Article Text

Abstract
Objective Ascites in patients with decompensated cirrhosis can lead to abdominal distention and decrease quality of life. Tolvaptan, a vasopressin V2 receptor antagonist, is an effective agent in the treatment of ascites, whereas some patients are refractory to tolvaptan. The efficacy of transjugular intrahepatic portosystemic shunt (TIPS) for these patients is not known. In this study, we performed TIPS for tolvaptan-refractory cirrhotic patients and analysed its efficacy and safety in these patients.
Design This retrospective analysis included patients with liver cirrhosis who received TIPS for ascites or hydrothorax refractory to tolvaptan therapy along with conventional diuretics between January 2015 and May 2018 at Tokai University Hospital. We evaluated the efficacy and safety of TIPS.
Results This study included four patients. All patients presented with Child-Pugh class B liver cirrhosis and model for end-stage liver disease-sodium scores were 10/12/14/16. TIPS was generated successfully without any major complications in all patients. The body weight decreased by a mean of 4.7 (SD=1.0) kg and estimated glomerular filtration rate improved from a mean of 38.2 (SD=10.3) to 59.5 (SD=25.0) mL/min/1.73 m2 in a month after TIPS procedure.
Conclusion TIPS is an effective potential treatment for ascites in patients with tolvaptan refractory condition. In appropriate patients who can tolerate TIPS, the treatment may lead towards renal function improvement.
- LIVER CIRRHOSIS
- PORTAL HYPERTENSION
- INTERVENTIONAL RADIOLOGY
- ASCITES
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Tolvaptan, a vasopressin V2 receptor antagonist, is an effective agent in the treatment of refractory ascites in cirrhosis, whereas some patients are refractory to tolvaptan.
WHAT THIS STUDY ADDS
This study found that transjugular intrahepatic portosystemic shunt (TIPS) is an effective potential treatment for ascites in patients with tolvaptan refractory condition.
The effect of TIPS reduced diuretics and may lead towards renal function improvement in these patient.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Although next-line treatment options for ascites in tolvaptan-refractory cases are limited, TIPS is a treatment option in appropriate cirrhotic patients.
Introduction
Ascites is a common symptom of decompensated cirrhotic patients and significantly impairs the quality of life due to abdominal distention. Ascites appears in approximately 5%–10% of compensated cirrhotic patients per year.1 Refractory ascites (RA), defined as ascites that does not recede by appropriate medical therapy such as salt restriction and diuretic therapy or recures shortly after large volume paracentesis (LVP),2 is associated with poor survival.3 According to the treatment guidelines for cirrhosis with RA issued by the American Association for the Study of Liver Diseases,4 the European Association for the Study of Liver diseases 5 and the Japan Society of Hepatology (JSH),6 7 additional therapy such as LVP with albumin infusion, cell-free and concentrated ascites refusion therapy (CART), peritoneovenous shunt, transjugular intrahepatic portosystemic shunt (TIPS) and liver transplantation should be considered.
TIPS is a well-established technique for reducing portal pressure and subsequently improves ascites.8 9 In addition, TIPS increases the cardiac output and decreases systemic vascular resistance, causing an effective reduction in circulating blood volume and improving renal perfusion.10 In clinical practice, TIPS can improve RA and prognosis,11 12 although success of TIPS creation depends on eligible patients and appropriate timing.13
Tolvaptan, a selective oral vasopressin V2 receptor antagonist, excretes water by inhibiting water reabsorption in the renal collecting tubule and exhibits diuretic activity without increase of electrolyte excretion. Tolvaptan has been used in clinical practice for hyponatraemia,14 15 heart failure16 and autosomal dominant polycystic kidney disease.17 In Japan, tolvaptan has been indicated for fluid retention in cirrhosis since September 2013, and its efficacy has been reported against RA.18 19 Guidelines from JSH recommend tolvaptan as a treatment option against RA. On the other hand, the efficacy of tolvaptan in cases of refractory fluid retention has been reported to be 50%–78%, and some cirrhotic patients do not respond to tolvaptan.20 As far as we know, RA cases who received TIPS after failure of tolvaptan therapy were very few. In this study, we investigated the efficacy and safety of TIPS in patients with RA who did not respond to tolvaptan.
