Article Text

Abstract
Objective Foreign body ingestion (FBI) occurs infrequently but can be associated with rare risks including perforation. There is limited understanding of the impact of adult FBI in Australia. We aim to evaluate patient characteristics, outcomes and hospital costs of FBI.
Design A retrospective cohort study of patients with FBI was performed at a non-prison referral centre in Melbourne, Australia. International Classification of Disease-10 coding identified patients with gastrointestinal FBI over financial years 2018–2021. Exclusion criteria were food bolus, medication foreign body, object in anus or rectum, or non-ingestion. Criteria for ‘emergent’ classification were oesophagus, size >6 cm, disc batteries, airway compromise, peritonitis, sepsis and/or suspected viscus perforation.
Results Thirty-two admissions attributed to 26 patients were included. The median age was 36 years (IQR: 27–56), 58% were male and 35% had a prior psychiatric or autism spectrum disorder. There were no deaths, perforations or surgery. Gastroscopy was performed in 16 admissions and 1 was scheduled following discharge. Rat-tooth forceps were used in 31% and an overtube was used in 3 cases. The median time from presentation to gastroscopy was 673 minutes (IQR: 380–1013). Management was adherent to European Society of Gastrointestinal Endoscopy guidelines in 81%. After excluding admissions with FBI as a secondary diagnosis, median admission cost was $A1989 (IQR: $A643–$A4976) and total admission costs over the 3 years was $A84 448.
Conclusion FBI in an Australian, non-prison referral centre is infrequent, can often be safely managed expectantly, and has limited impact on healthcare utilisation. Early, outpatient endoscopy could be considered for non-urgent cases, which may reduce costs while maintaining safety.
- endoscopy
- epidemiology
- gastroscopy
Data availability statement
Data are available on reasonable request. The data that support the findings of this study are available from the corresponding author, NN, upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Hospital presentations with foreign body ingestion are increasing in frequency and can accrue significant healthcare costs.
Adverse outcomes such as perforation are rare but are a surgical emergency.
WHAT THIS STUDY ADDS
There were no adverse events or emergent surgeries for foreign body ingestion in an Australian, non-prison referral centre between 2018 and 2021.
Gastroscopy was performed in 50% of presentations and management was as per European Society of Gastrointestinal Endoscopy guidelines in 81%.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Adherence to international endoscopy guidelines on foreign body ingestion may be associated with safe, expectant management and also limited impact on healthcare resource utilisation.
Early, outpatient endoscopy could be considered for non-urgent cases, which may reduce costs while maintaining safety.
Introduction
Foreign body ingestion (FBI) is a potentially harmful and costly hospital presentation, rarely associated with perforation or adverse outcomes and increasing in frequency worldwide.1 Mortality from FBI is exceptionally low with no deaths identified in two case series of 284 patients, though rates of endoscopic intervention remain high.2 3 Incidence is greatest among prison populations due to secondary gain,4 as well as individuals with previous trauma-related personality disorders.5 True incidence at a population level, however, remains unclear due to challenges with identifying cases and recording outcomes in heterogeneous populations, with a spectrum of outcomes ranging from asymptomatic passage to empirical retrieval and emergency laparotomy.1 2
Although there are few epidemiological studies available, patient characteristics of those presenting with FBI are similar in the USA and UK. An audit of hospital admissions data in USA demonstrated a median age in the fourth decade of life, approximately 50% female, and majority with a psychiatric comorbidity.2 A retrospective observation study at a university hospital in the UK described a younger median age of 23 years (SD 8 years), 78% female and 93% with a psychiatric illness.6 It has also been noted that 9% of patients with FBI are admitted from prison,1 2 associated with overlapping issues of psychiatric comorbidities, self-harm and secondary gain. Many of these individuals are psychosocially vulnerable and at risk of adverse outcomes.7
Major international endoscopy societies, including the European Society for Gastrointestinal Endoscopy (ESGE) and the American Society for Gastrointestinal Endoscopy (ASGE), have published standards of practice guidelines for the manageent of FBI,8 9 guided by factors such as object location, size, sharpness, caustic potential and magnetism. Management and adherence to local guidelines were previously well described in case reports10 and case series.11 The more recent retrospective observational study mentioned above also correlates the centre’s management of FBI with ESGE guidelines including median time to extraction and use of protective devices. The study provides reassuring data on safe endoscopic retrieval during hours except in those with oesophageal impaction, which necessitate urgent extraction.6 This approach appears more practical but may deviate from strict guideline-based management. Similarly, a study of 642 adults with FBI correlated ESGE guidelines with type/size of foreign body and time to extraction, finding increased complications in non-emergent endoscopy after 6 hours from presentation. This supports ESGE guidelines that endoscopic retrieval within 6 hours reduces complication rates.12 Alternatively, imaging can be used to exclude FBI with CT demonstrating a negative predictive value of 80% in a retrospective cross-sectional study of adults presenting with FBI.13
There is limited understanding of the economic impact of FBI, particularly within the Australian setting. A single-centre retrospective review of hospital costs associated with intentional FBI in the USA published in 2010, demonstrated a total estimated cost greater than US$2 million over the preceding 8 years.1 Factors that have been associated with intentional FBI in adults include psychiatric disorders, developmental delay, alcohol intoxication and incarceration.8 While these data have previously been reported in observational studies, there is a paucity of local and recent data to guide Australian health services in caring for this vulnerable population with potentially disproportionate healthcare resource utilisation.
