Article Text

Abstract
Background Today's highly efficacious, low-toxicity interferon-free treatment regimens for chronic hepatitis C virus (HCV) can cure most patients with HCV in 12–24 weeks. The aim of this study was to understand how the introduction of shorter duration treatment regimens for HCV will impact the capacity for treatment and value to society.
Methods A Markov model of HCV transmission and progression was constructed, incorporating nationally representative data on HCV prevalence, incidence and progression; mortality, treatment costs, medical expenditures, employment probabilities and disability payments in Germany. The model was stratified by HCV genotype and exposure route (1-time healthcare exposure, injection drug use and sexual activity). Treatment scenarios were based on German treatment guidelines and projected treatment capacity. The impact of different treatment scenarios on disease transmission and prevalence, quality-adjusted life years (QALYs), treatment costs, medical expenditures, employment and disability expenditures was calculated.
Results Depending on their adoption profile, new treatment regimens and protocols introduced over the next several years will increase HCV treatment capacity in Germany by 8–30%, reducing disease transmission and prevalence, increasing QALYs and adding €94–310 million in discounted social value (QALYs plus medical savings net of treatment costs) over a 30-year horizon. Additional social value in the form of higher employment and lower disability would also result.
Conclusions The introduction of shorter HCV treatment regimens and the resulting increased treatment capacity in Germany would result in large gains to society by reducing disease transmission and prevalence, resulting in longer, healthier, more productive lives for current and future generations.
- HEPATITIS C
- HEALTH ECONOMICS
- LIVER CIRRHOSIS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Hepatitis C virus (HCV) is a prevalent and burdensome disease, affecting 2–3% of the population globally.
▸ Significant treatment advances now can effectively cure most patients of HCV, with minimal side effects.
▸ The prices of these regimens, along with the availability of specialists and facilities, can restrict the number of patients who can be treated, a situation that is occurring in Germany.
▸ Regimens with shorter durations are expected to be approved, however, and may increase the number of patients able to be treated.
What are the new findings?
▸ Depending on their adoption profile, new treatment regimens and protocols introduced over the next several years will increase hepatitis C virus treatment capacity in Germany by 8–30%.
▸ Expansion of treatment capacity will generate accrued discounted social value (quality-adjusted life years plus medical savings net of treatment costs) of €94.4–€310.5 million in Germany over the next 30 years, relative to the current annual treatment capacity of 25 000 patients.
▸ Additional social value from higher employment and lower disability also would result from increased treatment capacity.
How might it impact on clinical practice in the foreseeable future?
▸ Increasing the number of patients with hepatitis C virus who are able to be treated can reduce disease prevalence and incidence considerably and lead to healthier and more productive lives.
Introduction
Background and objectives
Advances in hepatitis C virus (HCV) treatment have rapidly transformed the disease landscape in western countries: most patients can be cured, and the possibility of significantly reduced prevalence and even eradication may be within reach.1 However, significant ongoing disease transmission means that aggressive programmes to treat large patient populations quickly will be needed to achieve these outcomes. In its recent draft Global Health Sector Strategy on Viral Hepatitis, the WHO emphasises the importance of expanding treatment to reduce prevalence and thereby transmission of the disease, in support of its strategy to eliminate HCV as a major health threat by 2030.2 However, in many countries, payers face budget constraints and provide treatment only to the sickest patients.3 By restricting the number of patients treated, such constraints limit disease reduction and thereby diminish the social value available from treatment.4
Even in countries without fixed budget constraints, the availability of specialists and facilities to treat and monitor HCV patients may also limit the number of patients who can be treated over a fixed time period.5 In such cases, increasing the capacity to treat HCV becomes the key driver to maximising health gains and accelerating HCV eradication. Capacity can be increased in several ways, including adding liver specialists, training more healthcare providers to treat HCV or introducing regimens with shorter treatment durations, thereby reducing the number of visits and tests per patient treated.5
While new interferon-free regimens are highly efficacious and well tolerated, most require 12–24 weeks of treatment, depending on patient characteristics.6 Recent findings have demonstrated, however, that a limited number of ‘easy-to-treat’ genotype-1 patients can successfully be treated with an 8-week regimen, depending on the patients' viral load and liver status.7 The next generation of treatments promises to reduce the treatment duration and allow many more HCV-infected patients to be treated.8
Like many European countries, Germany faces an ongoing HCV epidemic with a non-declining rate of new infections since 2009.9 With its generally open access to HCV treatment, Germany provides a good environment for modelling the impact of increases in HCV treatment capacity resulting from the expected introduction of shorter treatment regimens. Treatments with shorter durations can reduce the need for healthcare resources in the short term, through fewer tests and visits, and in the long term, through fewer infected patients. Most importantly, increasing treatment capacity will accelerate the eradication of HCV, reduce the number of disease-related deaths, lower disease transmission rates and lead to healthier, more productive lives.
Methods
We use a discrete-time Markov model, which has been described elsewhere, to follow the movement of HCV-susceptible and HCV-infected patients through various stages of liver disease and treatment over a 30-year period beginning in 2015.4 While most published models examining the economic impacts of treating HCV follow a cohort of infected patients through disease progression and cure,10 ,11 our model takes a society-wide perspective and includes the dynamics of infection and disease transmission, explicitly considering the effect of treatment on the likelihood that currently uninfected individuals may become infected through contact with an infected person (see online supplementary appendix for the model schematic and details). Thus, our model considers the value of treatment resulting from curing those who are currently sick, as well as from preventing the infection of those who are currently susceptible to HCV but face a lower infection risk when others in the population are cured.
