Article Text

Abstract
Background We aim to compare the real-life direct and indirect costs of switching patients from intravenous to subcutaneous (SC) CT-P13, an infliximab biosimilar, in a tertiary UK Inflammatory Bowel Disease (IBD) centre.
Methods All adult patients with IBD on standard dosing CT-P13 (5 mg/kg 8 weekly) were eligible to switch. Of 169 patients eligible to switch to SC CT-P13, 98 (58%) switched within 3 months and one moved out of area.
Results Total annual intravenous cost for 168 patients was £689 507.04 (direct=£653 671.20, indirect=£35 835.84). After the switch, as-treated analysis demonstrated total annual cost for 168 patients (70 intravenous and 98 SC) was £674 922.83 (direct = £654 563, indirect = £20 359.83) resulting in £891.80 higher cost to healthcare providers. Intention to treat analysis showed a total annual cost of £665 961.01 (direct = £655 200, indirect = £10 761.01) resulting in £1528.80 higher cost to healthcare providers. However, in each scenario, the significant decrease in indirect costs resulted in lower total costs after switching to SC CT-P13.
Conclusions Our real-world analysis demonstrates switching from intravenous to SC CT-P13 is broadly cost neutral to healthcare providers. SC preparations have marginally higher direct costs, switching allows for efficient use of intravenous infusion units and reduces costs to patients.
- INFLAMMATORY BOWEL DISEASE
- INFLIXIMAB
- COST-EFFECTIVENESS
Data availability statement
No data are available. Summary data are available on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Subcutaneous infliximab has similar clinical effectiveness and safety compared with intravenous application.
Subcutaneous infliximab administration can reduce pressure on Inflammatory Bowel Disease (IBD) infusion units.
WHAT THIS STUDY ADDS
Switching patients established on intravenous to subcutaneous infliximab is broadly cost neutral to the British National Health Service.
Indirect costs to patients are lower for those patients switching to subcutaneous infliximab.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
IBD services can implement switches of established patients on intravenous infliximab to subcutaneous infliximab without increasing the overall cost to the National Health Service.
Introduction
The treatment of multiple immune-mediated conditions has been revolutionised by the introduction of the biological medication Infliximab. This medication is a chimeric human-murine monoclonal antibody,1 which has now been licensed for use in many conditions including Inflammatory Bowel Disease (IBD), Rheumatoid Arthritis, Ankylosing Spondylitis and Psoriasis.2 The effectiveness of Infliximab in IBD was first established in Crohns disease (CD)3 and soon after in Ulcerative Colitis (UC).4 Since then, infliximab has transformed the management of IBD and has been shown to reduce hospitalisation and rates of surgery in clinical trials5 with outcomes from population studies now starting to show a trend towards a decreasing rate of IBD-related surgery in the postbiologic era.6
The financial burden of IBD care on health services is significant. In the UK, the average cost of treating patients with UC and CD has been estimated to be around £3000 and £6000 per patient per year, respectively.7 While the therapeutic benefits of biological medications are clear, the originator versions were expensive. We have since seen the development and introduction of biosimilar biologics, which are associated with significant per patient cost savings due to very competitive pricing in the UK.1 Biosimilars are drugs which are comparable to the originator biologics in terms of mechanism of action as well as efficacy and safety.8 CT-P13 is a biosimilar version of infliximab and was initially shown to be efficacious in rheumatological conditions, but its utility has since also been proven in patients with IBD.8–10
The increasing use of intravenous biologic therapy has other implications for healthcare services and patients’ quality of life. Buisson et al demonstrated the significant time burden for patients associated with attending for intravenous infliximab infusions,11 while the cost of running the infusion unit and use of precious nursing time should not be underestimated.12 Additionally, demand on our IBD day case infusion unit has tripled in the last 7 years, leading to long delays in treatment initiation. A subcutaneous (SC) infliximab biosimilar, CT-P13, is now available. SC CT-P13 has been shown to have similar efficacy and safety in the treatment of IBD in both trials and real-world settings.10 13 14 There is a price differential between the intravenous and SC formulations of CT-P13, but the financial impact of switching existing intravenous patients to SC CT-P13 on the health service and wider society is currently unclear. We aim to compare the real-life direct and indirect costs associated with switching patients from intravenous to SC CT-P13 in a tertiary UK IBD centre.
