Article Text

Abstract
Objective Idiopathic hypercalciuria is characterised by renal stone formation and vertebral osteoporosis. The syndrome displays high clinical variability with patients almost equally distributed between fasting or renal type (prevalent calcium loss) and absorptive type (prevalent increase of intestinal absorption). Absorptive hypercalciuria (AH) is characterised by hypersensitivity of calcium-sensing receptors of antral G cells with normal fasting gastrinaemia and meal hypergastrinaemia. To the best of our knowledge, no study has been published about the morphological aspects of gastric biopsies of patients with AH and the immunohistochemical findings of gastrin-producing G cells. So we studied morphologically and immunohistochemically a group of 38 patients with AH, describing their gastric findings and associated lesion.
Design All 38 patients had a clinical-laboratory diagnosis of AH with normal fasting hypergastrinaemia and an abnormal rise of gastrinaemia after a standardised meal test. Their 38 antral and 27 body-fundus biopsies, and 5 normal antral and body controls, were stained with H&E, Giemsa stain, polyclonal antiserum anti-Gastrin and a monoclonal antibody anti-Chromogranin A.
Results Antral biopsies of all 38 patients showed a simple (15) or linear (23) hyperplasia of G cells, whereas only 2 of 27 body biopsies showed a nodular hyperplasia of endocrine cells. In five patients with AH, we found an association with fundic gland polyps (FGPs).
Conclusions We found in all of the patients with AH a correlation between meal hypergastrinaemia and morphological antral G-cell hyperplasia. Moreover, in five patients, AH was associated with FGPs. We know from literature data that FGPs’ development in Zollinger-Ellison syndrome is statistically associated with hypergastrinaemia. From our present data, we suggest that even in AH the stimulated hypergastrinaemia may have a role in polyp development.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Absorptive hypercalciuria (AH) is characterised by the hypersensitivity of calcium-sensing receptors of antral G cells.
▸ Patients with AH have normal fasting gastrinaemia and hypergastrinaemia stimulated by peptones and calcium.
▸ At present, no morphological and immunohistochemical studies on gastric biopsies of patients with AH have been published.
What are the new findings?
▸ Patients with AH showed morphological G-cell hyperplasia, independent from therapies or Helicobacter pylori infection.
▸ We found an unexpected association between AH and fundic gland polyps, with a 10-fold raised prevalence when compared with the general population, a difference extremely statistically significant.
How might it impact on clinical practice in the foreseeable future?
▸ It is to be elucidated if even in patients with sporadic fundic gland polyps, not treated with proton pump inhibitors, hypergastrinaemia may play a role.
▸ Alternatively, somatic β-catenin mutation of sporadic fundic gland polyps may stimulate G-cell hyperplasia.
Introduction
Idiopathic hypercalciuria is found in up to 40% of stone formers, but has an incidence of less than 10% in the overall population.1 The syndrome displays a large clinical variability with patients almost equally distributed between fasting or renal type (prevalent renal calcium loss) and absorptive type (prevalent increase of intestinal absorption).
Absorptive hypercalciuria (AH) is a clinical condition characterised by a large increase of calcium in the urine, formation of renal stones and osteoporosis in spite of normal levels in the blood. AH is characterised by hypersensitivity of calcium-sensing receptor (CaSR) of antral G cells, with normal fasting gastrinaemia and meal hypergastrinaemia.2 G-cell CaSR is the predominant chemosensor mediating gastrin secretion.3
To the best of our knowledge, there are no published data about the morphology and immunohistochemistry of gastric biopsies of patients with AH.
So we studied the gastric biopsies of a group of 38 patients with an established diagnosis of AH,2 analysing their morphology, immunohistochemical features and associated lesions.
Patients and methods
Criteria for patient selection were published elsewhere.2 All 38 patients had calcium urinary excretion higher than 250 mg/day (6.25 mmol/day, normal values, 2.5–6.25 mmol/day); they were on a free diet and were not taking calcium-sparing diuretics. After 1 month of a dietician-assisted calcium-free diet, they showed a reduction in daily calcium excretion (<100 mg/day or 2.5 mmol/day), and a decrease of calcium/creatinine values in fasting 2 h urine (<0.35 mmol Ca/mmol creatinine, normal values 0.1–0.2 mmol Ca/mmol creatinine), thus fulfilling the conventional criteria for AH diagnosis.
