Article Text

Abstract
Background Corticosteroids are a potential risk factor for mortality in patients with perforated diverticular disease, due to blinding of disease severity, hampered wound healing or adrenal insufficiency. We examined mortality in corticosteroid users and non-users among patients with perforated diverticular disease.
Methods A cohort study based on medical databases including all patients ≥18 years in Denmark (source population 5 289 261 inhabitants) admitted to a hospital with incident perforated diverticular disease between 2005 and 2013. 7-day, 1-month, 3-month and 1-year mortality risks in corticosteroid users and non-users were calculated using the Kaplan–Meier method, and compared with Cox proportional hazard regression adjusted for age, sex and comorbidities.
Results The study included 4640 patients with perforated diverticular disease. Of these, 3743 (80.7%) had not used corticosteroids in the year before admission and 725 (15.6%) had been exposed to systemic corticosteroid treatment. The remaining 172 patients had been exposed to either inhaled or intestinal acting corticosteroid therapy. Mortality risk in non-users was 4.4% after 7 days and 15.6% after 1 year. This risk was doubled for corticosteroid users who filled their last prescription during the 90 days before admission, with mortality risks ranging from 14.2% after 7 days to 47.6% after 1 year. 1-year mortality risk was even higher for corticosteroid users with a first filled prescription ≤90 days before admission: 52.5%.
Conclusions Corticosteroid use was associated with clearly increased mortality risk after perforated diverticular disease. Thus, use of corticosteroids should be regarded as an important clinical prognostic factor for mortality in patients with this condition.
- DIVERTICULAR DISEASE
- ADVERSE DRUG REACTIONS
- ENDOCRINE HORMONES
- EPIDEMIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Perforation is a well-known complication of diverticulitis.
The incidence of perforated diverticular disease is ∼4 per 100 000 persons each year.
Mortality risk after perforated diverticular disease requiring operative intervention has been reported to be 12–36% in small cohort studies.
Use of corticosteroids is a potential risk factor affecting mortality in patients with perforated diverticular disease.
What are the new findings?
Mortality risk was twice as high for current corticosteroids users compared with non-users.
This is the first large cohort study comparing mortality risks between corticosteroid users and non-users among patients with perforated diverticular disease. We found that corticosteroid use is a strong indicator for 1-year mortality, with an absolute risk of about 50%.
Our study did not indicate a relation between corticosteroid dose and mortality risk.
How might it impact on clinical practice in the foreseeable future?
Use of systemic corticosteroids should be regarded as an important risk marker for mortality in patients with perforated diverticular disease. Further multiangled evidence is needed to determine whether the association between corticosteroid use and mortality risk is causal.
Introduction
In Western countries, the prevalence of colonic diverticular disease reaches 50% among persons aged 60 and older.1 ,2 Although most patients remain asymptomatic, the lifetime risk for developing diverticulitis is ∼10–25%,3 which is known to present with perforation.4 ,5 The incidence of perforated diverticular disease is ∼4 per 100 000 persons each year, reported in hospital records in the UK of Great Britain and Northern Ireland and the USA.6 Mortality after perforated diverticular disease requiring operative intervention has been reported to be as high as 12–36% in small cohort studies (78–121 cases).7 ,8 Given this high mortality risk, a better understanding of prognostic factors associated with mortality is clearly needed.
Use of corticosteroids is a potential prognostic factor affecting mortality in patients with perforated diverticular disease. Corticosteroids are widely prescribed for inflammatory diseases, malignancies and after organ transplantation, in order to inhibit an inflammatory response.9–11 At the same time, corticosteroids have been associated with bowel perforation in patients with diverticular disease. Three case–control studies reported increased ORs of 1.7 to 28.3 and one cohort study reported a relative risk of 2.2.12–15 A recent meta-analysis showed ORs for perforation of diverticular disease after use of corticosteroids of 2.17 to 31.90.16
There are several reasons why mortality may be increased in patients with perforated diverticular disease who use corticosteroids. Disease severity might be masked by use of corticosteroids,17 leading to incorrect staging of disease severity and, consequently, inadequate treatment.6 Corticosteroid use might hamper wound healing as well through its anti-inflammatory effects, by suppressing cellular wound responses and by inducing diabetes, and thus increasing the risk of wound infection.18 A systematic review also showed that corticosteroid use may increase the risk of anastomotic leakage after colorectal surgery.19 Use of corticosteroids is associated with an increased risk of venous thromboembolism.20 In perforated diverticulitis, undiagnosed and untreated adrenal insufficiency may lead to an Addisonian crisis, which increases mortality risk in affected patients.21
Study aims
The primary aim of this study was to examine absolute mortality risks and compare 7-day, 1-month, 3-month and 1-year mortality rates in patients with perforated diverticular disease who were corticosteroid users versus non-users. The secondary aim was to examine mortality rates in patients with perforated diverticular disease who used corticosteroids administered in different forms and with different cumulative doses.
