Article Text

Abstract
Objective Although appendiceal cancer remains a rare gastrointestinal malignancy compared with colorectal cancer, incidence rates of appendiceal cancer have increased in the last two decades. Appendiceal and cecal adenocarcinomas have distinct genomic profiles, but chemotherapy protocols for these malignancies are the same and survival outcomes between them have not been compared extensively. To this end, we conducted a comparative survival analysis of appendiceal and cecal adenocarcinomas.
Design Using the Surveillance, Epidemiology and End Results (SEER) database, we identified individuals ≥30 years of age with appendiceal or cecal adenocarcinoma from 1975 to 2016. Demographic, clinical and county-level socioeconomic data were extracted using SEER*Stat software. Survival was compared by Mantel-Haenszel log-rank test, and survival curves were generated using the Kaplan-Meier method. Relative HRs for death in the 5-year period following diagnosis were calculated using multivariable Cox regression analysis, adjusted for all other covariates. The significance level was set at p<0.05 for two-tailed tests. Data were analysed using SAS V.9.4 and R software.
Results We identified 6491 patients with appendiceal adenocarcinoma and 99 387 patients with cecal adenocarcinoma. Multivariable Cox regression analysis demonstrated significantly higher cancer-specific and overall survival in appendiceal adenocarcinoma compared with cecal adenocarcinoma. Male sex, older age, earlier year of diagnosis, black race, single marital status, non-Hispanic ethnicity, and non-mucinous histology were associated with increased mortality rates. In addition, counties with lower percentage of individuals below the poverty line and higher colorectal cancer screening rates had better survival.
Conclusion This is the first study to show greater survival in appendiceal adenocarcinoma compared with cecal adenocarcinoma. We also highlighted novel associations of county-level socioeconomic factors with increased mortality in appendiceal adenocarcinoma. Future efforts to develop targeted molecular therapies and reduce socioeconomic barriers to diagnosis and treatment are warranted to improve survival.
- CANCER
- APPENDIX CARCINOMA
- COLORECTAL CARCINOMA
- CANCER EPIDEMIOLOGY
- EPIDEMIOLOGY
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Survival differences between appendiceal and colorectal cancers have not been well studied.
WHAT THIS STUDY ADDS
This is the largest comparative survival study of appendiceal and colorectal cancers, and the first to show that appendiceal adenocarcinoma is associated with improved survival compared with cecal adenocarcinoma. We also identified novel socioeconomic factors associated with appendiceal adenocarcinoma mortality at a countywide level.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study highlights the need for additional investigation of the unique molecular mechanisms and potential therapeutic targets underlying appendiceal malignancies as well as socioeconomic barriers to diagnosis and treatment critical to identifying individuals at risk for worse survival outcomes.
Introduction
Although appendiceal malignancies are rare, their incidence in the USA has steadily increased in the past two decades to 1–2 per million person-years despite stable rates of appendectomies.1–3 Previous large population-based studies have identified key demographic and clinical prognostic factors associated with survival in patients with appendiceal malignancies, including age, race, marital status, histological type, tumour stage, tumour grade, lymph node resection, chemotherapy and surgical intervention.1 4–10 These variables have been used to construct prognostic nomograms that predict overall mortality and disease-specific survival.11 12
Recent molecular profiling studies have provided novel insights into the genetic underpinnings of appendiceal cancer.13–16 Genetic heterogeneity exists among different histological types of appendiceal tumours, including mucinous adenocarcinoma (MAC), non-MAC (NMAC), signet-ring cell carcinoma (SRCC), goblet cell carcinoid and pseudomyxoma peritonei. In addition, although the appendix is embryologically derived from the cecum, appendiceal and colorectal cancers (CRC) have distinct genetic profiles.14–16 These discoveries are notable given that no standard chemotherapy guidelines exist specifically for advanced appendiceal cancers unamenable to surgery, which are currently treated with CRC chemotherapy protocols.17 18
The incidence rate of CRC at 25–30 per 100 000 person-years is much higher than that of appendiceal cancer, although it has declined over recent years due to an increased uptake in CRC screening and risk factor modifications such as smoking, diet and physical activity.19 While the incidence trend of cecal adenocarcinoma itself is not detailed in the literature, cecal tumours are estimated to account for 20% of CRC cases.20 Recent genomic studies have also demonstrated that CRC tumour location is associated with differences in molecular alterations. For example, cecal adenocarcinoma carries a higher frequency of KRAS mutations compared with non-cecal right-sided colon adenocarcinoma.21
Despite differences in genetic profiles, survival outcomes between appendiceal and colon cancer have not been compared extensively. One retrospective study showed that 5-year disease-free survival rates were lower in appendiceal adenocarcinoma than in colon adenocarcinoma.22 However, these findings excluded metastatic cases and were limited by a small sample size of appendiceal malignancies, precluding consideration of important demographic, clinical and socioeconomic factors. To this end, we conducted a comparative survival analysis of appendiceal and cecal adenocarcinomas using US survival data from the Surveillance, Epidemiology and End Results (SEER) database.
