Article Text

Abstract
We report a case of a woman with a medical history of classic Whipple surgery who underwent endoscopic ultrasound (EUS)-guided pancreatic drainage due to smouldering acute pancreatitis secondary to an obstructing pancreatic ductal stone. A gastro-pancreaticojejunostomy anastomosis was created anterogradely, with dilation of both the anastomoses in the same procedure, with subsequent decompression of the pancreatic duct. Endoscopic retrograde pancreatography (ERP) is often impossible to perform in patients with post-Whipple procedure anatomy due to inaccessibility to the pancreaticojejunostomy anastomosis. EUS-guided pancreatic drainage may be offered in these patients in whom the pancreatic duct cannot be accessed at ERP. It has been used as a platform for access to and drainage of the pancreatic duct either by rendezvous or transmural drainage. However, only one of four patients achieve successful completion of the rendezvous procedure. There are limited data regarding safety and long-term outcome of this procedure, as well as scant guidelines on the optimal time for leaving stents in place. We believe definitive endoscopic therapy should be attempted, whenever possible, after relief of obstruction. In our case, we expect that stent occlusion is inevitable and that long-term drainage is possible due to drainage occurring between the stent and the stone.
- ENDOSCOPIC RETROGRADE PANCREATOGRAPHY
- ENDOSCOPIC ULTRASONOGRAPHY
- PANCREATIC DISORDERS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Case report
An 82-year-old woman with a medical history of classic Whipple surgery due to pancreatic adenocarcinoma presented 3 months prior with smouldering acute pancreatitis secondary to an obstructing pancreatic ductal stone (figure 1). Attempted endoscopic retrograde pancreatography (ERP) with a paediatric colonoscope (Olympus PCF-PH190, Center Valley, Pennsylvania, USA) failed to reach the biliary and pancreatic anastomoses. Endoscopic ultrasound (EUS)-guided intervention was undertaken. A linear echoendoscope (Olympus GFUCT-180) was positioned in the stomach. Endosonographic signs of chronic pancreatitis were present, with 6 mm pancreatic duct dilation. The wall of the pancreatic duct was punctured transgastrically with a 19-gauge fine-needle aspiration needle (Expect, Boston Scientific, Marlborough, Massachusetts, USA) (figure 2). Contrast was instilled under fluoroscopic guidance and a pancreatogram was obtained (figure 3). An obstructive stone was identified near the pancreatic anastomosis. A 260 cm 0.035″ hydrophilic guidewire (GLIDEWIRE, Terumo Medical Corporation, Somerset, New Jersey, USA) was passed though the transgastric access into the pancreatic duct and across the surgical pancreaticojejunostomy into the jejunum. Using electrocautery, a needle knife (Clevercut 3V, Olympus) was advanced over the wire to allow passage through the stomach wall and pancreatic parenchyma into the pancreatic duct. After the needle knife was passed into the jejunum (figure 4), the wire was exchanged for a stiffer wire (Superstiff Jagwire, Boston Scientific). The surgical pancreaticojejunostomy and the EUS created pancreaticogastrostomy tracts were balloon dilated to 4 mm (Hurricane, Boston Scientific) (figure 5). A 7 Fr 10 cm double pigtail stent (Advantix, Boston Scientific) was placed transgastrically across the gastrojejunostomy and pancreaticojejunostomy with the proximal end in the stomach and distal end in the jejunum (figure 6 and online supplementary video). The procedure was completed as an outpatient; there were no adverse events and the patient is clinically well 4 months later. The patient was offered additional interventions for stone removal to allow the stent to be removed, but she refused.