Methods
Source population
The source population for this study was the entire population of Denmark (5 289 261 inhabitants) between 2005 and 2013. The study period began in 2005 because a full record of medications sold at community pharmacies and hospital-based outpatient pharmacies became available starting in 2004 in the National Health Service Prescription Database.22 The study was based on data from the Danish National Patient Registry, which has recorded all acute care hospital discharges since 1977 and all outpatient specialist clinic and emergency room visits since 1995.23 Data from the Danish Civil Registration System were used to determine vital status.24
Study population and follow-up
The study included all adult patients (≥18 years), with and without use of corticosteroids, hospitalised with incident perforated diverticular disease between 2005 and 2013. Identification of perforated and non-perforated diverticular disease was based on International Classification of Diseases (ICD) codes (see online supplementary appendix 1 for specification of the codes). The codes used for perforated diverticular disease have a positive predictive value ranging from 0.73 to 0.75.25 There were no restrictions in corticosteroid dose or treatment duration. Patients diagnosed during an emergency room visit were excluded because of the low predictive value of emergency room diagnoses; diagnostic accuracy improves with more extensive diagnostic procedures.26 The year 2005 as start of follow-up was chosen in order to provide a 1-year prediagnosis period in which exposure to corticosteroids could be assessed similarly in all patients. Patient follow-up began on the hospital admission date for perforated diverticular disease and ended on death, emigration or end of follow-up on 30 November 2013, whichever came first.
supplementary data
Classification of corticosteroid use and surgical procedures
Corticosteroid use was categorised as follows, based on the National Health Service Prescription Database:22
I. Non-users: patients not prescribed corticosteroids during the year prior to hospital admission.
II. Current users: patients using corticosteroids at time of admission, that is, the last prescription for corticosteroids was filled during the 90 days before admission. The group of current users was subdivided into new users, defined as patients who filled their first prescription ≤90 days before admission, and chronic users, which included all other current users.
III. Recent users: patients who used corticosteroids until shortly before admission, that is, their last corticosteroid prescription was filled between 91 and 365 days before admission.
Analyses were performed separately for patients using systemic corticosteroids regardless of use of other forms of corticosteroids, for patients using systemic corticosteroids only, for patients using inhaled corticosteroids only, and for patients using intestinal acting corticosteroids only. There was one patient using both inhaled and intestinal acting corticosteroids.
The analysis of cumulative dose was based on categorising the 1-year cumulative dose of systemic corticosteroids among current users, calculated using prednisone dose equivalents. The cumulative dose cut-offs were ≤625, >625 to 2000, >2000 to 3500 and >3500 mg, to provide four groups of approximately equal size.
Surgical procedures related to diverticular perforation (including a 30-day period around date of admission for diverticular disease) were categorised as explorative surgery including lavage; stoma with or without resection; and resections with primary anastomosis (see online supplementary appendix 2 for surgical codes).
Statistical analysis
Descriptive contingency tables were prepared, showing demographic characteristics and medical history (age, sex, calendar year of perforated diverticular disease diagnosis, comorbidities) of corticosteroid users and non-users.
For time-to-event analyses, the Kaplan-Meier method and Cox regression were used. Absolute mortality risks in corticosteroid users and non-users were calculated using the Kaplan-Meier method. Cox proportional hazard regression was used to compare mortality rates among the predefined categories of corticosteroid users, providing HRs for 7-day, 1-month, 3-month and 1-year mortality. Stratified analyses were performed according to type of surgery within 30 days before or after diagnosis of perforated diverticular disease.
Subgroup analyses were performed to compare mortality risks among patients taking different forms of corticosteroids (inhaled only, intestinal only and systemic only) and with different 1-year cumulative doses of systemic corticosteroid use. Also, sensitivity analyses were performed after excluding patients with malignancies, patients with inflammatory bowel disease, patients with a previous code for diverticular disease and patients with rheumatic diseases including mixed connective tissue disease.