Aims
We aim to evaluate the patient characteristics, outcomes and hospital-level healthcare costs of FBI to help inform health service policy and clinical approach to this challenging and multifaceted issue.
Materials and methods
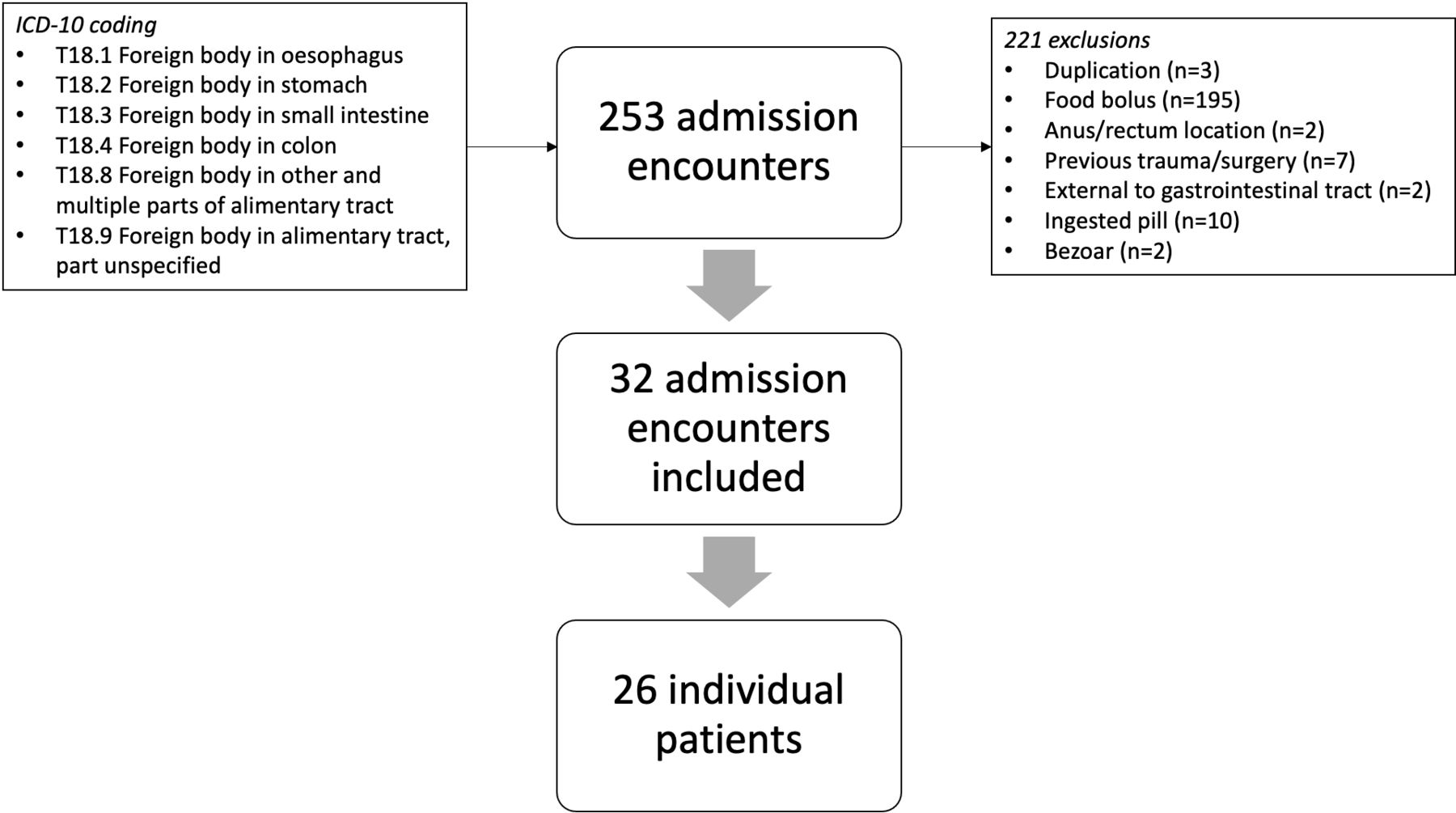
A retrospective cohort study of adult patients presenting with FBI was performed at a tertiary healthcare service in Melbourne, Victoria. The service is not a prison-referral centre nor associated with a long-term psychiatric facility. Cases were identified by searching the hospital admissions database using International Classification of Disease (ICD) version 10 coding for foreign bodies in the oesophagus, stomach, small intestine and colon (figure 1) from 1 July 2018 to 30 June 2021 financial years. We included subjects ≥18 years old who had at least one hospital presentation with FBI, documented through self-reporting or on imaging with a consistent history. Exclusion criteria were foreign body in anus, rectum or genitourinary tract, food bolus, ingestion of an edible substance, pill or non-ingested foreign body. Cases were correlated with clinical data obtained through the electronic medical record, which was deidentified on entry into a secure, electronic database. We collected data on patient baseline characteristics including psychiatric, personality or neurodiverse comorbidities. Cases were categorised using ESGE guidelines or conservative outpatient management, guided by location, size, sharpness, batteries and magnetism (table 1). The following cases were classified