They were all free of severe dyspepsia, and none had taken antiacid therapy. Whereas fasting gastrinaemia was comparable to controls (60–70 ng/L), patients with AH responded to both the calcium load test (1 g calcium gluconate Calcium Sandoz fortissimo) and peptone load test (10 mg Liebig meal extract diluted in 250 mL of 0.9% saline) with an abnormal rise in gastrinaemia with almost doubling values when compared with controls.
The patients were referred to our institution with the principal aim of evaluating gastric antra and to find a possible correlation between meal hypergastrinaemia and the morphology of antral G cells.
Endoscopically, all patients did not show significant lesions, except for sparse antral microerosions or hyperaemia; in five patients, small body-fundic polyps were seen that were biopsied.
Five antral and body normal controls and biopsies, randomly taken from the antrum (in all 38 patients) and body-fundus (in 27 patients), plus the five body-fundus polyps were fixed in Bouin, embedded in paraffin, cut at 3 µ and stained with H&E and modified Giemsa. Helicobacter pylori were extensively searched for on modified Giemsa section at 40× on both antral and body biopsies. Further sections were cut for the immunohistochemical study of endocrine population using anti-Gastrin polyclonal antiserum (Dako), diluted 1:300 for 30′, room temperature, and an anti-Chromogranin A monoclonal antibodies cocktail (LK2H10 and PHE5 MoAbs, Neomarker) diluted 1:100 for 45′ room temperature. We used four normal antral and body-fundic biopsies as controls.
Enterochromaffine like (ECL) cells (Chromogranin A+) were scored according to Solcia et al.4
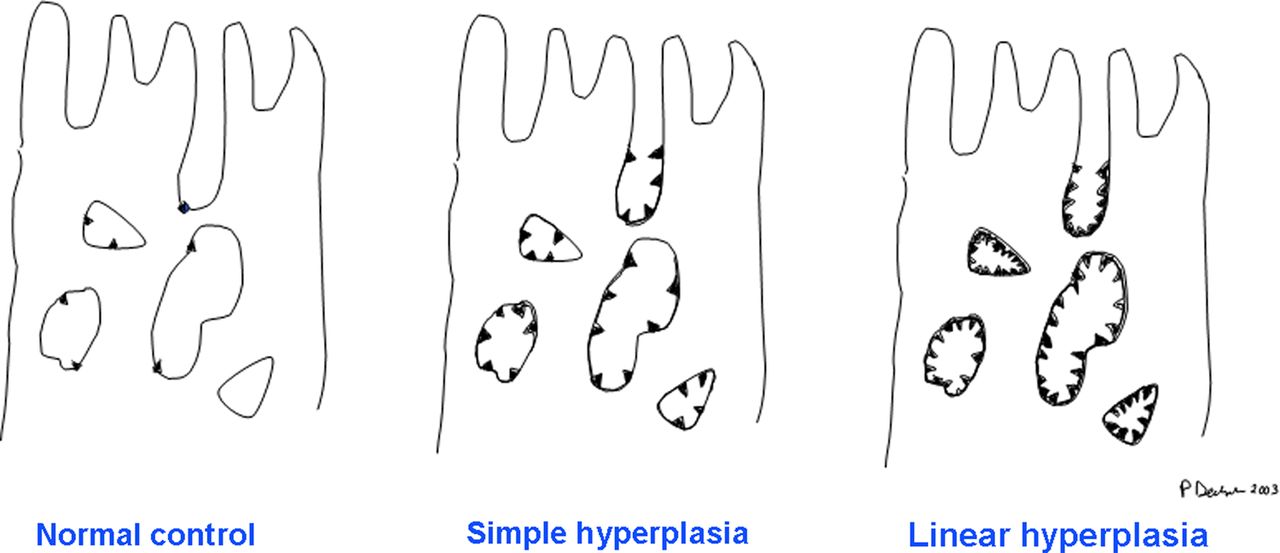
We scored antral G cells as follows:5 ,6
▸ Normal: 1–2 G cells for each gland, with uneven distribution;
▸ Simple hyperplasia: 4–5 cells for each gland;
▸ Linear hyperplasia: continuous chain-like distribution of G cells (figure 1).
In a subset experiment, we counted all gastrin-positive cells in controls, simple hyperplasia and linear hyperplasia, evaluating at least 20 well-oriented gastric pits-neck-glands. Results were compared unpaired t test, calculated using the internet resource at http://graphpad.com/quickcalcs/
Gastritis was assessed following the approach by Owen, distinguishing chronic active and quiescent, superficial and deep (under the neck region) gastritis, assessing the presence of H. pylori, atrophy and intestinal metaplasia.7
We used strict criteria for the diagnosis of fundic gland polyps (FGPs),8–11 that is:
▸ Shortened gastric pits;
▸ Presence of irregular dilations, both superficial and deep, bordered by all three cell types of body mucosa—mucous, parietal and chief cells.