Materials and methods
We recently instigated a switch programme of patients established on intravenous biologics to SC formulations where available.15 All adult patients with IBD undergoing treatment with the Infliximab biosimilar CT-P13 at Leeds Teaching Hospitals Trust, UK were identified from local hospital records. Demographics, disease-specific data and distance between residence and our infusion unit were extracted for each patient from the electronic hospital records. Patients were considered eligible to switch from intravenous to SC CT-P13 if they were on a standard dosing regimen, that is, 5 mg/kg every 8 weeks. Patients were invited to switch via written letter from the lead IBD clinician and subsequent discussion with the IBD nurses at their next CT-P13 infusion. Patients were classified as intravenous or SC based on their decision to switch within 3 months.15
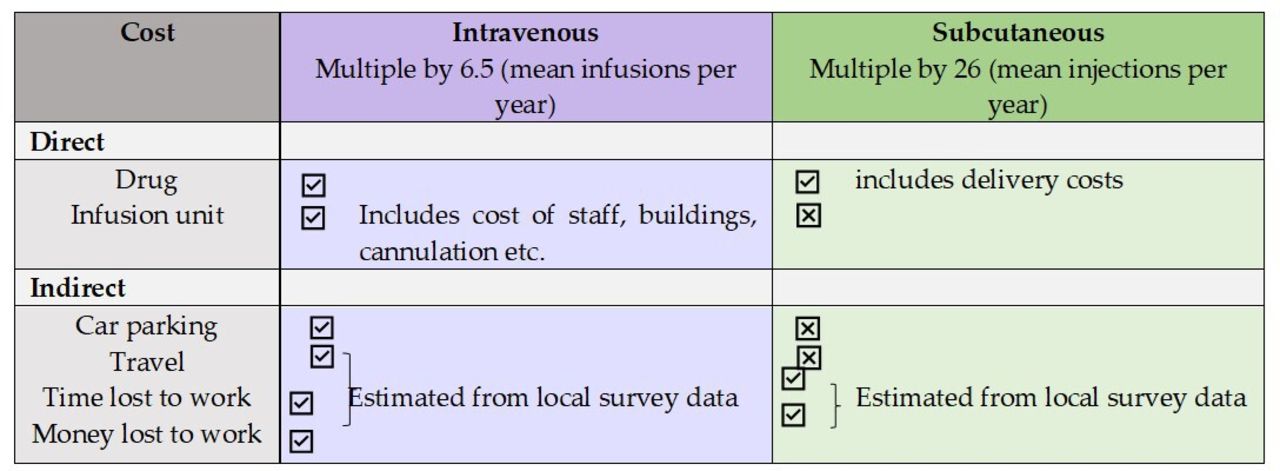
Annual costs were calculated by summating the direct and indirect costs. Figure 1 demonstrates how these costs were calculated. For direct costs, we used average number of infusions (6.5) or injections (26) per year. Medication costs were based on National Health Service (NHS) agreed pricing. The cost of a visit to the infusion unit cost was £325 per patient per visit as per locally agreed costs. There is variation in the costs of day unit infusion visits and we, therefore, performed a sensitivity analysis for a lower price of £249 and a highest price of £389 to allow comparison of costs which may apply to other UK units. For indirect costs, travel data were extrapolated from locally collected survey data from 50 responders.15 The 50 responders provided information on mode of transport, employment status, parking costs and time spent on travel and at the infusion unit. We then extrapolated the 50 responses to the full cohort. Indirect costs were calculated using average UK wage per hour (£13.57),16 advisory fuel rate per mile,17 hospital carparking prices, local return bus ticket prices18 and local taxi prices for the mean journey.19

A table to demonstrate how direct and indirect costs were calculated.
For analysis, we compared costs in intention-to-treat (all patients switched from intravenous to SC) versus as-treated (real-world data, all intravenous preswitch vs actual intravenous and actual SC postswitch). We used a sample of convenience without a formal sample size calculation due to the nature of the study. Continuous data on cost per patient were presented as means. We compared overall costs for the whole cohort and mean cost per patient. All analyses were performed using R V.4.2.1 (2022-06-23).
Results
Of 169 patients were identified as eligible to switch to SC CT-P13. Ninety-eight (58%) switched within 3 months, see table 1 for patient characteristics. One patient was excluded as they had subsequently moved out of area.