as ‘emergent’: oesophageal location and/or obstruction, size >6 cm and/or disc batteries; or critical patient factors including airway compromise, examination features suggestive of peritonism or sepsis, and/or suspected or confirmed oesophageal/gastric/intestinal perforation. Total, direct hospital-related costs by admission episode were obtained from the hospital costings department and reported in Australian dollars.
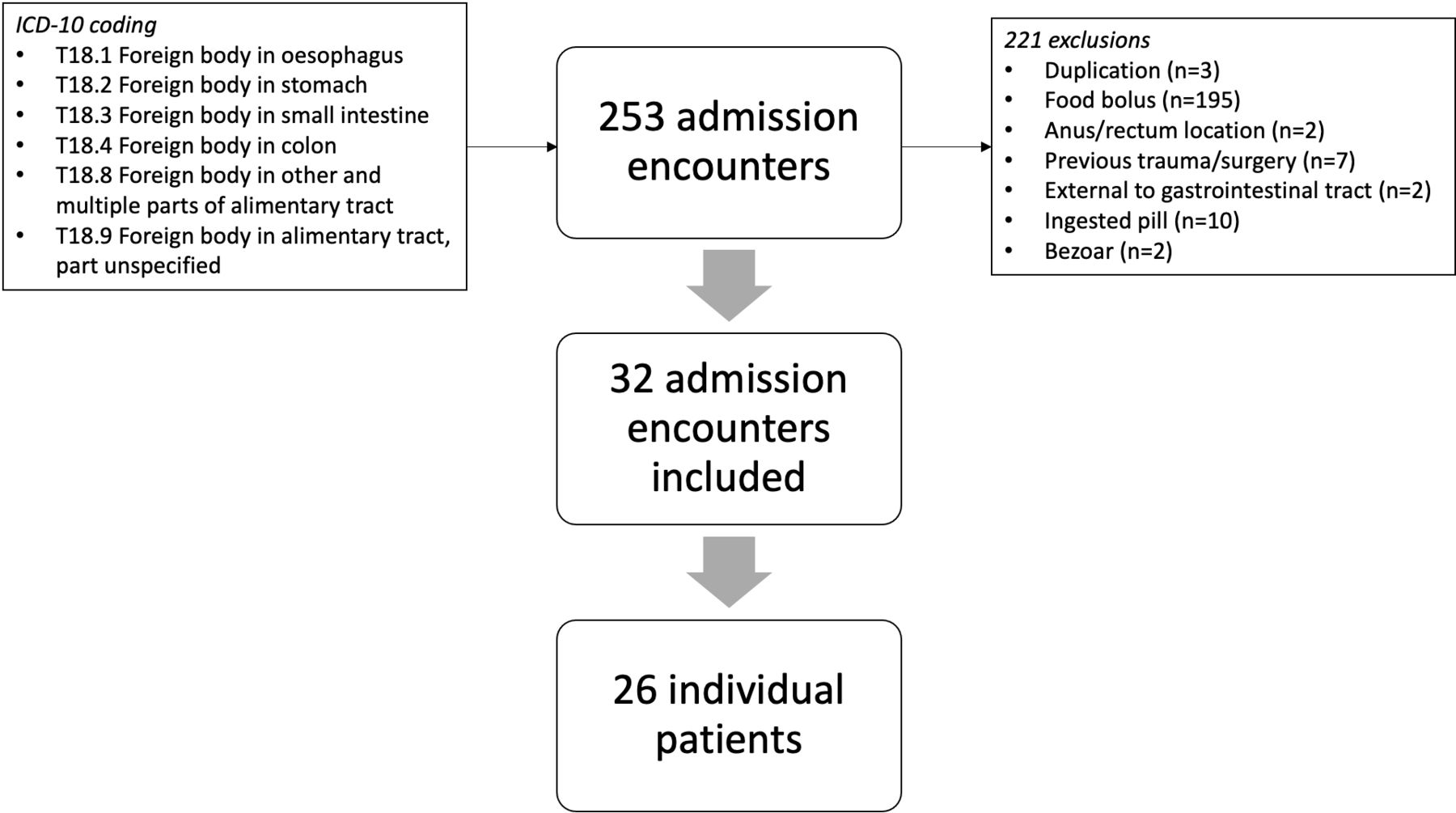
Flow chart of case identification by ICD-10 coding and inclusion/exclusion criteria. ICD-10, International Classification of Disease 10th Revision.
Timing of endoscopic management of FBI according to European Society for Gastrointestinal Endoscopy guidelines
Descriptive data were presented as a median and IQR for non-parametric data, and compared using Mann-Whitney U test. Categorical data were presented as frequency (n) and percentage and compared using a χ2 test. Factors associated with undergoing gastroscopy were compared using logistic regression and presented with an OR, 91% CI and p value. Statistical analysis was performed using Stata/IC V.16.1 (StataCorp) software.
Results
A total of 253 admissions were initially identified from 1 July 2018 to 30 June 2021 using ICD-10 coding with 221 excluded due to duplication (n=3), food bolus (n=195), location in anus/rectum (n=2), foreign body due to previous trauma or surgery (n=7), location external to gastrointestinal tract (n=2), ingested pill (n=10) and bezoar (n=2). Thirty-two admission encounters with FBI were included, attributed