Article Text

Abstract
While most gastroenterologists are aware of the more common complications of endoscopy such as bleeding, infection and perforation, air embolism remains an under-recognised and difficult to diagnose problem due to its varying modes of presentation. This is the case of a 55-year-old man with right upper quadrant pain and imaging notable for cholecystitis and choledocholithiasis, who underwent endoscopic retrograde cholangiopancreatography (ERCP). During the ERCP, and shortly after a sphincterotomy was performed, he became hypotensive and hypoxic, quickly decompensating into pulseless electrical activity. While advanced cardiac life support was initiated, the patient passed away. Autopsy revealed air in the pulmonary artery suggestive of a pulmonary embolism. While air embolism remains a rare complication of upper endoscopy, increased awareness and prompt recognition of signs that may point to this diagnosis may potentially save lives by allowing for earlier possible interventions.
- BILIARY ENDOSCOPY
- ENDOSCOPIC PROCEDURES
- ENDOSCOPIC RETROGRADE PANCREATOGRAPHY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is a routine invasive endoscopic procedure often utilised for both diagnostic, and more commonly, therapeutic indications. An air embolism can result from any type of endoscopic procedure, yet, over the past decade, it has been reported at an increasing rate in literature as a complication of ERCP with more than 25 cases reported as of 2013.1 While there is speculation of the exact source of embolism, many researchers believe that the high-pressured air that is insufflated during the procedure to allow for adequate visualisation may be the source of the air that creates the embolism. The various methods by which the air is thought to ultimately enter the venous system include intramural dissection due to mucosal damage from high pressures, biliary venous fistulas, blunt abdominal trauma, and others.2 Risk factors thought to be associated with its development include history of penetrating liver trauma, previous bile duct surgeries, and gastrointestinal inflammation, among others.1
Case scenario
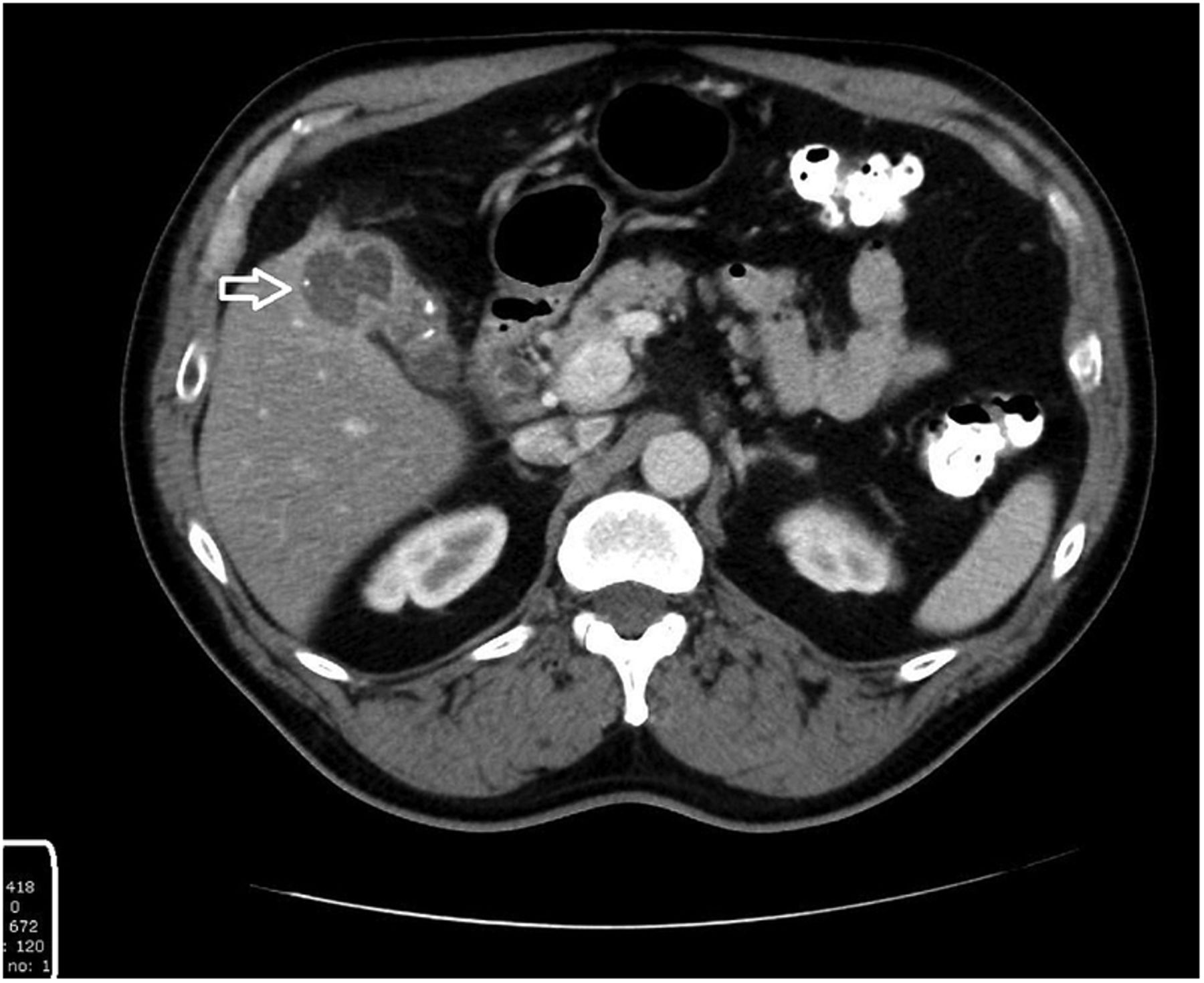