All statistical analyses were performed using the GraphPad Quick calc resource at http://graphpad.com/
Results
Clinical features
Table 1 shows anatomical and clinical features of the 38 patients with AH. They were mostly female (F/M: 4.4/1), with a median age of 58.2 years.
Clinical features of the 38 patients with AH are resumed
At least an antral biopsy was performed in all the patients, and body-fundic biopsies in 27 patients. None of the patients had been treated with proton pump inhibitor therapy previously.
Histology
At first endoscopy, 26 patients showed active superficial gastritis with H. pylori colonisation. None of the 27 patients who had body-fundic biopsy showed atrophy or metaplastic change. Patients with H. pylori gastritis were treated with our standard eradication therapy (amoxicillin 1 g twice a day, clarithromycin 500 mg twice a day, omeprazole 20 mg twice a day, all drugs for 1 week). They underwent a second endoscopic examination with a mean interval of 20.6 months (minimum 4 to maximum 40 months). Their antral biopsies appeared H. pylori free with no residual significant inflammation.
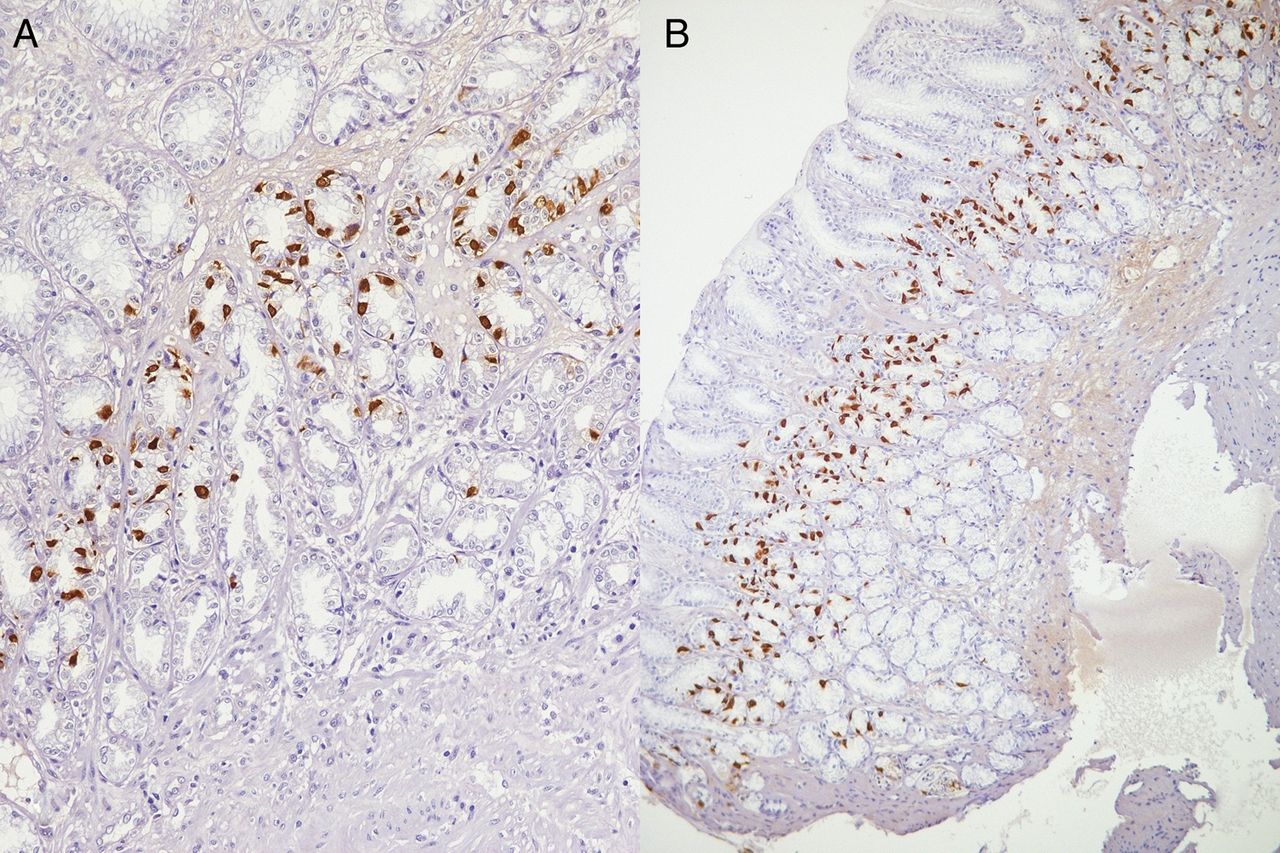
The immunohistochemical staining for gastrin was performed on 5 controls and 38 patients and repeated again after eradication on the 26 patients originally with gastritis. The G-cell score of the first examination and the second after eradication appeared unchanged, thus not being affected by H. pylori infection or proton pump inhibitors (PPI) therapy. The five controls showed normal G-cell values. All 38 patients showed a G-cell hyperplasia (simple in 15 and linear in 23; figure 2).The 12 patients, originally H. pylori free, showed simple hyperplasia in 4 cases and linear hyperplasia in 8 cases; the 26 patients, retested after H. pylori eradication, showed simple and linear hyperplasia in 11 and 15 cases, respectively. The different distribution of simple and linear hyperplasia between the patients originally H. pylori negative and patients eradicated, judged with Fisher's exact test, was not statistically significant (p=0.7281).