to 26 individual patients (figure 1). Intentional ingestion was self-reported in 17 admissions. Seven patients were readmitted with FBI, including four patients with two admissions and a single patient with three admissions. The median age was 36 years (IQR: 27–56) and 15 (58%) were male (table 2).
Patient characteristics
Thirty-five per cent had a prior psychiatric or personality disorder or neurodiversity documented in the medical record including borderline personality disorder (n=6), autism spectrum disorder (n=1), schizophrenia (n=1), and major depressive disorder (n=1) and all 9 of these patients self-reported intentional FBI, which was significant compared with those without a psychiatric diagnosis (p<0.001). Five patients were admitted on an inpatient treatment order or involuntary status, of which one was admitted twice. All patients were admitted from the community except for one who was admitted from a private inpatient psychiatric facility. No patients were incarcerated at the time of admission.
Foreign bodies and endoscopic retrieval
The most common FBI was of dentures (n=5, 16%), followed by blades (n=4, 13%), pins (n=4, 13%), glass (n=3, 9%), bottle caps (n=3, 9%), plastic objects (n=3, 9%), pens (n=2, 6%), nails (n=2, 6%) and one presentation each for battery, toothbrush, fabric hair accessory, coin, ball and aluminium foil (table 3).
Admission data
The most common location of FBI on either imaging or endoscopy was the stomach (n=16, 50%), followed by the oesophagus (n=6, 19%), colon (n=4, 13%) and small intestine (n=3, 9%).