A 55-year-old man from Guam, with medical history significant for difficult-to-control hypertension, but without coronary artery or pulmonary disease, presented to our medical establishment for further evaluation and treatment for abdominal pain that had been present for 1 year. During this time, he denied fevers, chills or night sweats. He maintained a good appetite with no recent weight changes. When seen by his primary care provider in Guam, an ultrasound of the abdomen was ordered, which suggested cholelithiasis. There was associated gallbladder thickening that was suspicious for malignancy. A CT scan found an incidental nodule on the adrenal gland, but confirmed findings from the ultrasound (figure 1). The patient was therefore transferred to our institution for further evaluation. CT imaging was repeated, and showed interval worsening of the gallbladder wall with common bile duct enlargement. The working diagnosis included chronic cholecystitis and carcinoma. While he was awaiting further work-up, he came to the emergency room with worsening and persistent abdominal pain, nausea and vomiting after eating breakfast. The patient's medical history revealed hypertension with no history of coronary artery or pulmonary disease. His prior surgeries included a haemorrhoidectomy with no reported complications. He denied any medication or seasonal allergies. He was a chronic smoker, admitting to ½ to 1 pack a day for the past 20 years. He denied chronic alcohol use but did drink 1–2 beers socially on the weekends. Family history was negative for malignancy, pregnancy complications. Vital signs in the emergency room revealed a blood pressure of 145/81 mm Hg, otherwise unremarkable. Physical examination was notable for a minimally distended, firm abdomen, with tenderness to palpation in the right upper quadrant with positive Murphy's sign. No jaundice or scleral icterus was noted. An MR cholangiopancreatography that was ordered for evaluation of the biliary tree and gallbladder revealed an irregularly thickened heterogeneous wall with multiple echogenic layering foci within the gallbladder and proximal common duct, with a 1.5 cm stone observed.

CT of the abdomen and pelvis with oral contrast revealing abnormal lobulated contour and thickening of the gallbladder and cystic duct, with heterogeneous enhancement noted in the thickened gallbladder wall. Multiple peripherally dense intraluminal objects in the lumen representing gallstones.
He was scheduled and had both an endoscopic ultrasound (EUS) and ERCP performed the following day.