In addition to crude analyses, we performed adjusted analyses including the following potential confounders: age, sex, use of cardiovascular medications (anticoagulants, non-steroidal anti-inflammatory drugs, ACE/angiotensin 2 receptor (A2R) inhibitors, statins, β blockers, calcium channel blockers, diuretics, selective serotonin reuptake inhibitors (SSRIs) and nitrates)16 during the 90 days before admission, hypertension, chronic obstructive pulmonary disease (COPD; as a proxy for smoking), liver disease or chronic pancreatitis, alcoholism-related diseases other than those affecting the liver or pancreas, inflammatory bowel disease, rheumatoid arthritis, connective tissue disease, malignancies and modified Charlson Comorbidity Index score (see online supplementary appendix 1 for specification of the codes). The modified Charlson Comorbidity Index score was calculated after exclusion of COPD, liver diseases, connective tissue disease and malignancies. These characteristics and conditions are associated with corticosteroid use and constitute potential risk factors for mortality.
We used SAS V.9.2 (SAS Institute, Cary, North Carolina, USA) for our statistical analyses. Permission from the Danish Data Protection Board was granted.
Results
Study population
A total of 4640 patients with perforated diverticular disease were included in the study. Of these, 3743 (80.7%) had not used corticosteroids in the year before hospital admission (table 1). Of the 897 patients using corticosteroids in the prior year, 725 (80.8%) were exposed to systemic corticosteroid treatment (current and recent users combined). Of systemic corticosteroid users, 88.8% used prednisone or prednisolone, 6.9% methylprednisolone, 13.4% β-methasone, 1.5% triamcinolone and 1.0% hydrocortisone. Since the number of patients using only intestinal acting corticosteroids was small (n=28), this patient group was not analysed further. Corticosteroid users were on average older than non-users and more often female than non-users (64.8% vs 54.2%). Patients using systemic corticosteroids were more often hypertensive, more often had COPD, chronic bronchitis, emphysema or asthma, and more often had malignancies, rheumatoid arthritis, connective tissue disease or inflammatory bowel disease. Almost all patients using only inhaled corticosteroids had a diagnosis of COPD, chronic bronchitis, emphysema or asthma, but were otherwise comparable to non-users. Charlson Comorbidity Index scores were higher for all groups of corticosteroid users compared with non-users.
Baseline characteristics of corticosteroid users and non-users among patients with perforated diverticular disease
Mortality risk in patients with perforated colonic diverticular disease
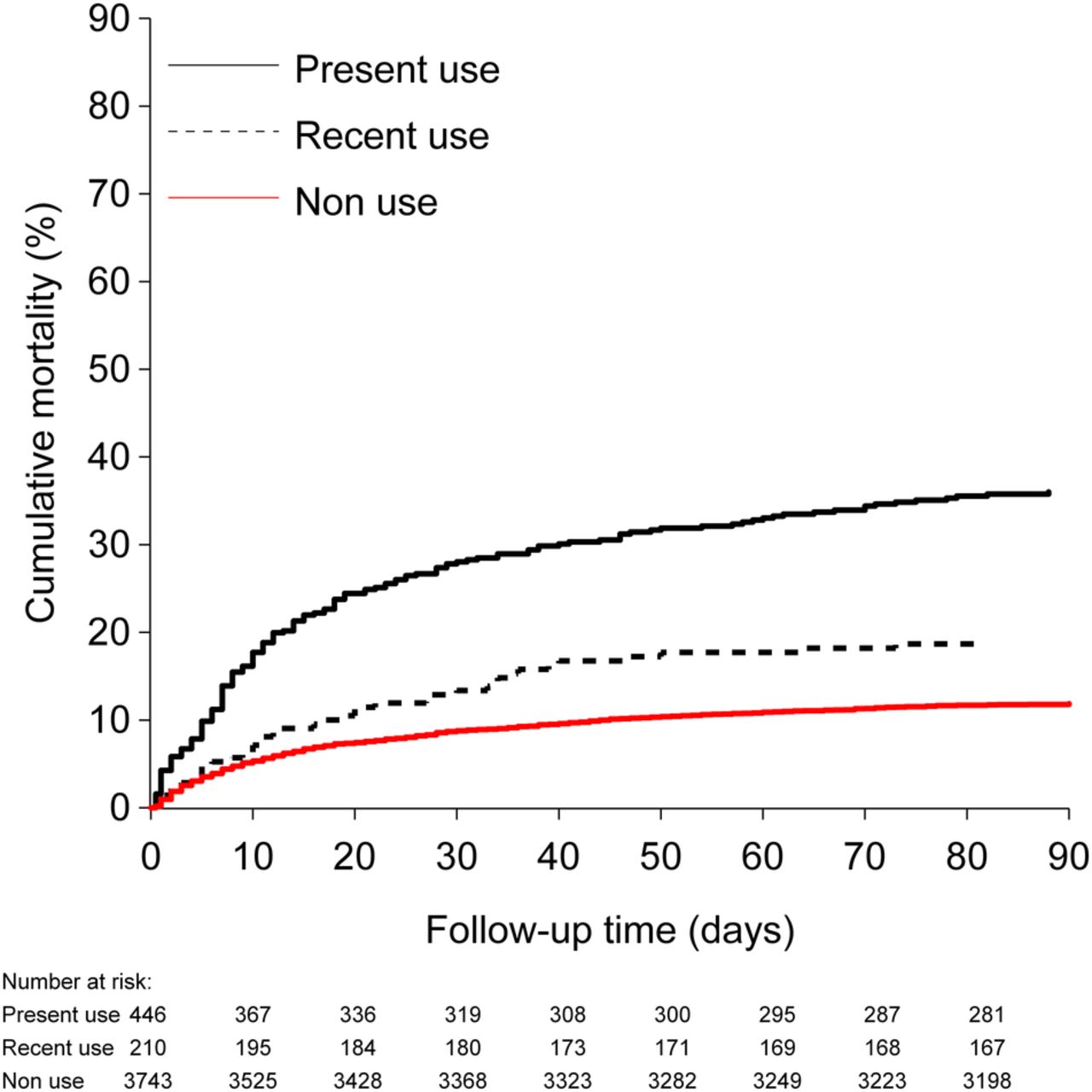