Half of the presentations were managed without intervention, half underwent gastroscopy, and no cases required surgical intervention (table 3). Indications for endoscopic removal were based on ESGE guidelines (summarised in table 1).
Cases were categorised into non-urgent (n=17, 53%), urgent (n=13, 41%) and emergent (n=2, 6%) (figure 2). Of the non-urgent cases, six cases underwent in-patient gastroscopy and all had successful removal of the foreign body.
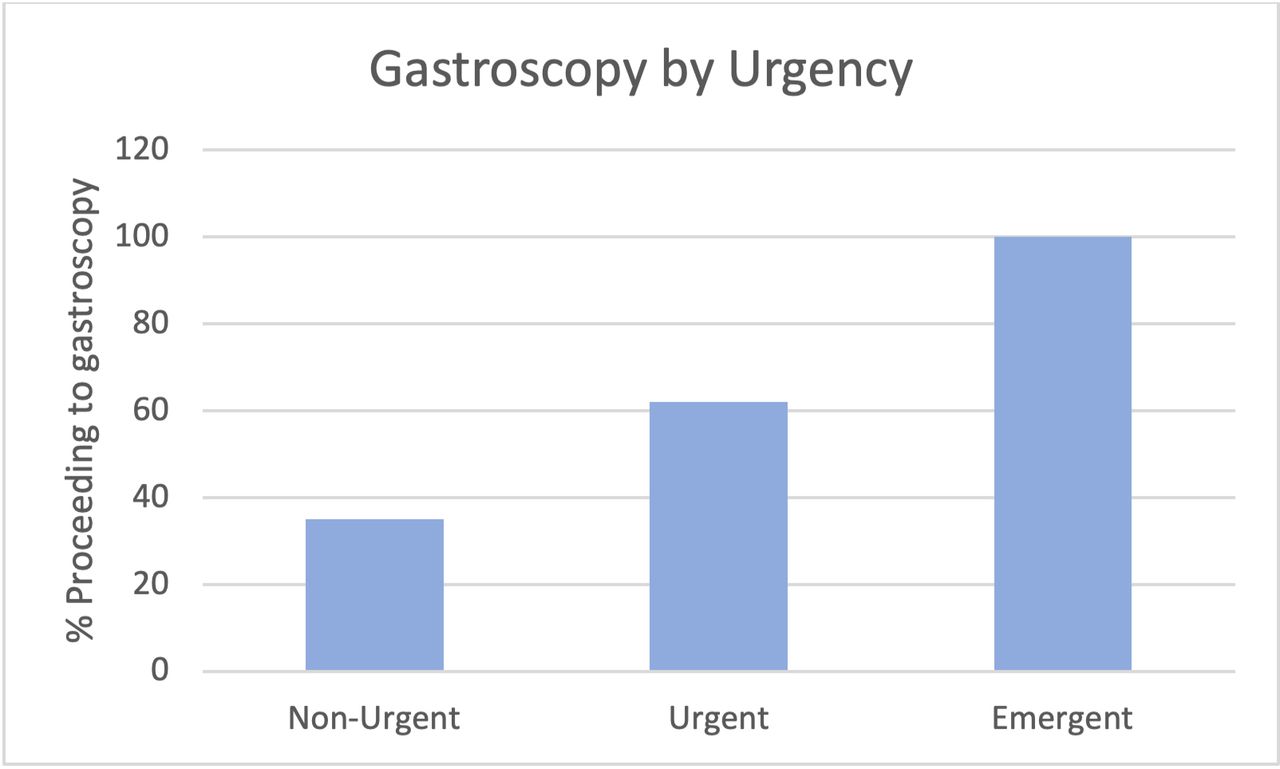
Gastroscopy by category of urgency.
The most frequently used endoscopic accessory for FB extraction was rat-tooth forceps (n=5, 31%). Other devices used were nets (n=4, 25%), snares (n=2, 13%), biopsy forceps (n=2, 13%) and tripod graspers (n=1, 6%). More than one endoscopic tool was used in five cases.
Overtubes were used in 3 (19%) cases for retrieval of a blade (figure 3) and a toothbrush from the stomach using biopsy forceps, and a pen from the oesophagus using rat-tooth forceps. A net was used in an unsuccessful retrieval of 24 small magnets and 48 screws, requiring 30–40 passes of the net.