supplementary data
Model dynamics
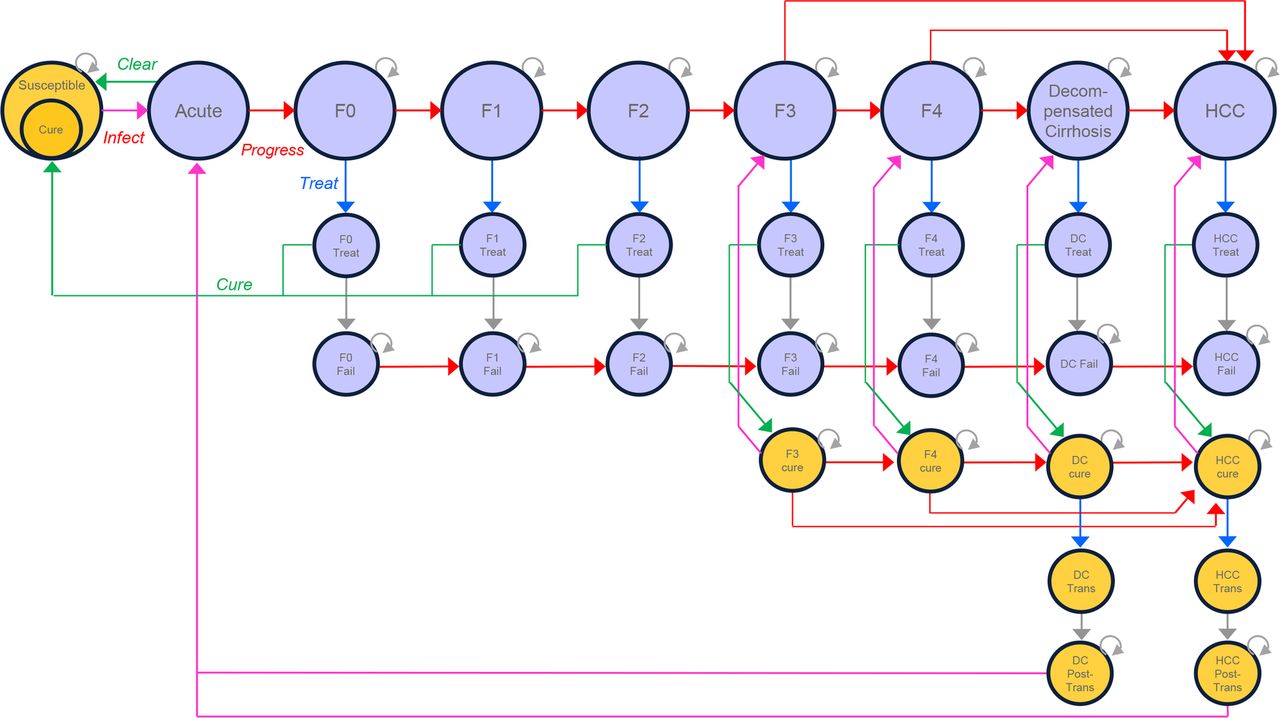
Once infected with HCV, patients progress through various levels of fibrosis (measured by the Metavir score), decompensated cirrhosis (DC), hepatocellular cancer (HCC), liver transplant and death, with transition rates derived from the literature (see online supplementary appendix for detailed values and citations). Patients who are diagnosed with a fibrosis score F0 and above are eligible for treatment with direct-acting antiviral regimens may achieve sustained viral response (SVR) and be considered cured. Patients who are treated and fail are not treated again, but remain infected and their liver disease continues to progress. Patients who are treated and cured return to the susceptible population and may be reinfected. If a patient is cured with fibrosis score F2 or lower, liver damage is assumed to resolve;12 ,13 if reinfected, that patient re-enters the infected population with an undamaged liver. If a patient is cured with fibrosis score F3 or above, liver damage is assumed to remain and continues to progress, albeit more slowly than in patients with active HCV infection.14 Figure 1 and the online supplementary appendix provide greater detail on model dynamics and assumptions.
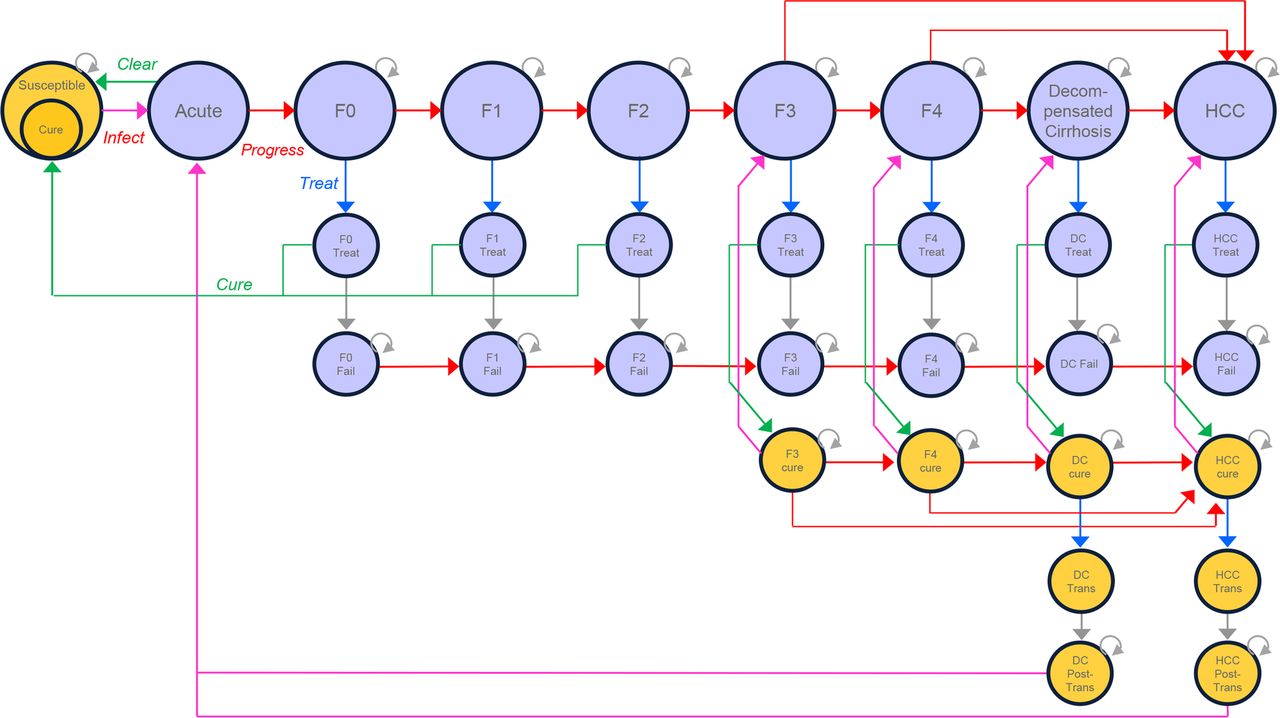
Model schematic. Schematic of the Markov model that simulates the progression of a hepatitis C virus (HCV)-susceptible population through infection, acute and then chronic HCV is shown. F0–F4, Metavir fibrosis scores 0–4; Treat, treatment stage; Fail, treatment failure; Cure, cured of HCV; DC, decompensated cirrhosis; HCC, hepatocellular carcinoma; trans, liver transplant.