supplementary data
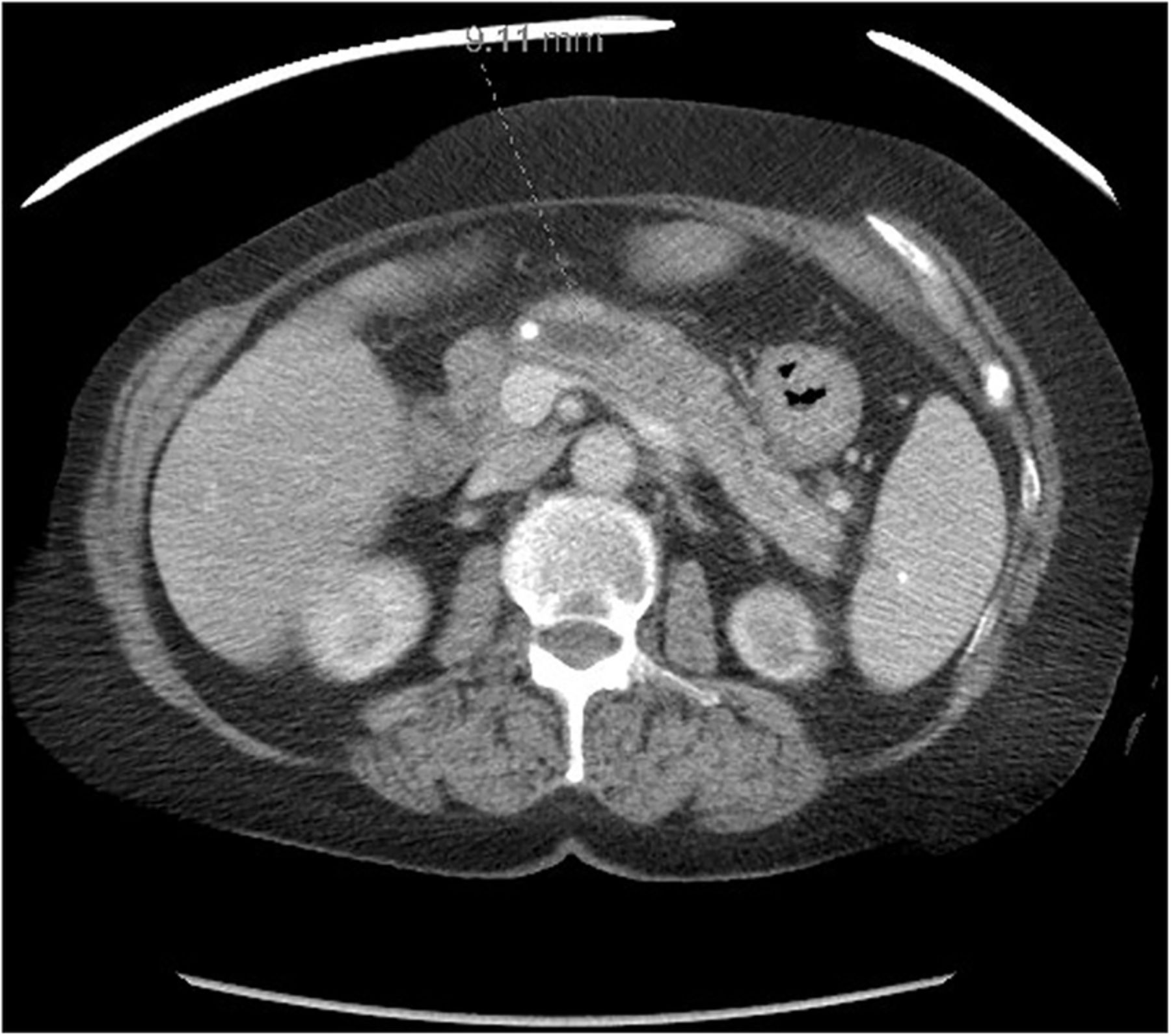
Transverse CT scan. Obstructive stone located near the pancreatic anastomosis with upstream dilation of the pancreatic duct.

Endosonographic image. Transgastric puncture of the wall of pancreatic duct with a 19-gauge fine-needle aspiration needle and instillation of contrast.