Materials and methods
Patients and study design
We enrolled four consecutive patients with liver cirrhosis who received TIPS for RA or hydrothorax under tolvaptan therapy between January 2015 and May 2018 at Tokai University Hospital. These patients had received tolvaptan for RA that was poorly controlled by sodium restriction and administration of furosemide (≥20 mg/day) and spironolactone (≥25 mg/day), but their ascites did not control even with tolvaptan treatment and repeated LVP with albumin infusion and/or CART. Response to TIPS was defined as weight loss ≥1.5 kg on day 7 from baseline.21 We retrospectively analysed the background, drug history, laboratory data and clinical course until November 2022.
TIPS procedure
All TIPS procedures were performed by an experienced interventional radiologist using conventional technique.22 First, a 10-French sheath was placed via the right femoral artery, and superior mesenteric artery portography and coeliac angiography were performed. The position of the hepatic artery and portal vein was confirmed on coeliac arterioportography, and a catheter was advanced to the right hepatic artery corresponding to the right portal branch approximately 2 cm from the porta hepatis as a landmark. Next, a 4-French sheath was placed via the right jugular vein. The Rosch-Uchida transjugular liver access set (Cook Medical, Bloomington, Indiana, USA) was used to create portal vein access and the tract was dilated using a Mustang 8 mm balloon catheter (Boston Scientific Corporation, Marlborough, Massachusetts, USA). The use of stents and the choice of stent device were decided by the radiologist. Self-expanding bare nitinol stents such as Luminex×12 mm×6 cm (Bard Peripheral Vascular, Tempe, Arizona, USA), Luminex×12 mm×8 cm (Bard Peripheral Vascular), Zilver 635 10 mm×8 cm (Cook Medical, Bloomington, Indiana, USA) and Epic vascular stent 10 mm×8 cm (Boston Scientific, Marlborough, Massachusetts, USA) were implanted. The pressures of the portal vein, right atriumand central vein were measured using a pressure transducer system. The portosystemic pressure gradient (PSG) was determined as the difference between the pressures in the portal vein and in the right atrium. ΔPSG was calculated by the difference in PSGs before and at the end of TIPS creation. TIPS is currently not covered by national health insurance in Japan, thus, TIPS procedure was planned and performed with sufficient informed consent.