Model populations
We model the HCV-infected and HCV-susceptible population in Germany with three distinct subpopulations, defined by the manner through which their members contracted the virus: one-time exposure in a healthcare setting (HC), injection drug use (ID) or sexual transmission (SX). Together, these groups account for most new and existing hepatitis C cases in Germany.9
The HC group is assumed to have acquired HCV through exposure to infected blood either as a healthcare worker or as a patient given infected blood products prior to universal screening for HCV introduced in 1995.15–17 Thus, we model this group as those aged 35+ at the start of the model. Importantly, this group is assumed not to experience any ongoing transmission. The ID group consists of people who regularly inject drugs; this group represents the largest number of HCV-infected persons and those with the highest infection rate in Germany today.18 The SX group consists of HIV-positive men who have sex with men, representing about 10% of the HCV-infected population and appearing to be particularly at risk for sexual transmission of HCV,19 but experience relatively low incidence compared with the ID group.15 ,20
Susceptible patients, those not currently infected with HCV but who are at risk, may become infected at rates determined dynamically by the proportion of infected patients in their exposure group. That is, there is a higher probability that a susceptible individual will be infected with HCV if there are more infected individuals in his subpopulation. We model the most prevalent genotypes in the German HCV population, 1, 2, 3 and 4, representing 99% of all HCV infection in Germany.15 We model each genotype group separately, since transmission dynamics may vary depending on the prevalence of particular genotypes in the population. The online supplementary appendix provides more information about starting population characteristics.
We calculate employment levels by multiplying the number of people in each group by their probability of being employed, using employment probability estimates from Stahmeyer et al21 for the HCV-infected population and the OECD, German population statistics and Dirks et al22–24 for the uninfected population.
All model input parameters are taken from the published literature, as specified in the online supplementary appendix. Treatments applied are those currently being used in German clinical practice, and SVR rates are derived from phase III clinical trials (see online supplementary appendix for sources). Background mortality rates are from the German Life Tables,25 and adjustment factors for exposure group, genotype and disease stage are derived from published estimates. We rely on the most recently published data for the costs of treatment and non-treatment medical expenditures. Employment and disability data are taken from OECD employment statistics and the published literature.
Scenarios
We model four alternative scenarios, which differ by the number of patients who can be treated in a year. In every scenario, patients who are diagnosed with the most severe liver disease are treated first in each period, following current practice; after these patients are treated, those diagnosed with less severe disease are treated in sequence until the treatment capacity for that period is exhausted. During the next period, treatment begins again with the most severe diagnosed patients first, followed by successively fewer patients until capacity is again exhausted.
In the Baseline scenario, a maximum of 25 000 patients are treated annually, which reflects the most recent treatment volumes in Germany26–28 and is consistent with estimates used in other recent studies.29
Three additional scenarios are modelled to simulate increasing future treatment capacity resulting from the expected introduction of therapies with shorter treatment durations for some patients.30–33 While precise treatment capacity projections are not available, we developed estimates using the following logic: we assumed that the average patient with HCV begins DAA treatment with an initial visit to a specialist, followed by visits every 4 weeks for the duration of treatment, and a final visit after treatment completion. Patients on a 12-week regimen thus will average 5 specialist visits, while those on 8-week and 6-week regimens will average 4 and 3.5 visits, respectively. Moving from a 12-week to an 8-week or 6-week regimen subsequently decreases the specialist resource requirement by 20–30%, and those now available resources can be applied to treating more patients each year. Note that, if the introduction of shorter duration therapies enables more patients to be cured prior to reaching F4, then some of these follow-up visits would be eliminated as well, freeing up still more resources than the 20–30% currently estimated. Thus, shorter duration therapy may enable treatment scenarios that are even more ambitious than our ‘Aggressive’ scenario.
