for CD screening locally especially in primary care).
We presented the results of this first part of our study at the local Endoscopy User Group meeting in November 2015. This meeting is attended by endoscopists in the trust who have regular endoscopy lists and therefore perform the majority of endoscopies in the unit, as well as endoscopy nurses. While most of these clinicians were present, a number did not attend. We therefore also put up posters summarising the results of our findings in all clinical areas within the endoscopy unit to raise awareness of the importance of complying with guidelines among endoscopists and to encourage and remind them to take the appropriate number of biopsies. We then collected data using the same methods described above for duodenal biopsies submitted for histopathological analysis over a 3-month period from February 2016 to May 2016.
As clinical records were not accessed, for the purpose of this study CD was defined as:
either histological Marsh grades IIIa, IIIb or IIIc (as defined by the Modified Marsh classification);
Marsh grades I or II or a report of increased intraepithelial lymphocytosis in conjunction with a positive serology result (anti-tTG antibody positive).
These definitions are based on the algorithm for the diagnosis of CD laid out in the BSG guidelines.6 In our institution, an IgA-tTG antibody level of 10U/mL is regarded as definitely positive. Values of exactly 10U/mL or just under 10U/mL are reported as either weakly positive or equivocal—we have regarded these as negative results for the purpose of our study.
The study was registered with and approved by the trust audit department, which did not deem local research and development approval necessary due to the study being purely an audit.
Exclusion criteria
Patients with known CD, having duodenal biopsies for follow-up, were excluded. We also excluded records where the number of biopsy specimens was not specified (described as ‘several’ or ‘multiple’). For patients having more than one endoscopy examination with duodenal biopsies during one study period, we only considered the first endoscopy. Duodenal bulb specimens (when taken and specified in the histopathology report) were included in the total count of number of duodenal specimens submitted.
Statistical analysis
The χ2 test was used to compare categorical variables and the independent t-test to compare means of numerical variables between the audit and reaudit groups. We also used the χ2 test to assess the impact of compliance to BSG guidelines on the proportion of patients diagnosed with CD (as per criteria defined above). We used a generalised estimating equation (GEE) to identify factors predicting adherence to guidance, while adjusting for clustering by endoscopist. All p values are 2-sided. The IBM SPSS (V.24) software was used for all statistical analyses.
Results
A total of 973 endoscopies with duodenal biopsies were performed from August 2014 to May 2015. Of these, 924 endoscopies were included in the study after applying exclusion criteria. The respective figures for the reaudit from February 2016 to May 2016 were 290 and 278. Table 1 shows the characteristics of patients included in the study. There were no significant differences between groups in terms of patient demographics and indication for biopsy. These 1263 endoscopies with duodenal biopsies performed across the two study periods (before applying exclusion criteria) represent 27.5% of the total number of upper gastrointestinal endoscopies performed in our institution.