Methods
We used the SEER database (https://seer.cancer.gov/) to identify individuals aged 30 years or older diagnosed with appendiceal or cecal adenocarcinoma from 1975 to 2016. Demographic, clinical and county-level socioeconomic data were extracted using SEER*Stat software. Demographic covariates included sex, age at diagnosis, year of diagnosis, race, ethnicity and marital status. Clinical data consisted of primary cancer site, tumour histology, tumour stage, tumour grade, surgery, chemotherapy and survival. County-level socioeconomic data included population percentages of the following: smokers, college education, minority, urban, foreign-born, below the poverty line and CRC screening adherence.
Survival curves were generated using the Kaplan-Meier method, and survival was compared by the Mantel-Haenszel log-rank test. Relative HRs for death in the 5-year period following diagnosis were calculated using multivariable Cox regression analyses, adjusted for all other covariates. The level of significance was set at p<0.05 for two-tailed tests. Data were analysed by using SAS V.9.4 and R software.
Results
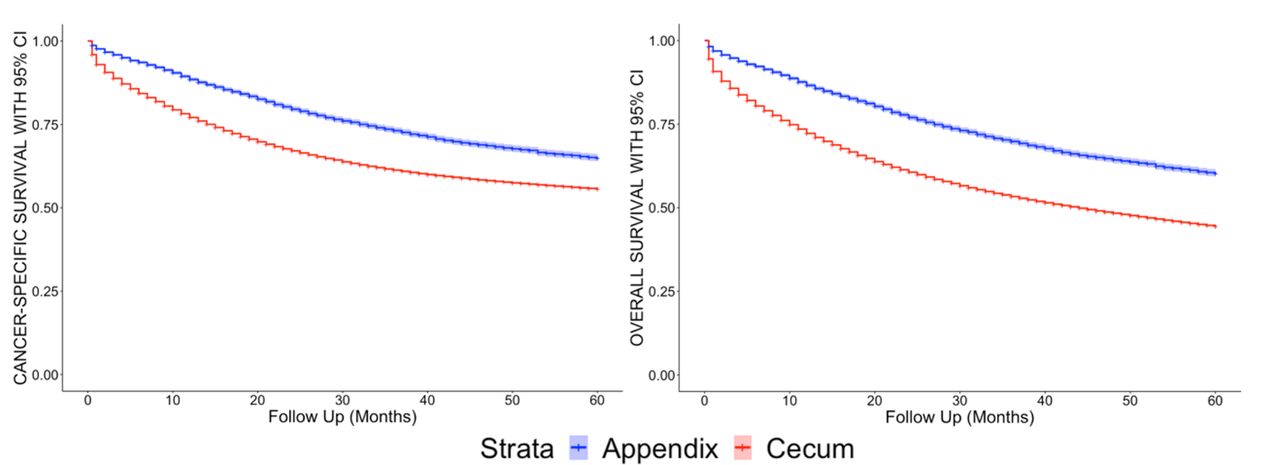
Our study consisted of 6491 appendiceal adenocarcinoma cases with 3602 MACs, 2235 NMACs, and 654 SRCCs, and 99 387 cecal adenocarcinoma cases with 13 136 MACs, 84 812 NMACs and 1439 SRCCs from the SEER database. Distributions of demographic and clinical data for each type of malignancy are provided in online supplemental table 1. The 5-year cancer-specific and overall survival curves for appendiceal and cecal adenocarcinomas are shown in figure 1.