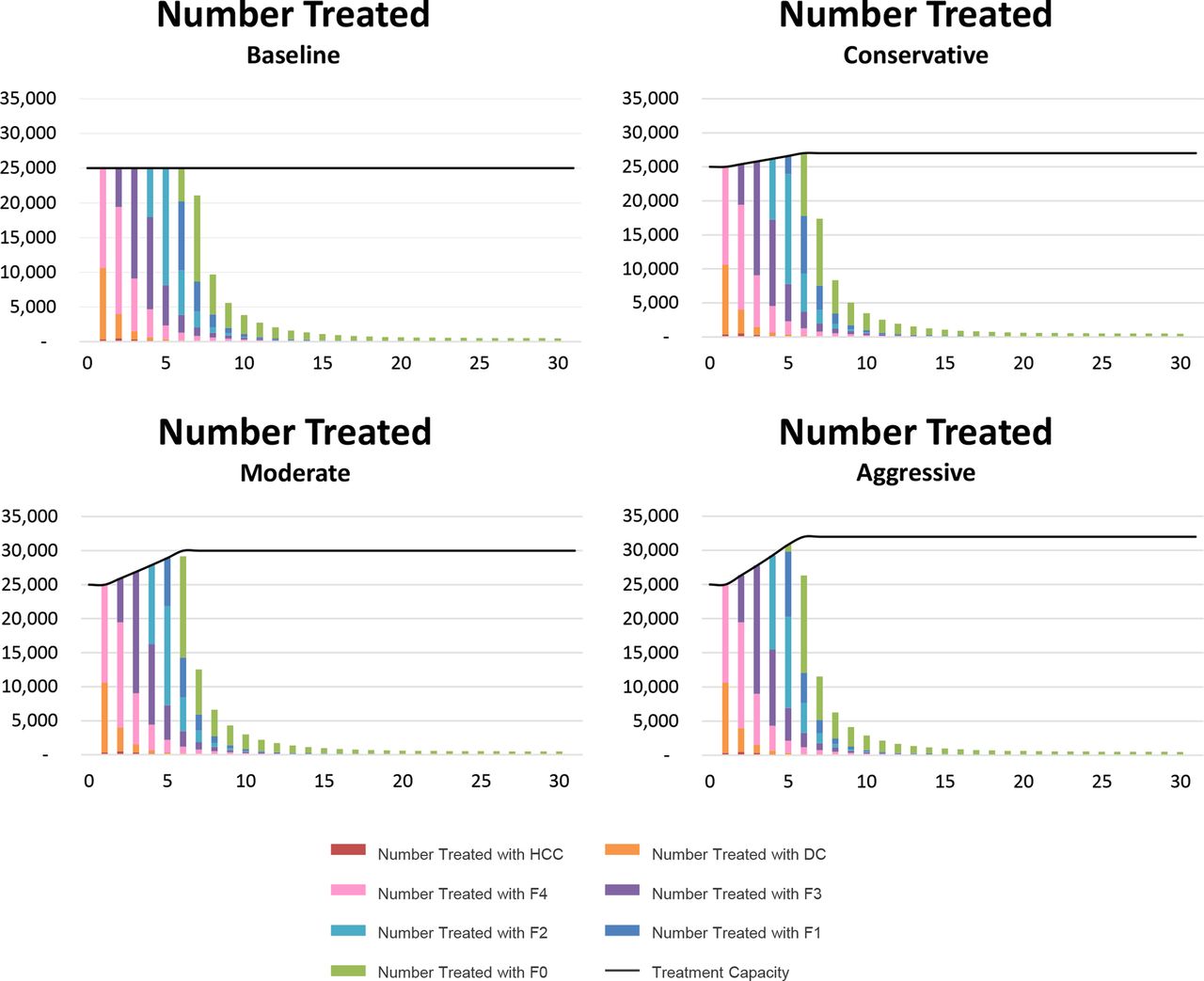
In our Conservative scenario, we assume that the introduction of therapies with shortened treatment durations increases annual treatment capacity from 25 000 patients with HCV to 27 000 (+8%) over 7 years; in our Moderate and Aggressive scenarios, annual treatment capacity is assumed to increase to 30 000 patients (+20%) or 32 500 (+30%), respectively. Figure 2 demonstrates the treatment capacity and the number of patients treated over time for each of the four scenarios.
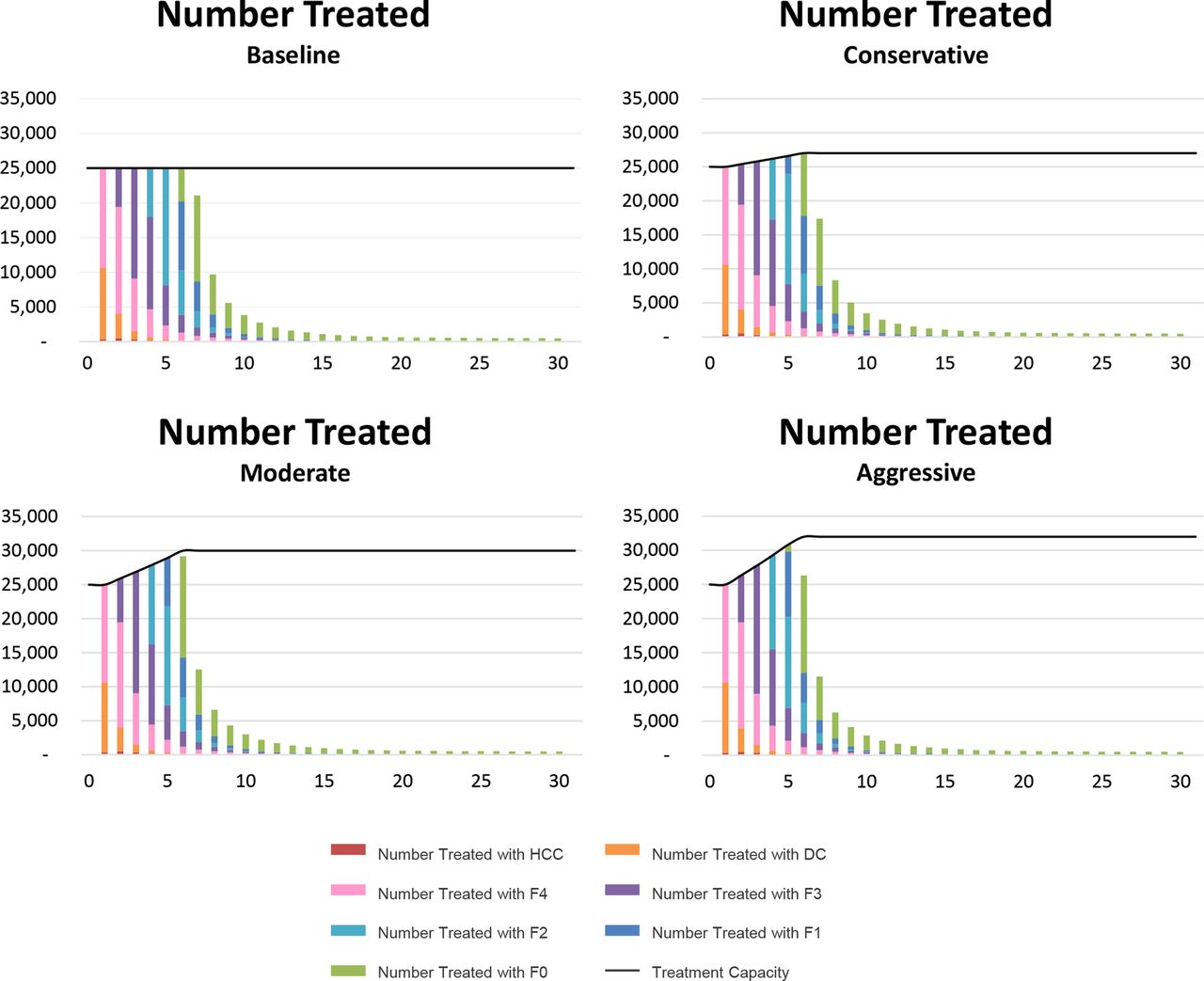
Treatment capacity and number of patients treated in each scenario. The treatment capacity and the number of patients treated over time for each of the four scenarios are shown. X-axis indicates time horizon in years; Y-axis indicates the number of patients treated. F0–F4, Metavir fibrosis scores 0–5; DC, decompensated cirrhosis; HCC, hepatocellular carcinoma.
Outcomes