In the operating room, induction of anaesthesia and intubation were performed without complications. The EUS was first performed with the patient on his side, and no complications occurred. The common bile duct was dilated to 9 mm and contained numerous mobile hyperechoic foci with posterior shadowing consistent with choledocholithiasis. He was then repositioned into a semiprone position, and an ERCP was performed. A cholangiogram was performed and showed evidence of filling defects consistent with common bile duct stones (figure 2). After the major papilla was identified (figure 3), a sphincterotomy was performed using a standard sphincterotome (figure 4) followed by balloon extraction of multiple pigmented and cholesterol stones (figures 5 and 6). Repeat occlusion cholangiogram showed successful resolution of previously noted filling defects (figure 7).
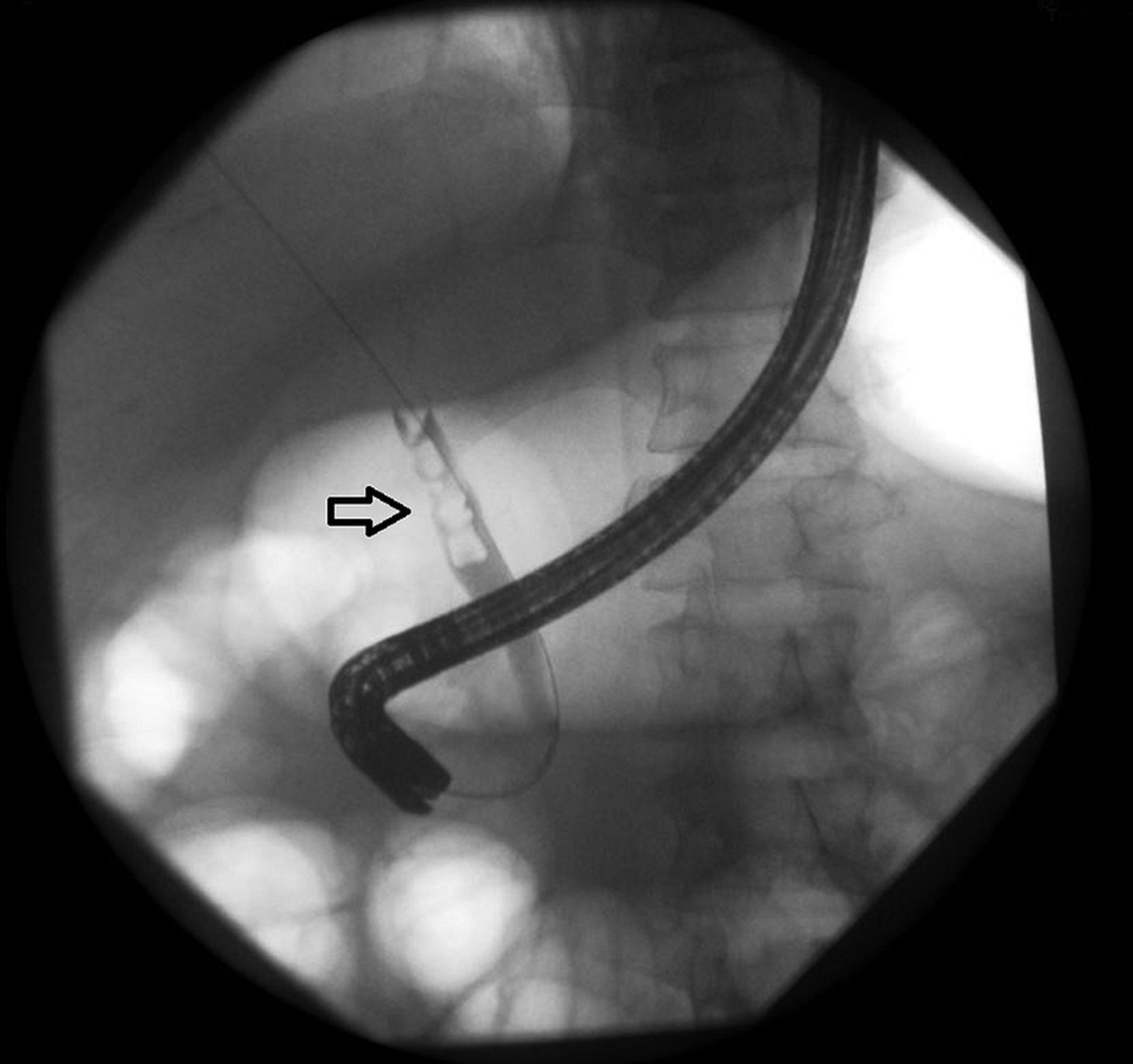
Cholangiogram revealing areas of filling defect of the common bile duct consistent with stones.