A total of 889 patients (19.2%) with perforated diverticulitis died within 1 year following their diagnosis (table 2). Mortality risk in non-users of corticosteroids was 4.4% after 7 days, 8.8% after 30 days, 11.9% after 90 days and 15.6% after 1 year. This risk was doubled for current users of corticosteroids (adjusted HRs ranging from 1.96 (30-day mortality) to 2.10 (7-day mortality)), with mortality risks reaching 14.2% after 7 days and 47.6% after 1 year (figure 1). Mortality risk was even higher for new corticosteroid users, increasing from 15.7% 7 days postdiagnosis to 52.5% after 1 year. Among chronic corticosteroid users, mortality risks also were almost doubled, with adjusted HRs of 1.89 after 7 days and 1.74 after 1 year, and absolute mortality risks reaching 13.7% after 7 days and 45.9% after 1 year.
Mortality among patients with systemic corticosteroid use, regardless of use of intestinal acting or inhaled corticosteroids compared with non-use

Cumulative mortality in patients with systemic corticosteroid use, regardless of other use.
Mortality risk according to 1-year cumulative dose
In our study population, 124 patients had a 1-year cumulative dose ≤625 mg, 144 patients had a 1-year cumulative dose >625–2000 mg, 140 patients had a 1-year cumulative dose >2000–3500 mg and 86 patients had a 1-year cumulative dose >3500 mg (table 3). A higher 1-year cumulative dose was not clearly associated with higher mortality risk in patients with perforated diverticular disease.
Mortality among patients with current use of systemic corticosteroids, regardless of other corticosteroid use, according to 1-year cumulative dose compared with non-use
Abdominal surgical procedures
In total, 2497 (53.8%) of 4640 patients had a diverticulitis-related surgical procedure (table 1). The percentage of patients with surgery within 30 days before or after incident perforated diverticular disease was higher among systemic corticosteroid users (62.9%) compared with users of inhalation corticosteroids only (56.6%) and non-users (52.1%). Patients using systemic corticosteroids had a surgical procedure resulting in a stoma (33.8%) more often than patients not using corticosteroids (22.6%).
Within categories of surgery (explorative surgery including lavage, stoma, resection with primary anastomosis), mortality risk was increased when comparing current users to non-users. After explorative surgery, mortality risk after 1 year was 14.8% for non-users and 43.5% for current users (adjusted HR 1.12 (95% CI 0.69 to 1.83)). For patients who received a stoma, mortality risk after 1 year was 26.5% for non-users and 48.8% for current users (adjusted HR 1.37 (95% CI 1.03 to 1.82)). After a resection with primary anastomosis, mortality risk after 1 year was 15.2% for non-users and 54.1% for current users (adjusted HR 2.88 (95% CI 1.57 to 5.28)).