Simple (A) and linear hyperplasia (B) highlighted by immunohistochemical stain for gastrin ((A) gastrin antiserum, 10× original magnification; (B) gastrin antiserum, 4× original magnification).
Evaluating at least 20 well-oriented antral glands in controls, cases with simple and linear hyperplasia, mean G cells per gland were scored (table 2), and the differences were evaluated with an unpaired t test. The difference between controls and simple hyperplasia was extremely statistically significant (p=0.0003), whereas the difference between simple and linear hyperplasia was very statistically significant (p=0.0032).
The mean number of G cells per gland was scored in controls, simple and linear hyperplasia and the differences evaluated with unpaired t test were considered very statistically significant
While studying the 27 body-fundic biopsies with an anti-Chromogranin antibody, we detected a normal ECL cell distribution in 25 cases, and a micronodular hyperplasia in only 2 cases. In both of them, the micronodular body hyperplasia was associated with linear G-cell hyperplasia. No signs of atrophy or parietal cell hypertrophy were present in all biopsies.
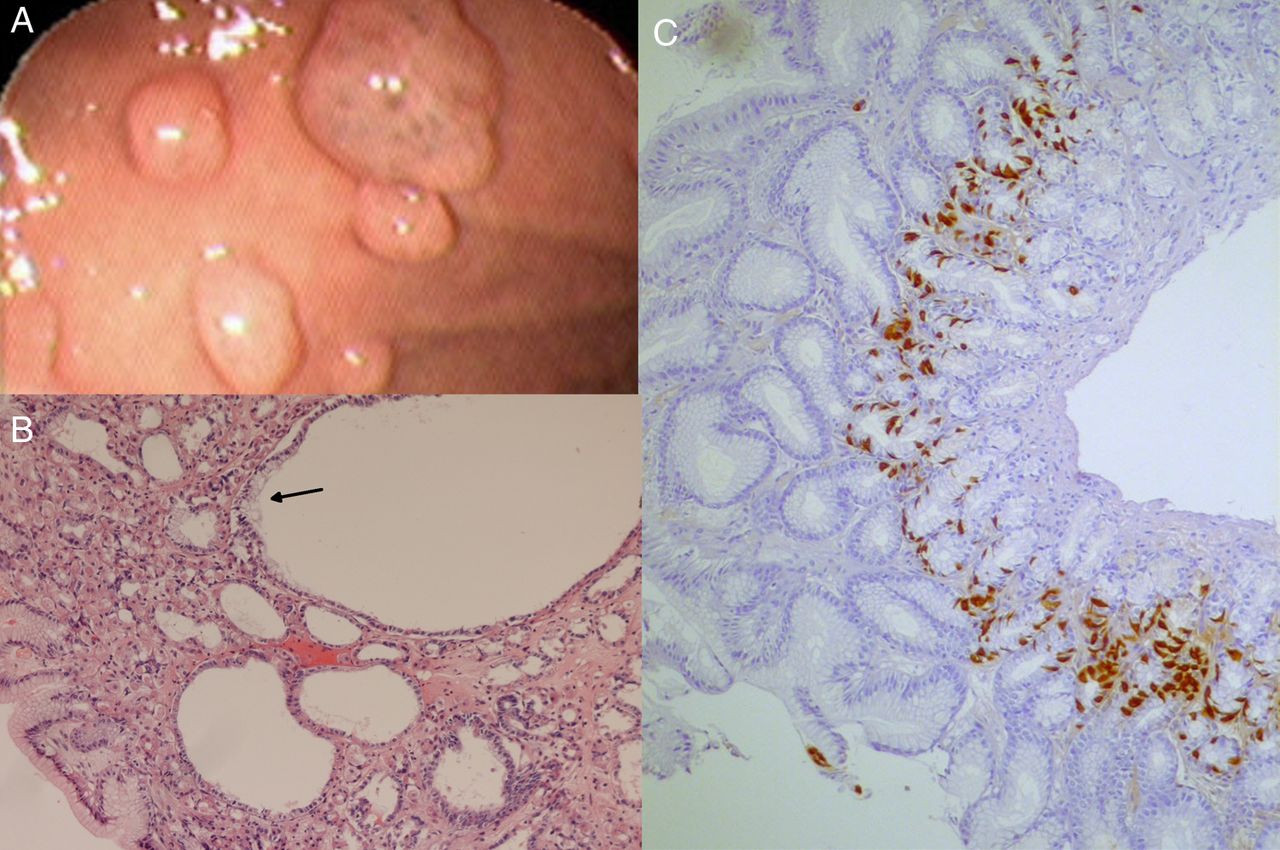
In five patients, we found an association with FGPs, that is, polyps characterised by shortened gastric pits and superficial and deep dilations bordered by mucous, parietal and chief cells (figure 3). No associated signs of parietal cell hypertrophy were seen, both in FGPs and in the 27 body-fundic biopsies. None of the polyps showed any sign of dysplasia.

{kind=link}
{kind=link}
{kind=link}
Tiny polyps covered by pink glistening mucosa in the body-fundus were apparent at endoscopy (A); histologically, they showed superficial and deep cystic dilation, covered by mucus (arrow), parietal and chief cells, diagnostic for fundic gland polyps (B); antigastrin immunostaining evidence a persistent linear hyperplasia after the Helicobacter pylori eradication (C) ((B) H&E, ×10 original magnification; (C) gastrin antiserum, ×4 original magnification).