Over the course of the simulation, we measure outcomes including the size of the infected population and the severity of liver disease among them, aggregate quality-adjusted life years (QALYs) among the infected population, treatment costs, medical expenditures, employment levels and disability expenditures.
All monetary outcomes are reported in 2015 Euros, and discounted at 3% per year according to local recommendations.34 QALYs are valued at €30 000 each, at the lower end of the range of €30 000–50 000 per QALY commonly applied in European healthcare systems.35 ,36
Results
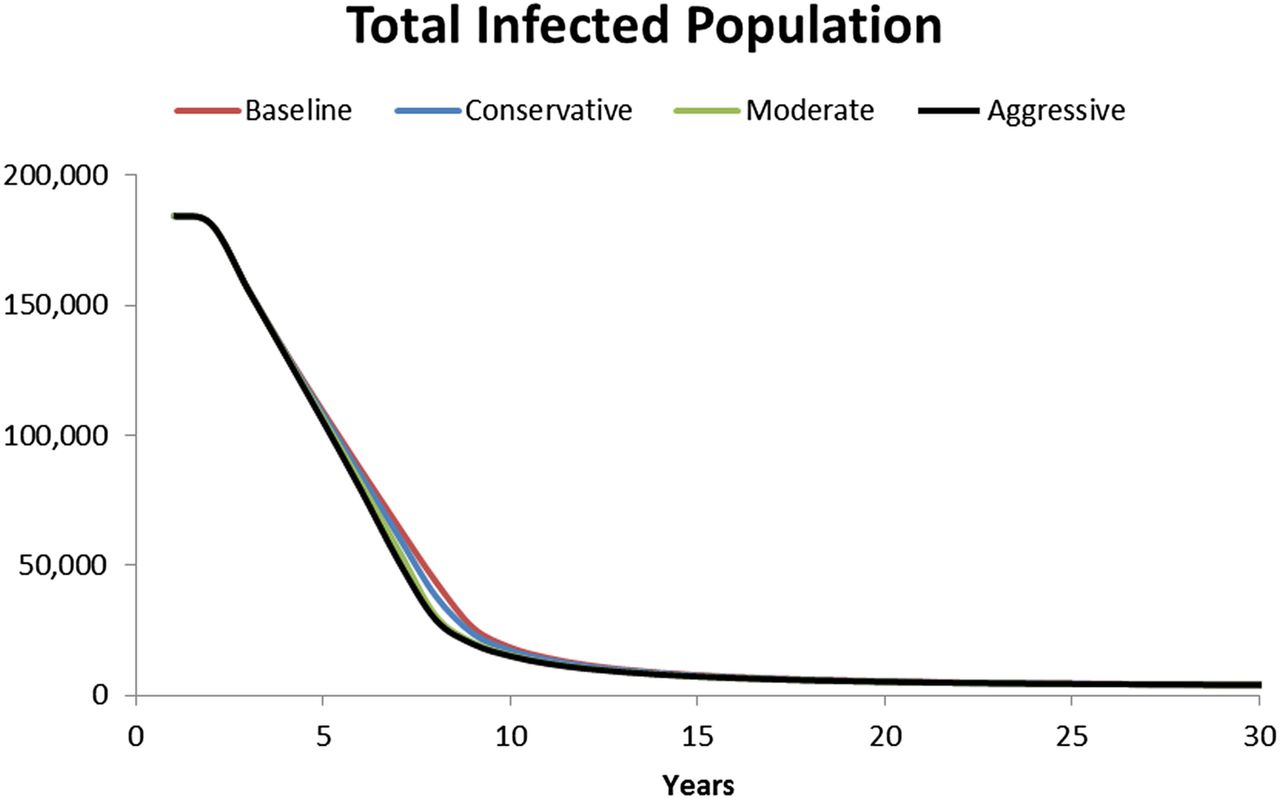
Figure 3 depicts the total infected population over time in each scenario. For starting prevalence, we rely on published estimates that 0.2% of the German adult population is currently infected,37 resulting in a prevalence curve that begins at 184 449 individuals infected and declines over time under all scenarios, but does so quicker in those scenarios treating more patients. Under the Baseline and Conservative scenarios, the infected population falls to under 5000 after 22 years; in the Moderate and Aggressive scenarios, it does so 1 year earlier.