Baseline demographics and patient characteristics, stratified by ‘switch’ decision
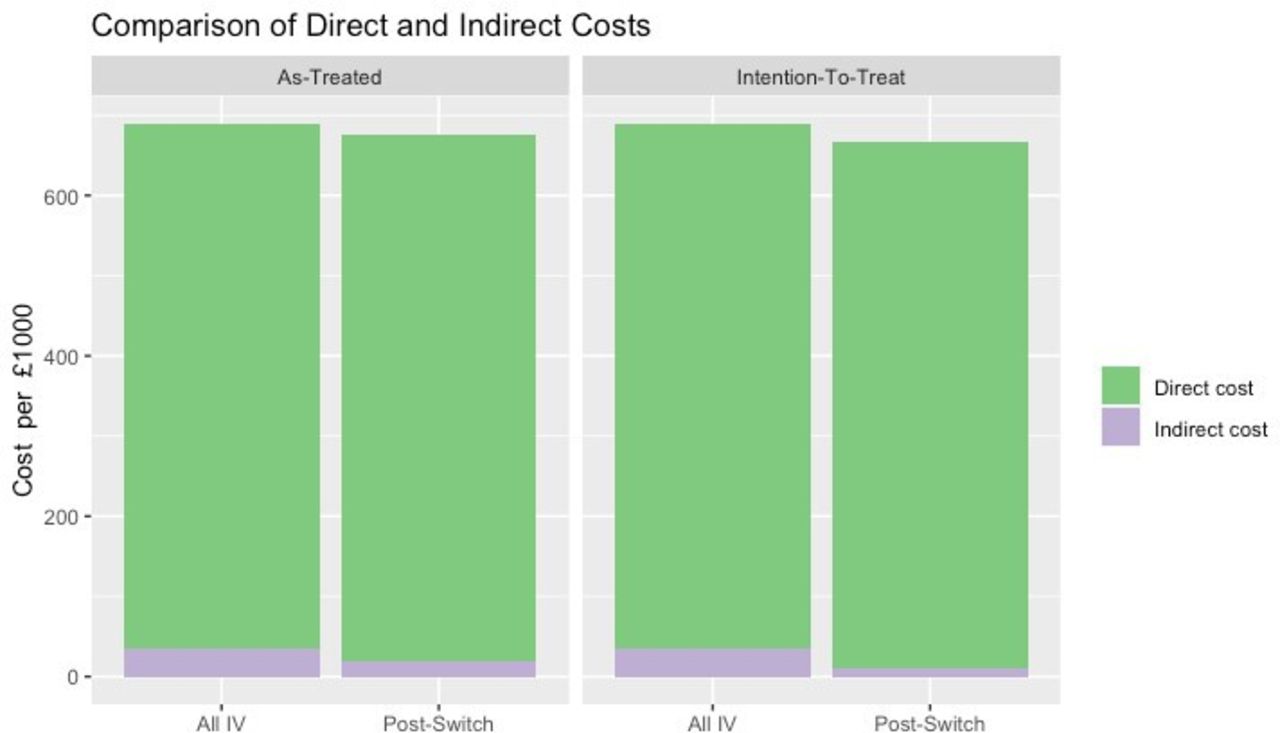
Prior to switching, total annual intravenous cost for 168 patients was calculated as £689 507.04 (direct = £653 671.20, indirect = £35 835.84). In the as-treated analysis after the switch, intravenous cost for 70 patients was £285 490.02 (direct=£272 363, indirect=£13 127.02) and SC cost for 98 patients was £389 432.81 (direct=£382 200, indirect=£7232.81). The total annual cost for 168 patients of £674 922.83 was similar to the preswitch overall costs. In this analysis after a proportion of patients switched to SC, annual direct costs to the health service were marginally higher by £891.80 more per year (figure 2); however, indirect costs or cost to the patient were lower, resulting in a lower overall cost. Per patient overall costs reduced marginally from £4104.21 to £4017.40. Direct per patient costs increased marginally from £3890.90 to £3896.21. Indirect costs per patient decreased from £213.31 to £121.19.
{kind=link}
{kind=link}
A graph to demonstrate the cost comparison between as-treated and intention-to-treat groups.
When analysed on an intention to treat basis overall costs for the whole cohort were lower than preswitch costs £665 961.01 (direct =£655 200, indirect =£10 761.01). However, this is because while direct costs were marginally higher compared with the preswitch period indirect costs were lower. Per patient overall costs reduced marginally from £4104.21 to £3964.05. Direct per patient costs increased marginally from £3890.90 to £3900. Indirect costs per patient decreased from £213.31 to £64.05.
On sensitivity analysis applied to the as-treated analysis with an infusion unit visit cost of £249, overall cohort costs were considerably higher after the switch compared with the preswitch period (£640 342.83 vs £606 515.04 preswitch) due to considerably higher direct costs (£619 983 vs £570 679.20 preswitch). When applying an infusion unit visit cost of £389, overall cohort costs were lower compared with the preswitch period (£704 042.84 vs £759 395.04 preswitch) due to lower direct costs (£683 683 vs £723 559.20 preswitch).