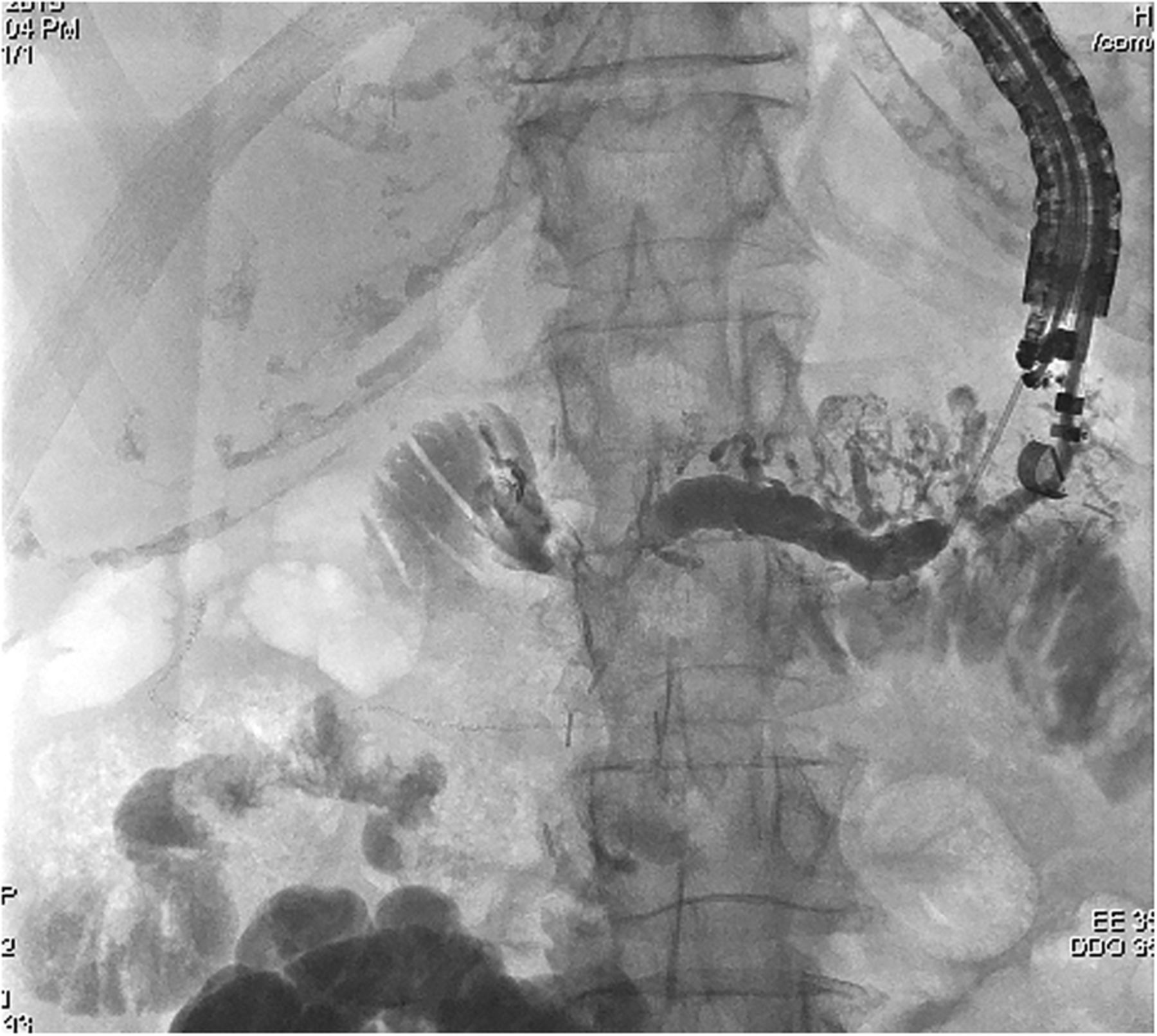
Fluoroscopic image. Pancreatogram after instillation of contrast.
Fluoroscopic image. Guidewire inside the pancreatic duct and passed across the pancreaticojejunostomy into the jejunum, with pancreatic ductal stone seen near the jejunopancreatic anastomosis.

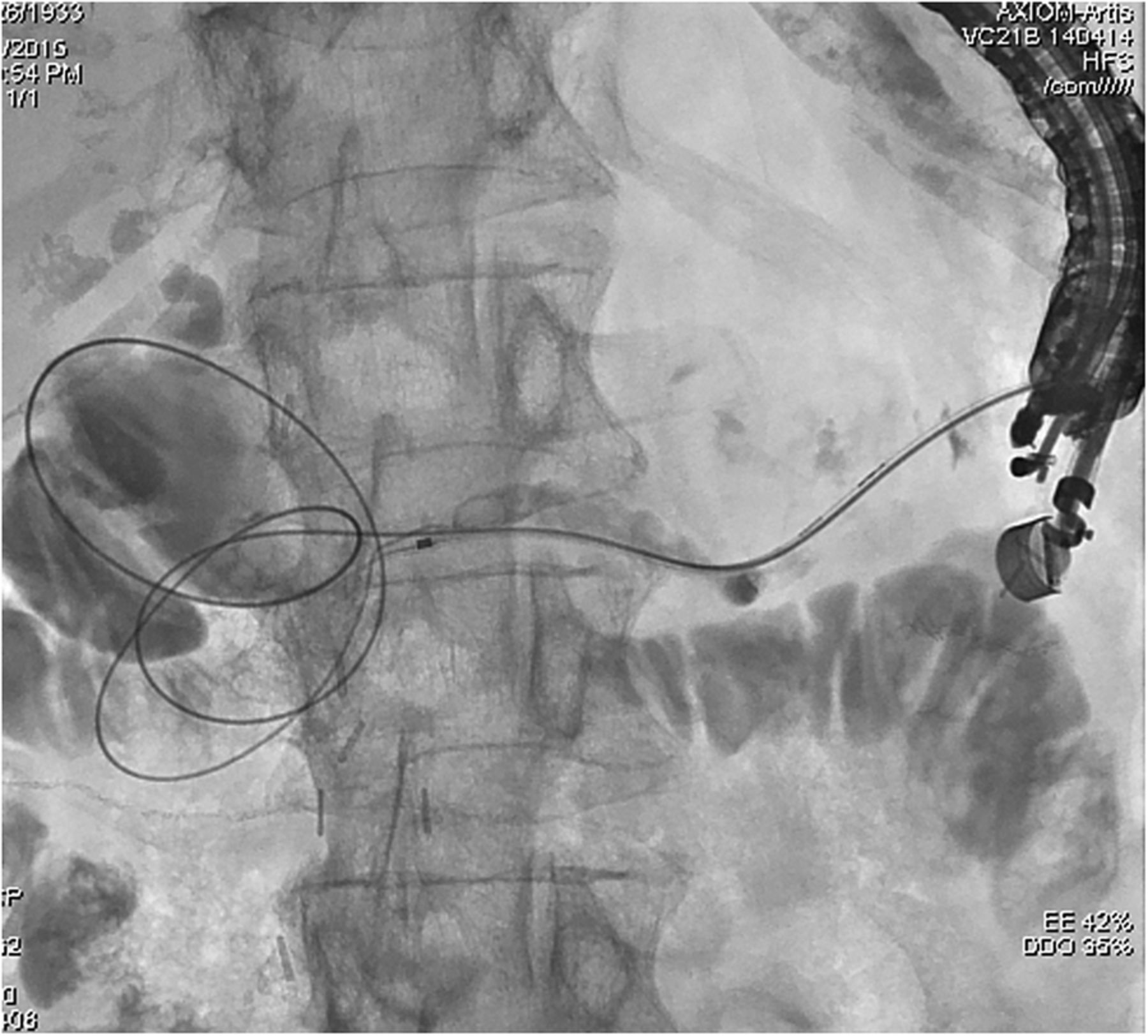
Fluoroscopic image. Dilation of the pancreaticojejunostomy and pancreaticogastrostomy with a 4 mm balloon.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fluoroscopic image. A 7 Fr 10 cm double pigtail stent across the pancreaticojejunostomy and gastrojejunostomy with the proximal end in the stomach.
ERP is often impossible to perform in patients with post-Whipple procedure anatomy due to inaccessibility to the pancreaticojejunostomy anastomosis. EUS-guided pancreatic drainage, first described in 1995,1 may be offered in these patients in whom the pancreatic duct cannot be accessed at ERP.2 It has been used as a platform for access to and drainage of the pancreatic duct either by rendezvous or transmural drainage.3 However, only one of four patients achieve successful completion of the rendezvous procedure.4 Even with transmural drainage, mean technical success may not be superior to 82%, possibly due to lack of a dedicated pancreatic stent designed for EUS-guided placement.5 Transmural drainage may be performed from the gastric6 ,7 or jejunum side.8 ,9 Even in cases where it is possible to reach the pancreaticojejunal anastomosis, retrograde pancreatic stent placement may be associated with difficulties in creating and dilating the fistula, when using a conventional