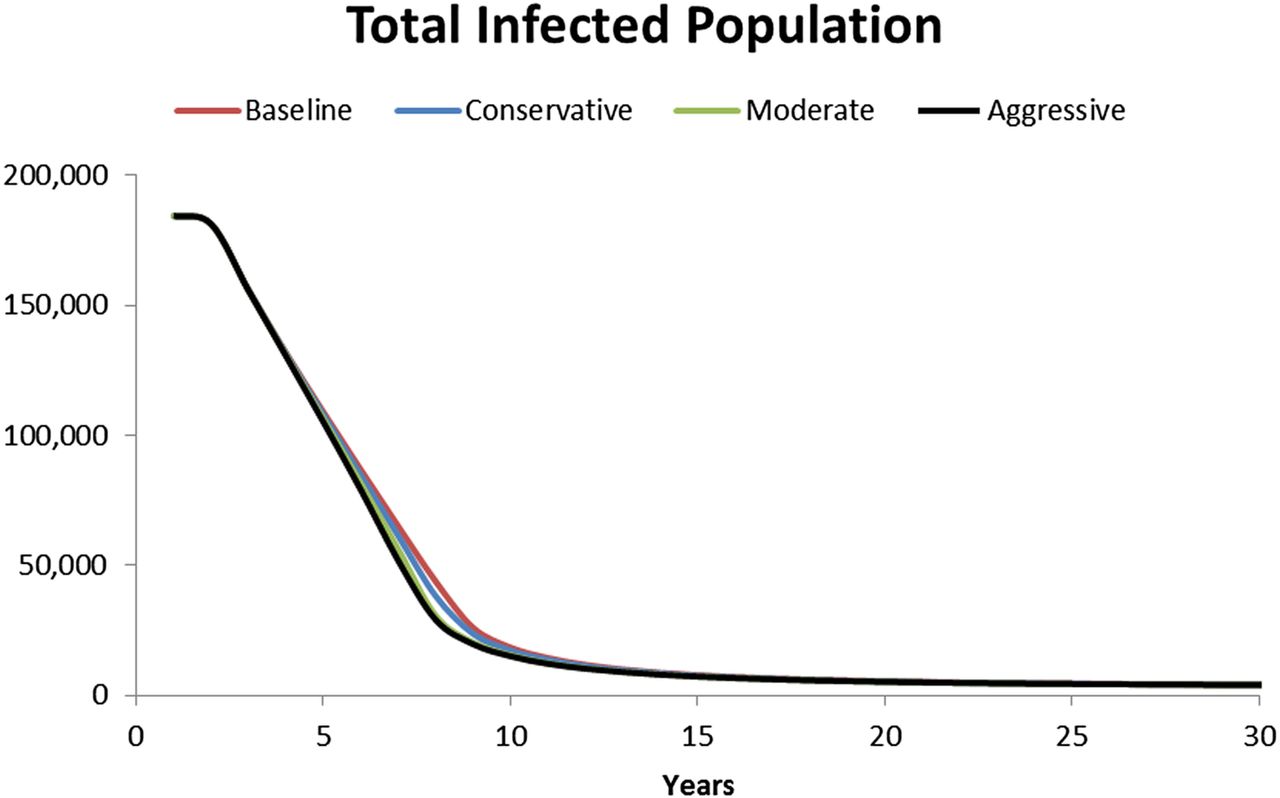
Total infected population over time. The number of patients infected with hepatitis C in Germany over time under each treatment scenario is shown. X-axis indicates time horizon in years; Y-axis indicates the number of infected individuals.
As patients are treated, the model calculates per-period treatment costs, non-treatment medical expenditures and QALYs for each scenario. These values are cumulated and shown in figures 4 and 5, net of their values under the Baseline scenario. Figure 4 shows cumulative treatment plus non-treatment medical expenditures for the three capacity-increasing scenarios. All three have the same general shape: initial expenditures increase relative to the Baseline, since more patients are treated in the earlier periods. However, over time, expenditures decline relative to the Baseline, as the number of patients treated and the population-wide non-treatment medical expenditures fall below those in the Baseline. All three treatment scenarios result in lower cumulative expenditures than Baseline after 11 years. As shown in figure 5, all three scenarios result in more QALYs than Baseline after 3 years, with more QALYs added as more patients are treated. After 30 years, the Conservative, Moderate and Aggressive scenarios add a total of 4600, 11 000 and 16 000 QALYs above Baseline, respectively.

Cumulative treatment costs plus medical expenditures, net of Baseline. The total hepatitis C treatment costs and medical expenditures over time under each treatment scenario are shown. X-axis indicates time horizon in years; Y-axis indicates total costs in millions of Euros.