Supplemental material

{kind=link}
Five-year cancer-specific and overall survival for appendiceal and cecal adenocarcinomas.
Multivariable Cox regression analyses were conducted to assess independent associations of demographic, clinical and county-level socioeconomic covariates with 5-year cancer-specific mortality rates (table 1) and overall mortality rates (online supplemental table 2) adjusted for all other covariates. Compared with cecal adenocarcinoma, appendiceal adenocarcinoma had better cancer-specific (HR 0.71; p<0.001) and overall survival (HR 0.71; p<0.001). Male sex, older age, earlier year of diagnosis, black race and non-Hispanic ethnicity were significantly associated with higher mortality. Those who were divorced, never married, widowed or with domestic partners had worse survivorship compared with married individuals. With regard to clinical characteristics, NMAC was associated with worse survival than MAC but improved survival compared with SRCC. Advanced tumour stage (HR 14.06; p<0.001) and grade (HR 2.31; p<0.001) exhibited higher mortality, as did lack of surgical intervention (HR 2.88; p<0.001). Lack of chemotherapy was significantly associated with worse overall survival (HR 1.10; p<0.001) (online supplemental table 2) but not cancer-specific survival (HR 1.00; p=0.05) (table 1). In addition, we analysed associations of county-level socioeconomic factors with survival and found improved survival in counties with lower percentage of individuals below the poverty line (HR 1.06; p=0.0002) and higher CRC screening rates (HR 0.94; p<0.001). Smoking, college education, percentage of minority population, percentage of urban population and percentage of foreign-born population were not associated with mortality risk at a county level.
Demographic, clinical and county-level socioeconomic factors associated with 5-year cancer-specific survival in appendiceal and cecal adenocarcinoma using multivariable Cox regression analysis
Discussion
In this largest comparative survival study of appendiceal and cecal cancers to date, we demonstrated that appendiceal adenocarcinoma is associated with improved survival outcomes compared with cecal adenocarcinoma. To our knowledge, only one other study has investigated differences in mortality between appendiceal and colon cancer.22 In contrast to our findings, Son et al found that 5-year disease-free survival was lower in appendiceal adenocarcinoma, perhaps in part due to a higher perforation rate associated with appendiceal tumours. This disparity may be explained by differences in study design as their analysis consisted of a smaller sample size of appendiceal tumours (n=47 compared with n=6491 in our study), measured disease-free survival rather than overall or cancer-specific survival, included only patients with appendiceal adenocarcinoma who underwent curative resection, and excluded metastatic disease. In addition, while Son et al included both proximal and distal colon adenocarcinomas, we limited our analysis to cecal adenocarcinoma given the close anatomical proximity to the appendix and their shared embryonic origin from the cecal diverticulum.22
Lower mortality rates associated with appendiceal adenocarcinoma may be related to differences in initial clinical presentation and tumour molecular profiles. Although the incidence of appendiceal cancer observed in appendectomies is rare, almost one-third of appendiceal cancer cases present as acute appendicitis,23 which may prompt early surgical resection leading to better prognosis compared with cecal cancer. In addition, recent genomic profiling studies have shown differing genetic mutation frequencies between appendiceal and colon cancers.14–16 Appendiceal tumours exhibit higher mutation rates in KRAS and GNAS and lower mutation rates in TP53, APC and PIK3CA compared with colon tumours. Differences in molecular characteristics also exist among various histological types of appendiceal adenocarcinoma. In particular, TP53 mutations are more commonly found in NMAC than in MAC, whereas MAC harbours a higher frequency of GNAS mutations.14 Given that TP53 mutations have been shown to be associated with worse overall survival compared with TP53 wild-type tumours and GNAS mutations are known to confer better prognosis relative to GNAS wild-type tumours,14 these differences in genetic mutation profiles may contribute to the improved survival observed with appendiceal cancer and MAC in comparison to cecal cancer and NMAC, respectively. Moreover, recognising these unique genomic features and their effects on downstream mechanistic pathways are critical to the development of future chemotherapy regimens tailored to treating appendiceal cancer.