Characteristics of patients, without known coeliac disease, undergoing endoscopy and duodenal biopsies
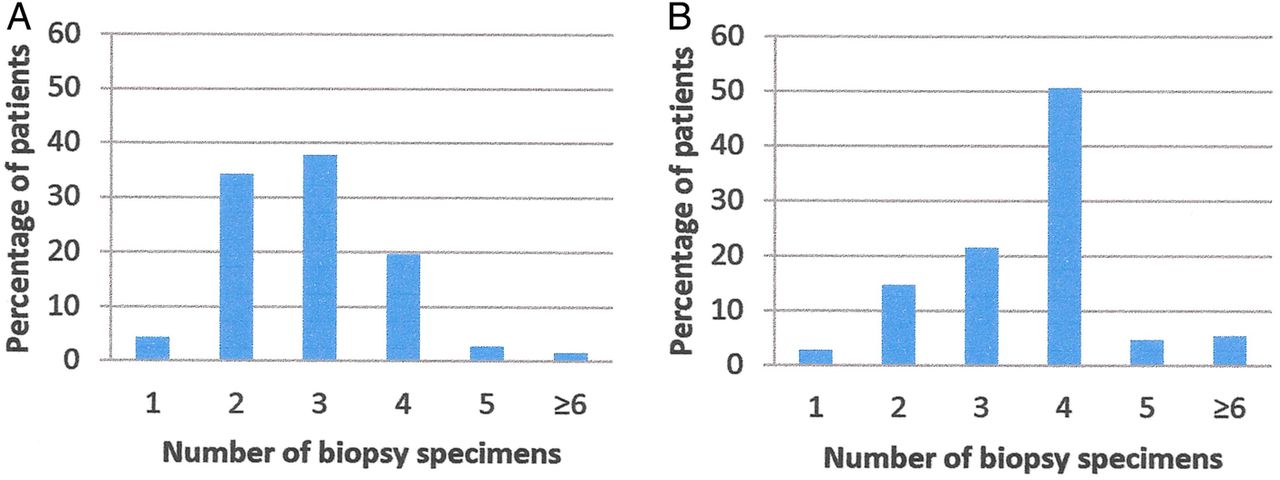
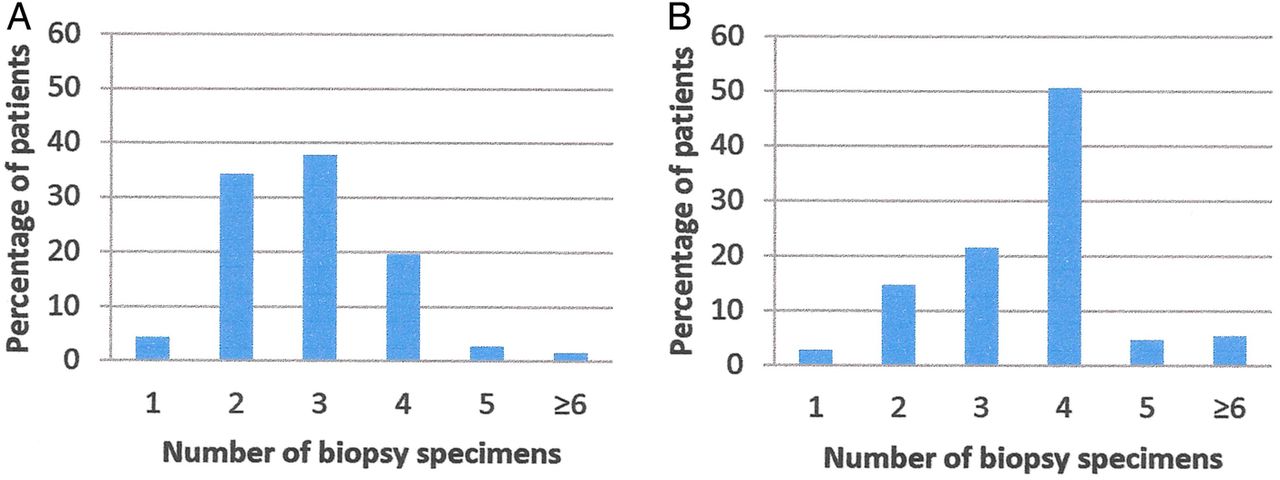
In the first part of the study, ≥4 biopsy specimens were submitted for histopathological analysis in 21.9% of cases (n=219). This increased to 60.8% (n=169) in the reaudit following implementation of interventional measures (p<0.001). Even when ‘suspected coeliac disease/malabsorption’ was the indication for biopsy, 39.2% (n=47) of patients had ≥4 biopsies taken in the first study period, but the corresponding figure was 60.0% (n=18) in the reaudit (p=0.039). The modal number of specimens submitted also changed from 3 to 4 (figure 1A,B).
{kind=link}
Bar charts of number of duodenal biopsies submitted for histopathological analysis for patients having an endoscopy and duodenal biopsies between (A) August 2014 and May 2015 and (B) February 2016 and May 2016.
Thirty-two patients were found to have CD in the first cohort and 21 in the second (3.5% vs 7.6%, p=0.004). In both groups of study, before and after intervention, the diagnostic yield of CD when ≥4 biopsies were taken was higher than when <4 biopsies were taken. The diagnostic rate of CD in the audit group was 2.0% (14 patients out of 705) when <4 biopsies were taken and 8.2% (18 out of 219 patients) when >4 biopsies were taken (p<0.001). The respective figures were 3.7% increasing to 10.1% with ≥4 biopsies in the reaudit group (p=0.049). The results from both parts of the study are summarised in table 2.
Differences between audit and reaudit groups in terms of number of biopsy specimens submitted for histopathological analysis and diagnostic rate of coeliac disease
A total of 42 different clinicians performed endoscopies with duodenal biopsies in the 1202 patients (audit and reaudit groups combined). Eighteen of these clinicians performed at least 10 endoscopies, with the remaining 24 performing fewer than 10 endoscopies over the study periods considered. Between these 18 clinicians, a total of 1133 endoscopies were performed (ie, 94% of the overall number of endoscopies performed). Their overall compliance with guidelines varied from 12% to 67% (SD 11.9%).
We therefore identified factors predicting overall adherence to BSG guidelines (ie, submission of ≥4 biopsy specimens), while adjusting for clustering by clinician, using GEE. The following parameters were assessed as predictors of taking ≥4 biopsies: study group (audit vs reaudit), age, sex, indication for biopsy and serology test result (positive or negative).
The reaudit group was associated with a significantly increased odds of taking four or more biopsies compared with the audit group (OR 5.3; 95% CI 3.8 to 7.5; p<0.001). Suspected CD as an indication for biopsy also had a higher odds of adhering to guidance (OR 2.45; 95% CI 1.01 to 6.17; p <0.05), while the lack of a positive anti-tTG antibody result was associated with decreased odds of compliance (OR 0.39; 95% CI 0.21 to 0.73; p=0.003). The remaining factors considered did not reach statistical significance.