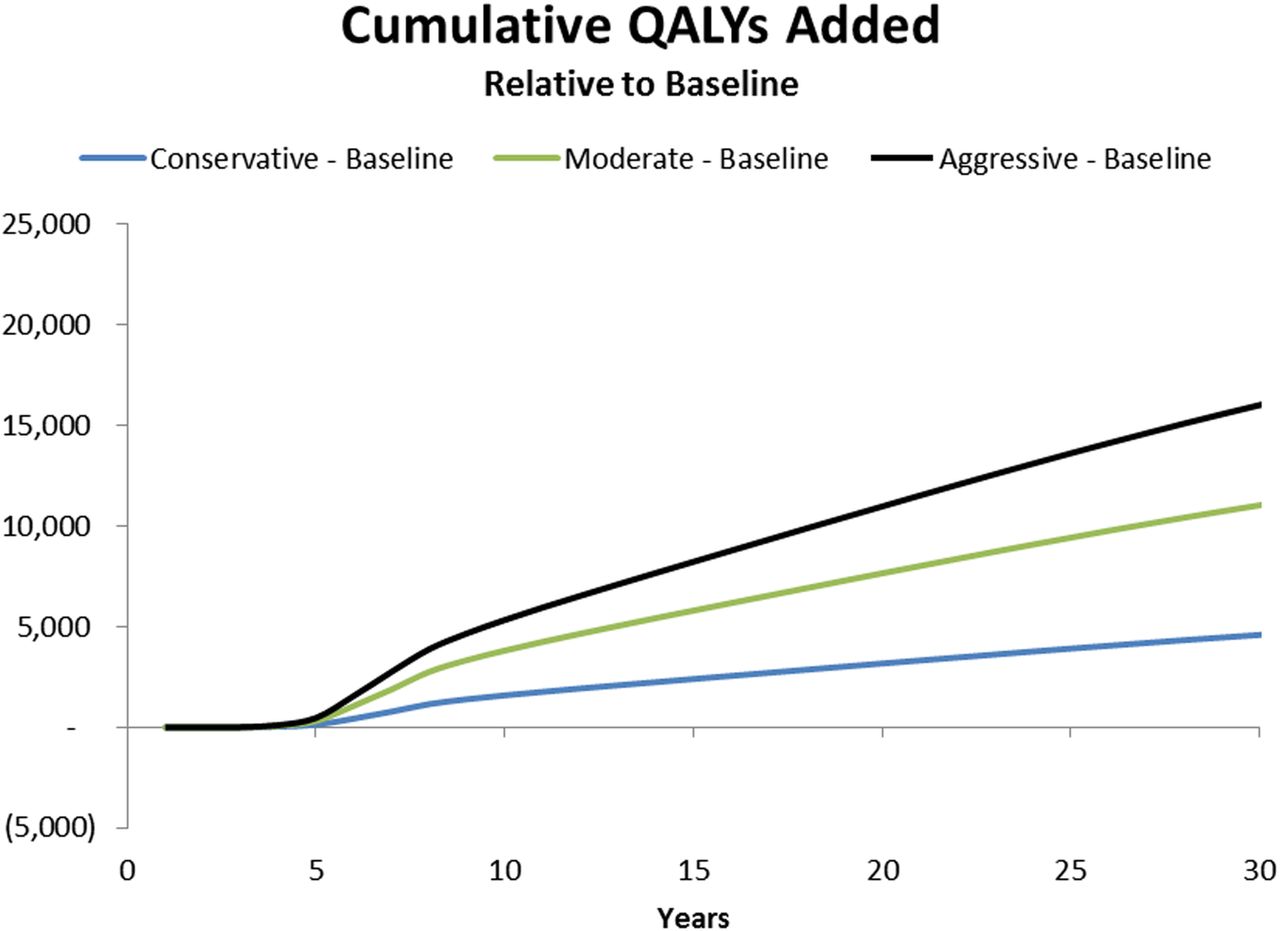
Cumulative quality-adjusted life years (QALYs), net of Baseline. The number of QALYs added over time under each treatment scenario net of the Baseline treatment scenario is shown. X-axis indicates time horizon in years; Y-axis indicates cumulative QALYs added. QALYs, quality-adjusted life years.
Figure 6 aggregates and discounts the value of QALY gains less treatment and non-treatment medical expenditures, net of Baseline, into a total discounted value of health gains resulting from HCV treatment. With QALYs valued at €30 000 and all values discounted at 3%, the Conservative scenario adds €94.4 million above Baseline over 30 years, while the Moderate and Aggressive scenarios add €229.9 million and €310.5 million, respectively. All three scenario comparisons are characterised by dominance.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall social value of capacity-increasing scenarios, net of Baseline. The discounted value of quality-adjusted life years added plus savings in medical expenditures from reduced disease prevalence and severity less treatment costs under each treatment scenario, net of the Baseline treatment scenario are shown. X-axis indicates each treatment scenario, net of Baseline; Y-axis indicates total value in billions of Euros. QALYs, quality-adjusted life years.
The literature suggests that patients cured of HCV may be more productive and incur lower disability expenses as their health improves.38 ,39 All three capacity-expanding scenarios result in greater employment in all simulation years, and lower disability expenditures, relative to Baseline
Discussion
Recent studies have demonstrated the cost-effectiveness of new HCV therapies in various settings based on traditional cost-effectiveness or disease burden models.10 ,11 Our model extends this understanding by incorporating the effect of treatment on future disease transmission—when a patient is cured, benefits accrue to the infected individual, as well as to the uninfected-but-susceptible population whose risk of future infection is decreased. To the best of our knowledge, ours is the first analysis of social value from HCV treatment in Germany that incorporates these reinfection and transmission dynamics.