Our study validated demographic and clinical factors previously reported to be associated with survival in appendiceal cancer in large population-based studies.4–9 Female sex, younger age, later year of diagnosis, white race and married marital status were significantly associated with lower mortality. Holowatyj et al previously reported that among individuals younger than 50 years of age diagnosed with appendiceal cancer, non-Hispanic black patients had poorer survival compared with non-Hispanic white and Hispanic patients.9 This was similar to our findings, where black race was associated with worse survival in appendiceal adenocarcinoma regardless of age, further suggesting interracial differences in key clinical and socioeconomic factors such as tumour molecular profiles and healthcare access. In addition, Hispanic individuals had improved survival compared with non-Hispanics, which has been previously reported in CRC but is a novel finding for appendiceal cancer.3 24 Similar to previous studies, we found SRCC had worse survival than both MAC and NMAC while MAC was associated with lower mortality compared with NMAC.1 10 Not surprisingly, advanced tumour stage and grade exhibited higher mortality rates, while surgical intervention was associated with improved survival. Chemotherapy was significantly associated with greater overall survival but not cancer-specific survival, raising the possibility that current chemotherapy protocols are inadequately targeting key molecular pathways by not accounting for differences in genomic profiles between appendiceal and colon cancers.
Socioeconomic factors related specifically to appendiceal cancer have not been studied extensively. One retrospective study of individuals with appendiceal cancer with peritoneal metastases found that those with low socioeconomic status, assessed via the area deprivation index, were less likely to receive cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion (CRS HIPEC) treatment.25 In addition, among patients who received CRS HIPEC, those with low socioeconomic status had worse overall survival.25 In our study, counties with higher percentage of individuals below the poverty line and lower CRC screening rates had a higher mortality risk. Given that CRC screening may serve as surrogate marker for income status as well as healthcare literacy and access, our findings highlight important socioeconomic factors that may lead to survival disparities.
We acknowledge several limitations of our study inherent to the SEER database, including its retrospective design limiting the inference of causality and lack of pertinent clinical data such as comorbidities, specific chemotherapy regimens and postoperative complications. Our study also included a larger sample size of cecal adenocarcinoma compared with appendiceal adenocarcinoma, although this is reflective of the substantially rarer incidence of appendiceal cancer. In addition, our association analyses of socioeconomic factors with survival involved county-level data, which precludes drawing definitive conclusions at the individual level. Nonetheless, our well-powered study, strengthened by the large number of cancer cases and extensive data collection period, demonstrated better prognosis associated with appendiceal adenocarcinoma compared with cecal adenocarcinoma. Further investigation of the unique molecular mechanisms and potential therapeutic targets underlying appendiceal malignancies as well as socioeconomic barriers to diagnosis and treatment is critical to identifying individuals at risk for worse survival outcomes.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study was exempt from obtaining informed consent as the SEER database is publicly available and patient data are deidentified.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GC conceptualised the project, assessed data and was the primary author in drafting and editing of the manuscript. KC and LS made substantial conceptual contributions, assessed data and edited the manuscript. SZ assessed data and edited the manuscript. PP managed the project, made substantial conceptual contributions, conducted statistical analysed, edited the manuscript and accepts full responsibility for the work as guarantor. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.