Patient 1—A 59-year-old man, with antral active gastritis with H. pylori colonisation at the time of the first control, showed a normal body-fundic mucosa, without polyps or irregularities. Immunohistochemical stainings detected linear G-cell hyperplasia and a normal ECL cell population. On the next endoscopic control, 40 months after the eradication treatment, the gastric body presented some tiny sessile polyps (1–2 mm). The antral mucosa showed a mild hyperaemia H. pylori negative, and a persistent linear G-cell hyperplasia (figure 3).
Patient 2—A 59-year-old woman, with intense chronic active gastritis in the antral mucosa H. pylori positive, with simple G-cell hyperplasia associated to superficial active H. pylori positive gastritis in the body, normal endocrine population. The following posteradication control, 26 months after the first examination, detected a residual chronic quiescent H. pylori negative gastritis in the antral mucosa, with simple G-cell hyperplasia. Tiny sessile polyps with the typical FGPs histological features were seen in the gastric body.
Patient 3—A 58-year-old woman showed at first chronic active H. pylori positive gastritis, with a linear G-cell hyperplasia, and a normal body-fundic mucosa. Thirty months later, the post-eradication endoscopic control evidenced a persistent linear G-cell hyperplasia in an already normal antral mucosa H. pylori negative, with FGPs in the body-fundus.
Patient 4—A 37-year-old woman had at the first endoscopic control normal antral mucosa H. pylori negative, with linear G-cell hyperplasia and associated FGPs.
Patient 5—A 60-year-old woman, with normal antral mucosa H. pylori negative at the first endoscopic control had a linear G-cell hyperplasia, and FGPs.
The prevalence of FGPs in patients with AH (13.1%) was confronted with FGPs’ prevalence in our general endoscopic population (0.7%; 11) by mean of χ2 test with Yates correction. The difference between the two percentages was extremely statistically significant (p<0.0001).