Subgroup and sensitivity analyses
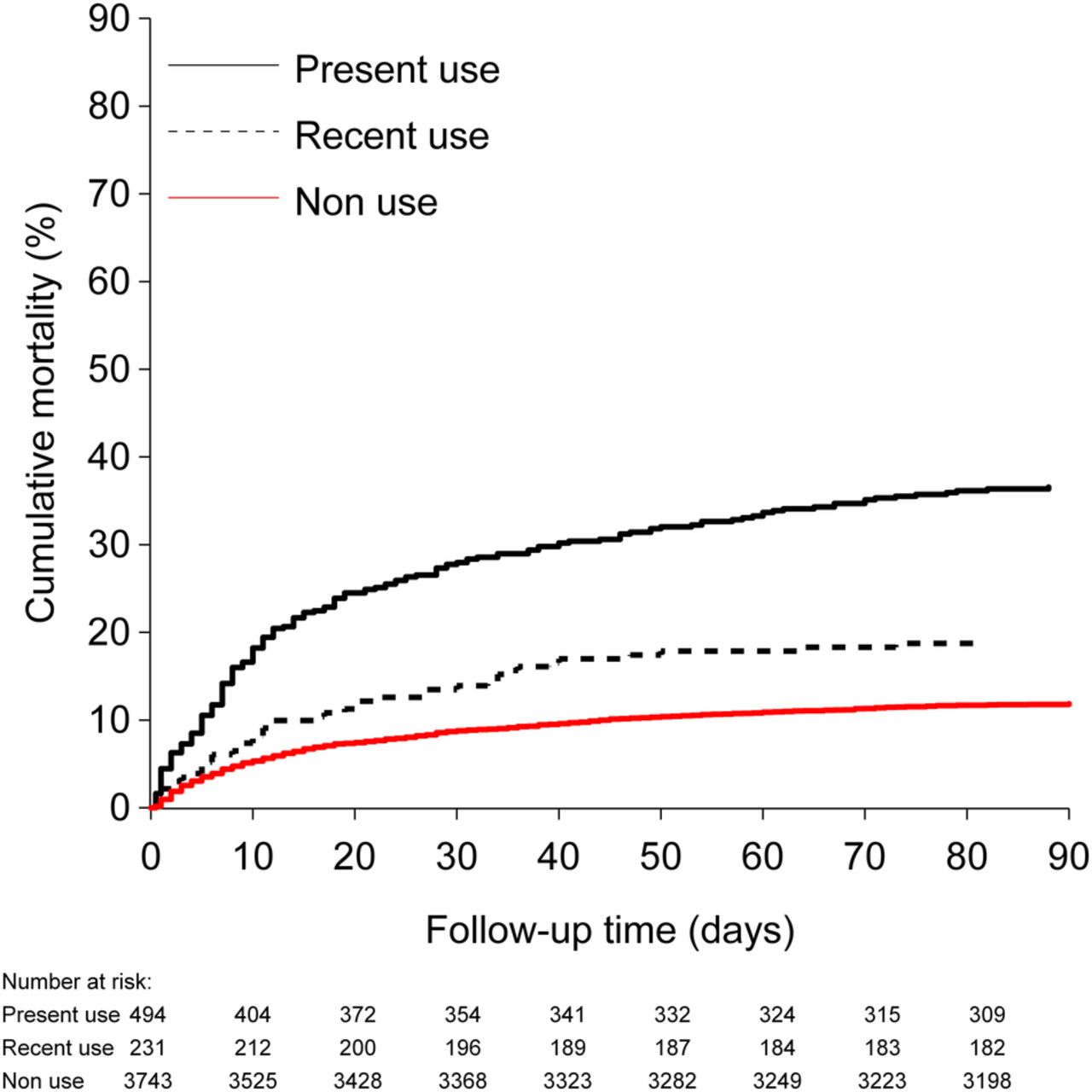
The mortality risk among patients currently using systemic corticosteroids only (13.9% after 7 days and 48.0% after 1 year) was comparable to that among patients using systemic corticosteroids regardless of other corticosteroid use (figure 2). Compared with non-users, patients who currently used only inhaled corticosteroids also had an increased mortality risk (6.2% after 7 days and 22.3% after 1 year), with an adjusted HR ranging from 1.44 to 1.85 (table 4).