Intraoperative view of major papilla.

Intraoperative view of sphincterotomy.

Pigmented stone removed during endoscopy.

Cholesterol stone removed during endoscopy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Occlusion cholangiogram showing successful removal of previously noted stones.
While in the process of transitioning to choledochoscopy for planned direct visualisation of the biliary tree for further evaluation of the noted mass on prior imaging, the patient became hypotensive (50/30 mm Hg) with a concurrent drop in his EtCO2. Advanced cardiac life support was initiated when the patient was found to have no pulse or spontaneous breathing. During cardiopulmonary resuscitation, the patient's abdomen was noted to be significantly distended, and caused concern for intra-abdominal pathology. An orogastric tube was inserted to decompress the stomach and the general surgery department was consulted. An exploratory laparotomy was performed and showed no evidence of perforation, intra-abdominal bleed, no retroperitoneal haematoma. Examination of the chest was facilitated through a 5th ICS incision to expose the pericardium. The heart was full, but without motion. A left ventricular aspiration was performed to rule out air embolism and revealed frothy blood. Cardiac massage was initiated, and intracardiac epinephrine was administered without success. Time of death was called shortly thereafter.
Review of autopsy results showed evidence of a pulmonary air embolism as the ultimate cause of death, as during autopsy, bubbles were found in the pulmonary artery when it was incised under fluid.
Review
When performing an ERCP, the abdomen is insufflated with air to allow for optimal visualisation which provides the source for embolism formation.
Air embolisms can occur with any endoscopic procedure (to include esophagogastroduodenoscopy, enteroscopy, colonoscopy) and while Donepudi and colleagues reported 41 cases following various endoscopic procedures, Wills-Sanin described 27 cases, subsequent to ERCP, as of 2014.1 ,3 They occur when a communication between air and the vasculature is created that, given favourable pressure gradients, allows for air to enter either the venous or arterial circulation. Through the venous circulation, if the embolism is large enough, it may lodge in the pulmonary artery resulting in a limitation of blood flow leading to reflex vasoconstriction, increased pulmonary resistance, and finally elevated right ventricular pressures causing a decrease in cardiac output. The air itself may also have a proinflammatory response causing endothelial damage resulting in pulmonary oedema and hypoxia.4
Owing to its high rate of mortality (upwards of 40%), it is pivotal to recognise the associated clinical signs and symptoms of the condition. Prior biliary surgical interventions, blunt trauma to the liver, gastric ulcer disease, and inflammation of the digestive system are a few of the many risk factors one must be aware of that can predispose a patient to this condition.1 ,5 When undergoing interventional procedures, such as an ERCP, multiple mechanisms of air entry into the systemic vasculature are present to include intramural dissection to the portal vein and biliary-venous fistulas.1
If an embolism is suspected, a concurrent echocardiography should be performed to determine whether the foramen ovale is patent, as this can lead to a paradoxical embolism.6
High-flow oxygen is the specific treatment and should be started without delay to reduce the bubble size along with volume expansion, positioning in left lateral decubitus position and Trendelenburg, and direct aspiration of air from affected cardiac cavities if possible. Urgent hyperbaric oxygenation therapy (HBOT), atmospheric pressure of at least 2.5 for 2 h may maintain oxygen supply to ischaemic tissues while reducing the intracranial hypertension, and the most favourable neurological results are obtained when HBOT is initiated quickly.6 ,7 The patient's survival and functional prognosis depend directly on rapid diagnosis and treatment.