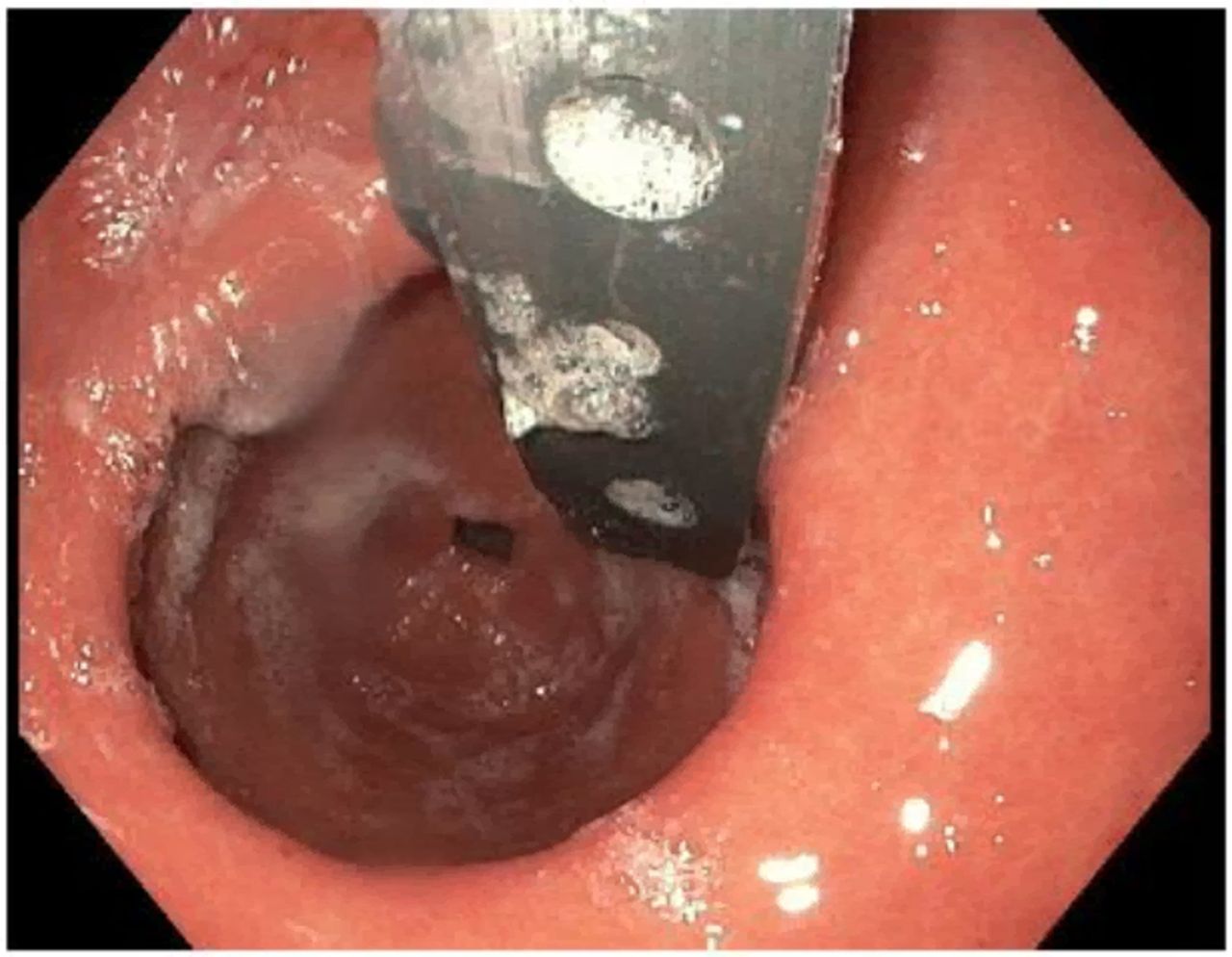
Endoscopic image of blade in stomach.
Of the total 16 gastroscopies, the median time from presentation to procedure was 673 min (IQR: 380–1013). Seven were performed after hours, between 17:00 and 08:00 hours, during which time staff levels are reduced and there are no elective endoscopy lists.