Discussion
The arrival of SC CT-P13 offers more choice to clinicians and patients already established on intravenous infliximab. We have demonstrated that in a real-world cohort setting, the financial impact was broadly similar compared with the preswitch period. A higher price for SC versus intravenous CT-P13 is largely offset by avoidance of infusion unit costs. Indirect costs are considerably lower, which is excellent news for patients who may not wish to spend a considerable amount of time and their own money to attend intravenous infusions.15
We acknowledge that infusion unit costs may vary throughout the UK and have, hence, conducted a sensitivity analysis using the extremes of potentially applied day case fees. When applying the lower and higher extreme end of the fee range, the overall cost impact of a switch swing from a significant extra spend to a significant saving. Services may, therefore, wish to examine the fees charged by the hospital to the NHS primary care budget holders to examine local cost impacts. As our fee lies in the mid of the range, however, we expect that our findings may apply to the wider NHS in the UK.
Decisions to switch existing intravenous patients to SC CT-P13 may be driven by several service factors. These include capacity issues in the infusion unit including shortening time to treatment initiation and applying nurse specialist time to more pressing areas of the IBD service. For patients, a switch to SC CT-P13 offers a significant time and cost saving, which can motivate patients to switch.15
As switching established intravenous patients to SC CT-P13 is safe and effective, the direct and indirect impact on patients should be considered. Indirect impacts include a better IBD service for fellow patients, while direct impact include time and cost savings for the patient offered a switch. We suggest that both impacts are discussed with the patients to allow for an informed decision.
There are a number of limitations to our work. We only had data regarding travel and employment on a percentage of patients collected via a survey. This means we had to extrapolate to calculate these costs to the whole cohort, but we used the actual distance from hospital for each patient in the whole cohort to calculate the costs. Employment costs were estimated using the average national hourly wage, but this may over or underestimate the wages our cohort may receive. Furthermore, it is possible patients travel to the infusion unit from work or another destination and, therefore, our distance measures may not be truly representative. This data were also obtained by retrospective questionnaire and so is susceptible to recall bias. Direct costs are accurate to our setting but may vary in different locations inside the UK or internationally. To overcome this, we also performed a sensitivity analysis, but drug costs in jurisdictions outside the UK may vary considerably. We have examined patients’ motivation to switch in a previous publication15 but did not keep a log of reasons patients gave when not agreeing to a switch to SC infliximab. Collecting reasons for refusal to switch will help plan IBD centres developing their switch programmes. Data on the number of patients requiring support with the SC administration after a switch for a prolonged period would also be helpful for centres considering switches. Future work should address those aspects.
Our real-world analysis demonstrates that a switch from IV to SC CT-P13 is broadly cost neutral to the health service. While the SC option has higher drug costs, a switch to SC allows for more efficient running of intravenous induction therapies by reducing demand on the infusion unit and reduces indirect costs to the patient in terms of travel, parking and potential loss of working hours.
Data availability statement
No data are available. Summary data are available on request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical review and approval were waived for this study as it was performed as a service evaluation and improvement project according to the UK Health Research Authority rules. These types of study are exempt from ethic review and approval. Patient consent was waived it was performed as a service evaluation and improvement project according to the UK Health Research Authority rules. These types of study are exempt from ethic review and approval.
Footnotes
Contributors Conceptualisation—IC, GB, DG, AA and CPS; methodology, CPS; formal analysis—IC, CPS; investigation—all authors; data curation—CPS; writing—original draft preparation—IC, CPS.; writing—review and editing—GB, AA, GC, IC, DG; supervision—CPS. All authors have read and agreed to the published version of the manuscript. CPS is the guarantor of the article.
Funding This study was supported by a grant from Celltrion.
Competing interests IC has received speaker honoraria from Celltrion and research grants from Celltrion. CPS has received unrestricted research grants from Celltrion, Warner Chilcott, Janssen and AbbVie, has provided consultancy to Warner Chilcott, Dr Falk, AbbVie, Takeda, Fresenius Kabi, Galapagos, Ferring, Arena and Janssen, and had speaker arrangements with Warner Chilcott, Dr Falk, AbbVie, MSD, Pfizer, Celltrion and Takeda. All other authors report no conflict of interest.
Provenance and peer review Not commissioned; externally peer reviewed.