There have been increasing numbers of case reports regarding this known complication possibly secondary to its increasing recognition within the field.8 ,9 Of the 29 individual case reports encompassing patients between the ages of 8 and 82 years, 14 were fatal. Of the patients who went into cardiopulmonary arrest, only two survived.10 Major risk factors include prior interventions or surgeries of the biliary tract, along with air insufflation directly into the bile duct.11
A review by Finsterer et al7 describes multiple proposed mechanisms for this condition. One theory is that when air is insufflated into the abdomen, it is believed that air is introduced into the portal vein during the sphincterotomy given its anatomical location which is parallel to the biliary tree. Others focus on the bile duct wall and irritation by both the instrument and pressure exuded by air insufflation resulting in the introduction of air at the microscopic level to the surrounding veins.
While this case resulted in an air embolism to the pulmonary artery, systemic embolism resulting in cerebral emboli has been seen in multiple case reports, many of which have been fatal.12 ,13 As a result, some researchers have proposed further investigation as to whether patients would benefit from evaluation for a right-to-left shunt (PFO) prior to undergoing an ERCP.1
In our patient, air was found in both the pulmonary vein and suggested to be present in the right ventricle due to the frothy aspirate noted during the code. These findings were similar to those found by Finesterer et al on review of autopsy findings from two of the fatal case reports.13
As in this case, diagnosis of an air embolism can be established if air is visible in the portal vein, hepatic veins, or any chambers of the heart. Treatment is based on the severity of the patient's presentation, ranging from conservative measures to life-saving interventions including volume expansion, Trendelenburg positioning, and removal of air either through direct aspiration or hyperbaric treatment.7
As a result, it has been proposed whether insufflation with CO2 would decrease the risk of embolism.7 While CO2 can be expired through respiration, accumulations have the potential to lead to respiratory acidosis, but multiple studies showed that CO2 remained within physiologically accepted levels, therefore, there were no significant occurrences of respiratory acidosis.10 Owing to the high water solubility of CO2, it is thought to have lower risks of complications in comparison with room air, however, no formal prospective or retrospective studies comparing the two in regards to the incidence of air embolism have been performed.14
Potential complications from ERCP, other than air embolism have been reported, the most common of which is pancreatitis which has been reported in up to 15.7% of cases (table 1).15 ,16 While it is not uncommon to see transient elevations in pancreatic enzyme levels, the consensus defines post-ERCP pancreatitis as a clinical picture consisting of new or worsening abdominal pain requiring hospitalisation for 2 or more days, with an amylase level three times the upper limit of normal 24 h after the procedure concludes.17 Aside from pancreatitis, haemorrhage, perforation and infection have been described.
Commonly reported complications post-ERCP
Conclusion
Endoscopy is becoming a popular, minimally invasive option for gastroenterologists in the diagnosis and treatment of multiple gastrointestinal disorders. When undergoing more invasive interventional procedures such as an ERCP, endoscopic mucosal dissection, or large polypectomy, there can be multiple potential mechanisms of air entry into the systemic vasculature, and are present to include intramural dissection to the portal vein and biliary-venous fistulas.1 An under-recognised complication thought to occur specifically from air insufflation is air embolism. Owing to its high rate of mortality, it is pivotal to recognise the associated clinical signs and symptoms of the condition. Diagnosis can be established if air is visible in the portal vein, hepatic veins, or any chambers of the heart. Treatment ranges from conservative measures (Trendelenburg positioning, hyperbaric treatment) to life-saving interventions including direct aspiration.7 It has been proposed whether insufflation with CO2 rather than O2 would decrease the risk of embolism. While no randomised controlled trials comparing both techniques exist, hospitals around the world have adopted CO2 insufflation rather than room air in an attempt to decrease occurrences of embolism in patients undergoing more invasive endoscopic procedures. Ultimately, early diagnosis through better understanding of the signs and symptoms of this potential complication may decrease the delay in treatment and mortality.
References
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.