Results
Clinical characteristics
TIPS was performed in four patients with RA who did not respond to the addition of tolvaptan to the existing diuretics such as furosemide and spironolactone. General characteristics in the patients are described in table 1. Aetiology of liver diseases were hepatitis C virus, alcoholic liver disease, non-alcoholic steatohepatitis and sarcoidosis, one by one. All patients presented with Child-Pugh class B liver cirrhosis. Model for end-stage liver disease-sodium (MELD-Na) scores were 10/12/14/16. Concomitantly used diuretics were furosemide at doses of 20–80 mg, spironolactone at doses of 25–200 mg and tolvaptan at a dose of 7.5 mg. Figure 1 shows CT images of ascites and pleural effusion before TIPS.
Clinical characteristics of the patients
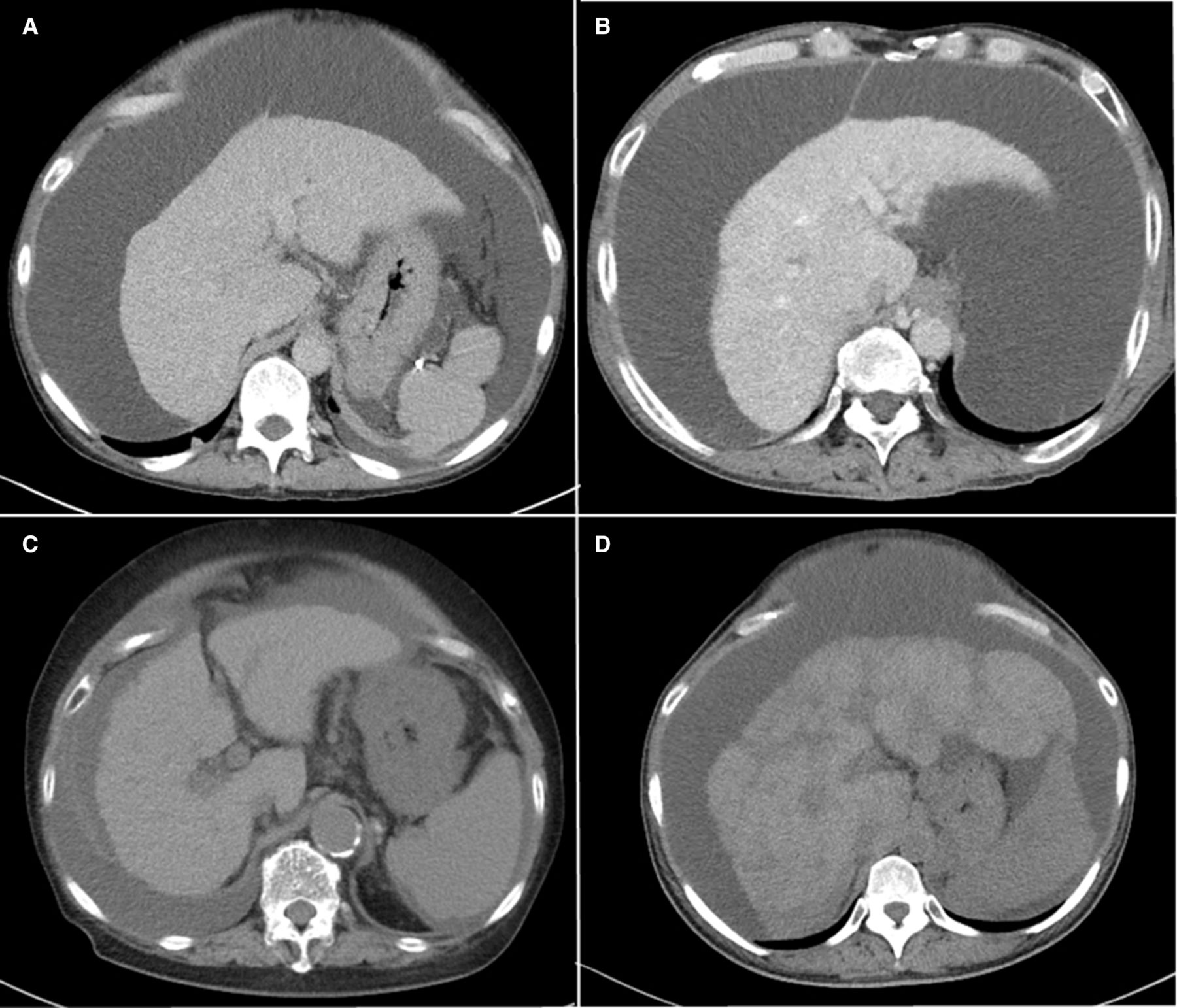
Abdominal computed tomography scan images before TIPS creation. (A) Case 1, (B) case 2, (C) case 3 and (D) case 4. TIPS, transjugular intrahepatic portosystemic shunt.
TIPS clinical efficacy against ascites and complication
TIPS was successfully created in all patients. The PSG decreased from a mean of 17.5 (SD=3.1) to 8.8 (SD=3.3) mmHg. All patients achieved response to TIPS along with the decrease in body weight by 4.7 (SD=1.0) kg in 1 month (table 2). As shown in figure 2, ascites and pleural fluid receded in all patients. The patients were prophylactically given rifaximin and hepatic encephalopathy was not observed. There were no deaths within the 30 days and no apparent complications associated with TIPS.
Clinical course and outcome of the patient

{kind=link}
{kind=link}
Abdominal computed tomography scan images post TIPS creation. (A) Case 1, (B) Case 2, (C) case 3 and (D) case 4. TIPS, transjugular intrahepatic portosystemic shunt.
Renal function and diuretic dose post-TIPS procedure
In 1 month after TIPS procedure, the estimated glomerular filtration rate (GFR) improved in all patients with the increase from a mean of 38.2 (SD=10.3) to 59.5 (SD=25.0) mL/min/1.73 m2. Diuretics were adjusted after TIPS procedure due to improvement in fluid retention. Subsequently, in the outpatient setting, tolvaptan was continued in all patients, while the doses of furosemide were reduced (table 2).
Mortality outcomes
Case 3 died of pneumonia; 83 days after TIPS, and case 1 died of unexplained sudden death; 112 days after TIPS. While, other two patients survived under ascites control.