echoendoscope.10 In our case, we were able to create a gastro-pancreaticojejunostomy anterogradely, with dilation of both the anastomoses in the same procedure, with subsequently decompression of the pancreatic duct. There are limited data regarding safety and long-term outcome of this procedure, as well as little information on the optimal time for leaving stents in place. We believe definitive endoscopic therapy should be attempted, whenever possible, after relief of obstruction. In the cases where pancreaticojejunal anastomosis can be reached with a colonoscope, a rendezvous stent placement could be considered, without need of creating a larger transgastric tract, which could potentiate a leak between the gastric wall and the pancreas. However, we could not reach the pancreaticojejunal anastomosis. Our option for future treatment would be electrohydraulic lithotripsy assisted by anterograde pancreatoscopy, followed by advancement of the stone fragments into the jejunum through the pancreaticojejunal anastomosis. However, the patient refused any additional interventions. Considering this, we expect that stent occlusion is inevitable, however, long-term drainage may still be possible due to drainage occurring between the stent and the stone.
Footnotes
Contributors THB performed the endoscopic procedure. ER-P and ISG attended the procedure. All the authors participated in the drafting and critical revision of the manuscript.
Competing interests ISG is a consultant for Boston Scientific. THB is a consultant for Olympus Medical Systems and Boston Scientific.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.