Mortality among current corticosteroid users: subgroup and sensitivity analyses compared with non-use
{kind=link}
{kind=link}
Cumulative mortality in patients with systemic use of corticosteroids only.
When we excluded patients with malignancies, inflammatory bowel disease, a previous code for diverticular disease, or rheumatic diseases including mixed connective tissue disease, the results of the analysis of current users of systemic corticosteroids regardless of use of other corticosteroids did not materially change for mortality risk after 7, 30, 90 days or 1 year.
Discussion
We examined mortality risks between corticosteroid users and non-users among patients with perforated diverticular disease. One-year mortality risk for current users of corticosteroids was 47.6%, double that of non-users after adjustment for confounders. One-year mortality risk was even higher for new corticosteroid users: 52.5%. Thus, corticosteroid use was clearly associated with an increased mortality risk for patients with perforated diverticular disease, continuing until at least 1 year after diagnosis, regardless of corticosteroid dose.
This is the first large cohort study comparing mortality risks between corticosteroid users and non-users among patients with perforated diverticular disease. The advantage of the cohort approach is the ability to calculate absolute mortality risks, which can inform clinical practice. Our study showed that corticosteroid use is a strong indicator for 1-year mortality. An earlier study of patients with perforated peptic ulcer disease reported a 30-day mortality ratio of 2.1 after corticosteroid use.27 This is in line with the increased mortality risk (adjusted HR of 1.96 for 30-day mortality) that we found among current users of systemic corticosteroids in the present study.
The following study limitations need to be taken into account in interpreting our results. Determination of exposure was based on redeemed prescriptions, which may not always coincide completely with medication taken by patients.28 We also did not consider use of corticosteroids for longer than a year before hospital admission. Also, since prednisolone and prednisone were the most frequently used systemic steroids (89%), the results in first line apply to this patient category; whether our results also apply to patients using steroids with high first pass metabolism needs further study. Finally, perforated diverticular disease may be misclassified,6 ,17 as the sensitivity of relevant ICD codes is not 100% accurate. Since misclassification is probably more likely in corticosteroid users (due to blinding of symptoms and severity of the condition), mortality risk is potentially overestimated if less severe cases in corticosteroid users go undetected.25 However, in analyses stratified by type of surgery, which most likely harmonises the diagnostic category, a similar increased risk was found.
The central causal question is whether increased mortality risk in corticosteroid users is actually caused by corticosteroid use prior to diagnosis. Clinical arguments underlying the rationale for a causal association are masked disease severity,17 impaired wound healing and increased infection risk,18 increased risk of venous thromboembolism20 and unrecognised adrenal insufficiency.29 The risk was doubled for corticosteroid users in our fully adjusted statistical model, but residual confounding (no perfectly valid data on actual disease severity status) might still be an issue. For instance, high mortality among patients using corticosteroids may be explained partially by the underlying diseases for which corticosteroids were prescribed. However, our subgroup analyses showed no clear differences when high-risk subgroups were excluded. Regardless of the causal question, our study indicated that corticosteroid use was an important prognostic factor for mortality.
Two explanations are possible for the lack of an association observed between mortality risk and dose. First, the risk may be associated with corticosteroid use per se, so that the maximum increase in risk is already reached at a low (but still supraphysiological) dose. Second, our classification did not distinguish between short-term, high-dose corticosteroid use and long-term, low-dose use, because the prescription database used does not provide certainty whether a drug is prescribed in high doses for short-term use, or in lower doses for longer duration. Although clinically short-term, high-dose corticosteroid use and long-term, low-dose corticosteroid use are very heterogeneous groups of patients, in our analysis according to dose, both translate into the same 1-year cumulative dose.
In conclusion, this study demonstrated that corticosteroid use was associated with increased mortality risk after diagnosis of perforated diverticular disease. Clinically, use of systemic corticosteroids should be regarded as an important risk marker for mortality among patients with this disease.
References
Footnotes
Contributors All authors contributed to the development of the study protocol and read and approved the final manuscript. EH-P extracted the data from the National Health Service Prescription Database and the Danish National Patient Registry, and performed the statistical analyses. LHAB first analysed the rough data from the statistical analyses and summarised their implications in this article. AMP related the implications to the endocrinology practice, whereas RE did the same for the gastroenterology practice. OMD paid attention to the epidemiological correctness of the implications that were made. HTS managed the entire research process and checked the final version of the article for completeness.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.