Discussion
The first treatment for fluid retention in cirrhosis is salt restriction followed by conventional diuretics such as spironolactone and loop diuretics.6 7 Increasing doses of diuretics such as furosemide activates the sympathetic nervous system and renin–angiotensin–aldosterone (RAA) system, decreases GFR and raises the risks of renal impairment, electrolyte abnormalities and sarcopenia.23 24 High furosemide administration doses may also decrease renal interstitial osmolarity, leading to refractoriness against tolvaptan.25 Tolvaptan exerts its action independently of serum albumin concentration and does not reduce the renal blood flow and GFR because it does not affect RAA system.25–27 There are also reports that the use of tolvaptan reduced furosemide doses in cases of chronic kidney disease stages 3–4.28 According to the JSH cirrhosis guidelines,6 7 from the viewpoint of preventing deterioration of renal function early add-on administration of tolvaptan is recommended for patient who are resistant to conventional diuretics such as spironolactone (25–50 mg/day) and furosemide (20–40 mg/day). In cases of ascites refractory to conventional diuretics, tolvaptan induction has been shown to be more effective than increasing the dose of furosemide.29 On the other hand, factors prior to tolvaptan induction such as high blood urea nitrogen value,30 low serum natrium value31 and decreased liver function (based on high Child-Pugh score)32 are predicted to decrease response to tolvaptan treatment.
Treatment for RA includes TIPS, serial LVP plus albumin infusion, PV shunts, low-flow ascites pumps and liver transplantation. TIPS is an endovascular operation which is performed to create an intrahepatic tract between the hepatic and portal veins and can reduce the portal pressure. Compared with serial LVP, TIPS reduced the relapse of symptoms due to ascites and improves transplant-free survival.33 Selection of eligible patients is important for the success of TIPS creation. Child-Pugh class C,34 MELD score greater than 18,35 advanced age,33 cardiopulmonary insufficiency or sarcopenia36 37 have a high risk for complications of TIPS creation. In addition, Bureau et al reported serum bilirubin value below 50 µmol/L and a platelet count above 75×109/L is predictive of survival in patients with RA treated with TIPS.38 In this study, all patients were Child-Pugh grade B, MELD score was less than 18, and serum bilirubin and platelet count were within above criteria, indicating appropriate patient selection. We do not derive the exact mechanisms why these four patients responded to TIPS well. However, TIPS might be as effective in the tolvaptan-refractory patients as in the patients with RA as long as they fit the eligibility criteria of TIPS described above.
The larger diameter-stent can more reliably achieve the target hepatic venous pressure gradient. Whereas excessive shunting may induce hepatic dysfunction due to reduced effective hepatic blood flow and the development of encephalopathy. Therefore, it is important to select the appropriate diameter of the stent to balance the efficacy and complications of TIPS.39 A comparative study of 8 mm and 10 mm diameter stents showed no difference in the development of hepatic encephalopathy, but control of complications due to portal hypertension was superior with the 10 mm diameter stent.40 41 In this study, the stents used for two patients in TIPS placement were 10 mm and 12 mm each, which were effective in improving ascites and did not cause any hepatic encephalopathy or dysfunctions. This discrepancy is attributed to bare stents used in our country as different from a more popular stent-graft in Western countries. Because of more frequent restenosis of bare stents in TIPS, bigger stent diameters tends to be selected in our hospital.
This study shows, for the first time, the therapeutic results of TIPS in a patient refractory to tolvaptan with effective results. The effect of TIPS and the controllable ascites showed that renal function improved in this patient after TIPS due to the diuretics reduction, especially furosemide. Our study has limitations. This study is a retrospective, single-centre study with a small number of patients, which will include selection bias. The accumulation of cases is necessary to evaluate the safety and efficacy of TIPS in these patients. Next-line treatment options for ascites in tolvaptan-refractory cases are limited, but TIPS is a promising treatment option in appropriate cases. In conclusion, TIPS was clinically successful in the treatment of RA in tolvaptan-refractory patients.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This research was conducted with the approval of the Ethics Review Board of the Tokai University School of Medicine (No. 21R-174) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all patients.
References
Footnotes
Contributors KT conceived the idea of the study. JK, YS, SO, TS, and TH contributed to the diagnosis and the treatment including the TIPS procedure. KT, YM, YA, SH, KS, and TK contributed the clinical management of the patients. KT, JK, and TK drafted the original manuscript. All authors critically reviewed and revised the manuscript draft and approved the final version for submission. KT is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.