Discussion
We studied morphologically and immunohistochemically the antral biopsies (and body-fundus biopsies in 27 cases) of 38 patients with AH. AH is characterised by a large increase of calcium in the urine, with renal stones and osteoporosis, with normal calcium levels in the blood, due to hypersensitivity of CaSRs located on the antral G-cell membrane. These patients show normal fasting gastrinaemia and meal hypergastrinaemia (Ca2+ and peptones) with median gastrin levels almost doubled compared with normal controls.2 It is now known that gastric CaSR and gastrin-secreting G cells are both activated by Ca2+, amino acids and elevated pH. This association strongly suggests an important role of CaSRs in the meal-stimulated gastrin secretion and regulation.3
The first aim of our histological and immunohistochemical work was to define if patients with AH and meal hypergastrinaemia had morphological antral G-cell alterations. None of the 38 patients had a history of significant dyspepsia or had received antisecretory therapies.
According to literature data,12 and our own experience, normal controls showed 1–2 G cells per gland, with irregular distribution. All our 38 patients presented G-cell hyperplasia, either simple (4–5 cells per gland, uniformly distributed) or linear G-cell hyperplasia (continuous chain-like distribution). In a subset experiment, we scored the mean G cell per gland in our five controls, simple and linear hyperplasia (1.18; 3.48; 7.12, respectively), and we found that the difference between controls and simple hyperplasia was extremely statistically significant (p=0.0003), and the difference between simple and linear hyperplasia was very statistically significant (p=0.0032).
Twenty-six patients initially presented with H. pylori gastritis. As H. pylori infection may induce a G-cell reactive hyperplasia,13 immunohistochemical stainings were performed again after eradication therapy, with a very long mean interval (20.6 months), with identical results in all cases. This very long interval seems to rule out a possible influence of both H. pylori and PPI therapy. None of the patients had shown significant body atrophy, another possible confounding condition for G-cell hyperplasia. Moreover, comparing the percentages of simple and linear hyperplasia between the 12 patients originally H. pylori negative and the 26 patients eradicated, there was not any statistically significant difference. This control between the two groups appears as a further proof of the primitivity of G-cell hyperplasia in patients with AH.
So we could conclude that the observed G-cell hyperplasia was primitive and that it represented the morphological counterpart of meal hypergastrinaemia in AH.
On the other hand, only 2 of 27 patients with a body biopsy had a micronodular endocrine cell hyperplasia. Evidently, in patients with AH, the meal hypergastrinaemia is not high enough to produce marked pictures of endocrine hyperplasia in the body-fundic mucosa, as seen in the Zollinger-Ellison syndrome.14
Unexpectedly, we found in five patients with AH an association with FGPs. FGPs are tiny sessile polyps of the gastric body-fundic mucosa, so far described as sporadic, without other gastrointestinal associations,8 ,10 syndromic forms associated with familial adenomatous polyposis, classic or attenuated,15 ,16 with Zollinger-Ellison syndrome,14 ,17 and recently as part of the gastric adenocarcinoma-associated proximal polyposis of the stomach (GAPPS).6 ,18 In 2 of our 12 patients, with gastric antrum H. pylori negative, the polyps were already present at the first endoscopic examination. In the other three patients, FGPs appeared in the second endoscopic control, after H. pylori eradication. So even in patients with AH, we found an inverse relationship between polyps and H. pylori infection.19 ,20
The prevalence of FGPs associated with patients with AH was more than 10-fold that of sporadic FGPs (13, 1% vs 0, 7% of sporadic FGPs), and this difference was extremely statistically significant. Aprile et al14 demonstrated in a multivariate analysis that in 106 patients with Zollinger-Ellison syndrome there was a statistically significant association between polyp formation and levels of gastrinaemia. Similarly, gastrin may a have a role in the increased prevalence of FGPs in patients with AH.
In a preliminary experiment, we stained with a gastrin antiserum the gastric antrum biopsies of 79 patients with sporadic FGPs that had never been treated with PPI previously; we found that 75.9% of these patients presented a G-cell hyperplasia morphologically similar to patients with AH.5 Furthermore, similar findings were shown by Worthley et al18 in the gastric antrum of patients with GAPPS.6 Apart from this finding, our patients with AH had a negative family history for gastric or colonic cancer, and none of the FGPs showed any dysplastic change.
Another important question to be addressed is to verify if among sporadic FGPs may exist a subset of patients with abnormal calcium excretion, stone formation or abnormal response to calcium or peptone load. At present, we have no data about this interesting question.
In conclusion, we have seen that patients with AH, with sporadic FGPs and with GAPPS share in common an antral G-cell hyperplasia. This fact may represent a promising field of future research.
References
Footnotes
Contributors DP conceived the study design and wrote the draft. BJ gave a substantial contribution in draft preparation. TE and BS contributed substantially to the study design. OB, BA, AI and DM collected cases and also assisted in a critical reading of the manuscript.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.