Discussion
Only a quarter of upper gastrointestinal endoscopies performed in our institution result in duodenal biopsies, which reinforces the fact that, when taken, the main aim probably remains to diagnose or exclude CD. The results of our initial audit thus demonstrate poor adherence to established national recommendations in patients with no known diagnosis of CD, in whom this diagnosis is being considered at endoscopy. This remained suboptimal even when the clinical indication for biopsies was ‘suspected coeliac disease’. Although compliance only reached 60.8% in the reaudit, we have been able to demonstrate that simple interventional measures to raise awareness among endoscopists can be successful in significantly improving compliance to guidance. Potential barriers to adherence, as previously suggested in the literature7 include lack of awareness among clinicians of these guidelines and the extra time required to take a larger number of samples due to multiple passes of the biopsy forceps.
Of the 18 endoscopists who performed the majority of endoscopies during our study periods, only nine were present at the Endoscopy User Group meeting (November 2015) where we presented the results of our audit and encouraged endoscopists to comply with guidelines. Furthermore, a number of clinicians performing endoscopies in our trust are nor regular trust clinicians, but rather are from external agencies. Thus, reasons for failing to reach a higher rate of compliance in our postintervention group may include the fact that the recommendations from our initial study were not taken up by all clinicians involved, and potentially our message did not get across to everyone. The next stage of our study involves a more targeted training approach, to also include endoscopy nurses who are in a position to request clinicians to take an adequate number of biopsies. A formal assessment of individual clinicians' perceptions through questionnaires may further clarify barriers to compliance, and potentially help us to improve it further.
The diagnostic rate of CD doubled following implementation of changes (7.6% in the reaudit vs 3.5% in the audit). There were no statistically significant differences between the audit and reaudit groups in terms of baseline characteristics, hence why we postulate that the higher probability of diagnosing CD in the reaudit group is likely attributable to the higher proportion of patients having ≥4 biopsies taken. In fact, within each group there was a significant increase in the probability of a CD diagnosis when patients with <4 biopsy specimens were compared with those with ≥4 specimens. Lebowhl et al7 also reported a doubling of the diagnostic rate of CD when four or more specimens are submitted for histology.
This raises the question of whether new diagnoses of CD are being missed due to inadequate number of biopsies submitted. CD is believed to be largely underdiagnosed.9 A number of reasons for this have been suggested in the literature including the patchy nature of mucosal changes in CD, yield of biopsy samples that are inadequate for histological analysis and variability in histopathology reporting.10–12 Our results and those of similar studies7 ,8 strongly favour the submission of an adequate number of duodenal biopsies for histopathological analysis when a diagnosis of CD is considered.
The GEE analysis confirmed that while adjusting for clustering by endoscopists, the odds of compliance to guidelines still significantly increased in our reaudit cohort. We found that a positive serology result and ‘suspected coeliac disease’ as the principal indication for biopsy to be independent predictors of the likelihood of adhering to guidelines. In their study with a larger sample size, Lebowhl et al7 also found increasing age to be associated with decreased odds of submitting for biopsy specimens.
Limitations
Our study was retrospective and performed using electronic records. With the lack of information regarding clinical CD diagnosis, we formulated definitions of CD based on histology and serology. We did not have complete data on gross endoscopic findings, which are inconsistently documented by endoscopists; these would be best collected in a prospective design. Our reaudit sample size is also relatively small, and our study limited to a single centre. We have not quantified the exact effect that our intervention has had on improving compliance. However, all other factors have remained constant across the two periods of study—see table 1—therefore allowing us to conclude that our intervention at least partly explains the improvement. We do aim to carry out more focused training and qualitatively measure its effect on clinicians' practice before carrying out a further reaudit.
Conclusion
Despite these limitations, our results are in line with previous studies. Our study has reiterated the fact that adherence to BSG recommendations on the number of duodenal biopsies taken at endoscopy when CD is suspected does improve the diagnostic yield of CD. Simple measures to increase awareness of this issue can improve local compliance, with a potential improved detection of CD. We also highlight the fact that despite the existence of the BSG guidelines, overall compliance remains quite poor at our centre, which may affect the diagnosis of CD. Our results should prompt other centres to assess their practice.
References
Footnotes
Acknowledgements We thank audit department, Barnsley Hospital; Rachael Sanderson, Lead Nurse Endoscopy, Barnsley Hospital; Christopher Barton, Clinical Effectiveness Assistant, Barnsley Hospital.
Contributors NH was involved in conception and design; acquisition, analysis and interpretation of the data; drafting of the article; critical revision of the article for important intellectual content; final approval of the article; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. WA was involved in conception and design; acquisition of data; critical revision of the article for important intellectual content; final approval of the article; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MHS was involved in conception and design; critical revision of the article for important intellectual content; final approval of the article; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MHS is responsible for overall content as guarantor.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.