The introduction of remarkably effective HCV treatments in recent years has caused large numbers of patients to seek treatment, making treatment capacity an especially important concern in many countries. In 2015, roughly 25 000 HCV patients were treated with direct-acting antiviral therapies in Germany, using protocols that treat most patients in 12–24 weeks.27–29 In the next several years, therapies currently in development that reduce HCV treatment duration even further are expected to become available in Germany. Even if the current number of healthcare providers and treatment facilities remain fixed, these shorter duration therapies could increase the number of patients who can be treated each year. Our model demonstrates that such expansion of treatment capacity will generate an accrued value of €94.4–€310.5 million over the next 30 years, relative to a Baseline scenario in which no shortened-duration treatment options become available and capacity remains at 25 000 patients/year indefinitely. This additional value comes through several mechanisms: first, adding capacity and treating more patients sooner reduces disease prevalence faster, both because it cures patients who are currently sick, and reduces the risk of future infection to those currently uninfected. Reducing disease prevalence earlier adds population life-years and improves their quality, so total QALYs increase by 4600–16 000 over 30 years.
Increasing treatment capacity also increases upfront treatment costs, but by curing more patients of HCV, these scenarios also prevent further liver disease and decrease future non-treatment medical expenditures for costly conditions such as HCC or DC. Higher treatment costs are thus offset by reduced medical expenditures, and all three capacity-increasing scenarios are money-saving after 11 years.
Expanding treatment capacity also leads to additional productivity, as patients cured of HCV are more likely to work and draw lower disability payments compared with those with active infection. While these sources of value are not included in the calculations of health gains from above, they are potentially large, adding employment of between 150 and 500 full-time workers/year, and reducing disability outlays after 4 years.
Additionally, we have assumed that treatment costs are constant over the first 15 years of the simulation. In fact, entry of other treatment options will most likely lower costs over the next few years, resulting in lower treatment costs for all scenarios, enabling more patients to be treated with a given budget, and generating even greater social value. While we have focused on the mechanism of expanding treatment capacity to reduce HCV prevalence and societal impact, other strategies could also be explored. For example, what is the optimal capacity to eradicate HCV, given other policy priorities and budget demands? Also, since patients with less severe disease are generally less costly to treat, the number of patients treated with a fixed budget could be increased by prioritising less expensive patients ahead of more expensive ones. Such a strategy might reduce prevalence more quickly at a lower cost, but the ethical implications of failing to prioritise the sickest patients would need to be addressed. In fact, we explored treating patients with the least serious disease first—while this does increase total social welfare, it also results in higher mortality in early years, as many of the most serious patients die waiting for treatment (see online supplementary appendix for details). Precisely which type of strategy a country should pursue in treating HCV is an interesting question for future research.
Limitations
As with any modelling exercise, ours is an imperfect representation of the real world. First, while all model parameter values were derived from published sources, they are estimated with some error, and some were unavailable in precisely the form required. For example, for some parameters such as QALY weights and employment probabilities, estimates stratified by genotype or exposure group or disease severity as required by the model were unavailable; in these cases, we used unstratified values. Also, some clinical trials involve very small sample sizes for certain patient subsets; in these cases, we used more conservative SVR rates based on larger patient subsets, potentially underestimating future treatment effects. In some cases, owing to lack of published data, we used efficacy rates based on clinical trial results for treatment-naïve patients, while SVR rates for treatment-experienced patients may be lower. (However, the proportion of treatment-experienced patients in Germany will most likely shrink over time, minimising the impact of this particular limitation.) Basing SVR rates on clinical trials may overestimate the benefits of treatment in practice, although this issue may be of decreasing concern, as several recent studies have shown comparable efficacy between real-world and trial settings.40–44 We explore the sensitivity of our results to variations in various parameter values in the online supplementary appendix; while the precise magnitudes of results vary, the overall conclusions do not: across a wide range of parameter values, model results demonstrate that increasing treatment capacity reduces the infected population and adds significant social value.
Finally, while our treatment scenarios prioritise patients strictly according to the severity of their liver disease, actual treatment patterns will reflect to some degree the order in which patients present for treatment, so some less severe patients may be treated before more severe patients. Thus, the distribution of disease severity among treated patients in our model will tend to differ from that observed in the German population.
Conclusion
While other studies have considered expanded access to HCV treatment in Germany through increased diagnosis,5 to the best of our knowledge, this is the first analysis of the social and economic value of expanding treatment capacity through shorter treatment regimens in Germany.
While our analysis focused on the value resulting from shorter duration therapies, this is not the only mechanism by which new HCV regimens expand treatment capacity and subsequently reduce HCV infection. Innovations that increase efficacy or improve tolerability in currently treatable subpopulations, or improve treatment options in currently difficult-to-treat subpopulations, will all expand the set of patients who can be cured in a given healthcare system, and generate value similar to regimens that shorten treatment duration. Finally, while the results presented here are specific to HCV treatment in Germany, similar analyses could easily be performed for other countries, most likely with similar results—expanding HCV treatment would most likely create value in many countries beyond Germany.
References
Footnotes
Contributors US, DW, KVN and RB are responsible for study concept and design; DW, KVN, CH, JS,CK and US are responsible for acquisition of input data; US, DW, KVN, CH, RB, JS and CK are responsible for analysis and interpretation of data; KVN, CH, US, DW, JS and CK are responsible for drafting of the manuscript; US, DW, KVN, CH, RB, JS and CK are responsible for critical revision of the manuscript for important intellectual content; KVN and CH are responsible for statistical analysis; US, DW, JS and CK are responsible for supervision.
Funding This work was supported by Janssen Pharmaceuticals NV, a pharmaceutical company of Johnson & Johnson, through consulting fees paid to PHE. Janssen and PHE collaborated to conduct the study. Janssen and PHE participated in the interpretation of data, review and approval of the manuscript.
Competing interests US is an employee of Janssen Pharmaceutica NV Belgium and DW is an employee of Janssen-Cilag GmbH Germany. Both hold stocks at Johnson & Johnson. KVN and CH are employees of Precision Health Economics.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.