Outcomes
There were no deaths, perforations, endoscopic complications or surgical interventions performed. Management in 26 cases (81%) was adherent to ESGE guidelines. Two cases met criteria for emergent retrieval due to being both sharp and located in the oesophagus. One case was a pen, retrieved endoscopically at 175 min. A second case was a pin, retrieved at 630 min from presentation, with delays to gastroscopy due to theatre availability. Five other cases involving sharp objects (pins n=2, nail n=1, blade=1, plastic shard n=1) located in the stomach, for which retrieval within 24 hours would be indicated, were managed expectantly with no emergent or elective gastroscopy performed. A single case was discharged after presenting with self-reported ingestion of a small shard of plastic. This was not seen on imaging and the patient was scheduled for elective gastroscopy at 24 days from initial presentation at which time the foreign body could not be located.
Admissions and costs
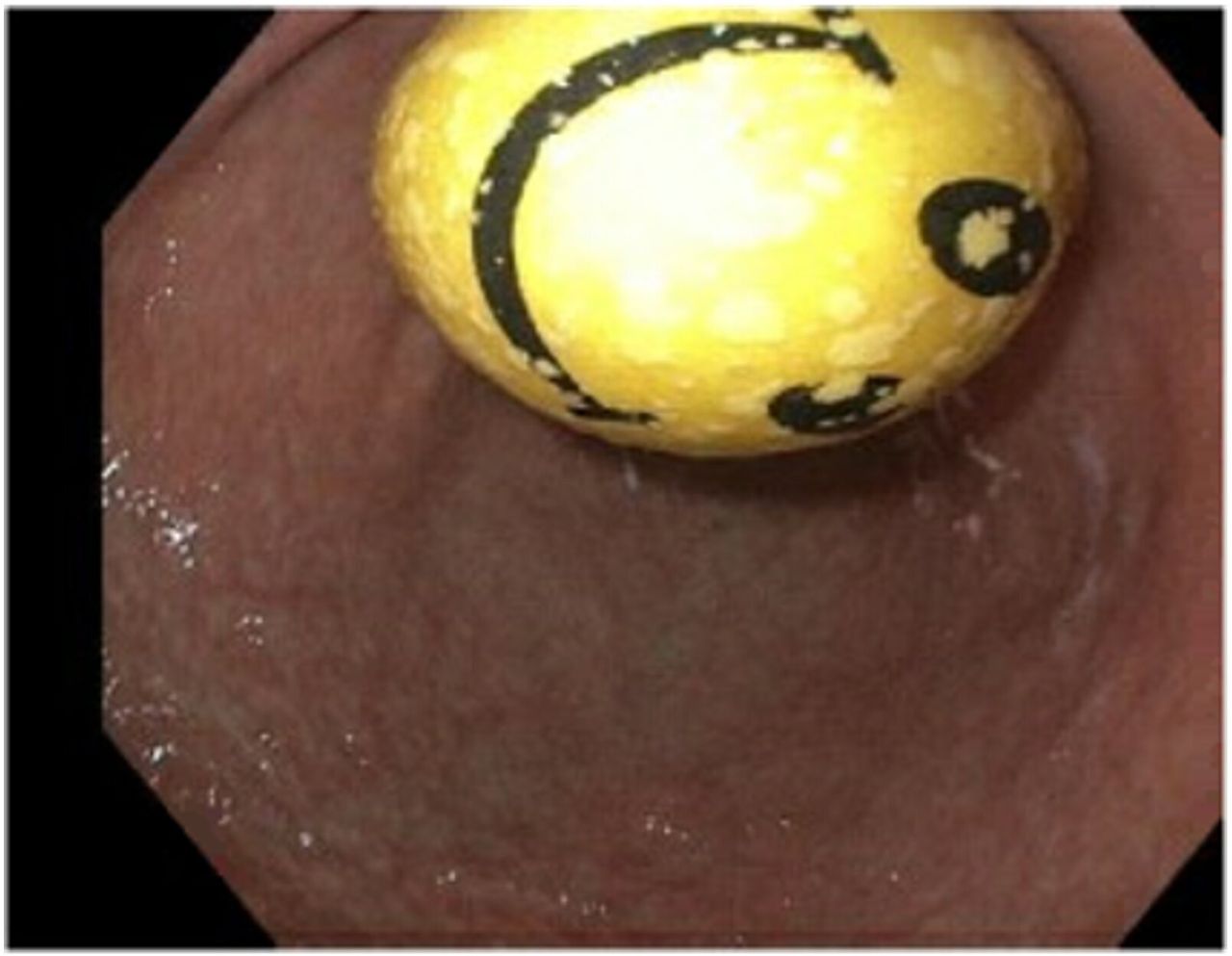
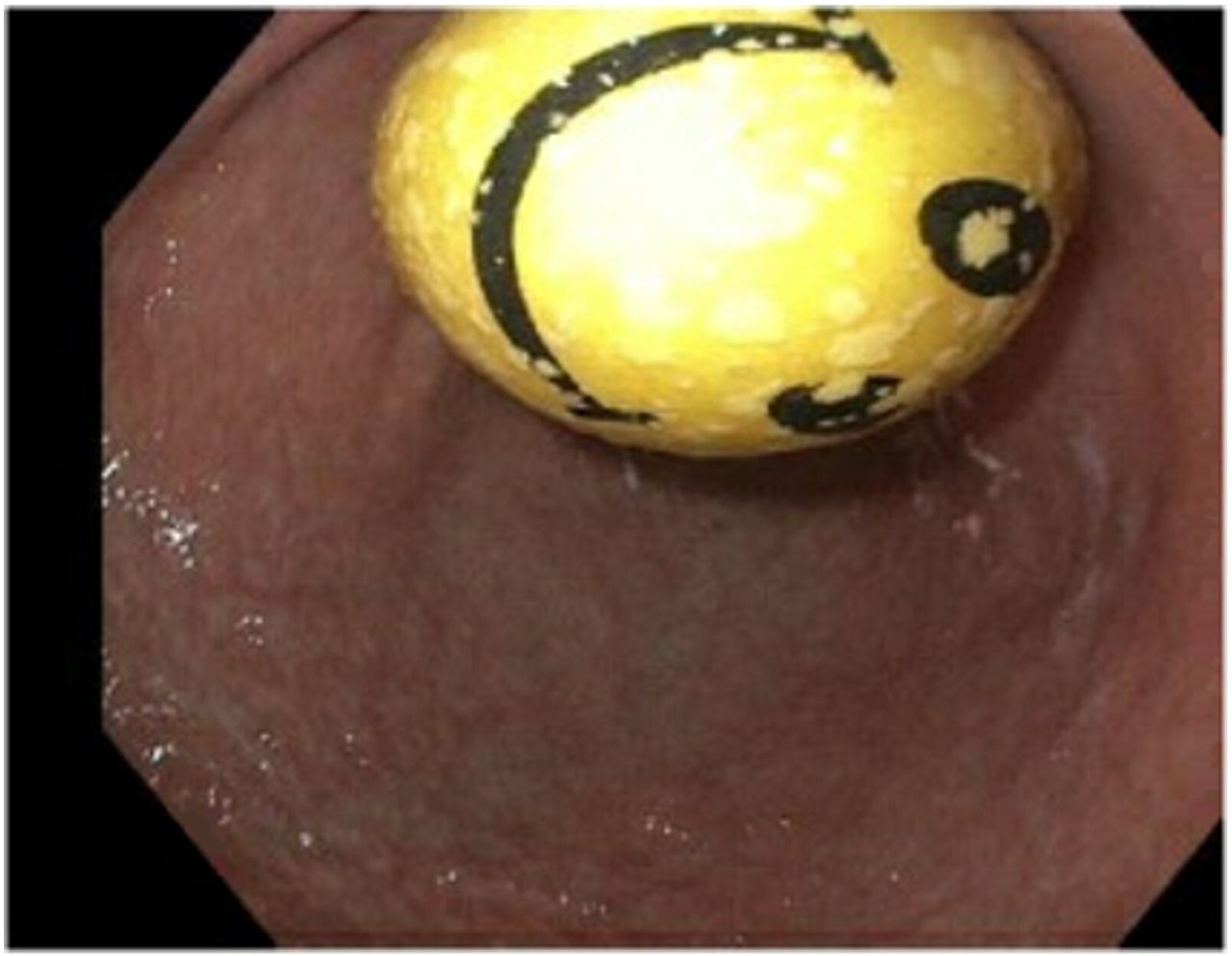
FBI was the primary diagnosis in 27 of the 32 admissions. Of the other five admissions, two were incidental FBI found imaging which were both successfully retrieved endoscopically using a net. One of these was a coin located in the oesophagus during an admission for an unwitnessed fall, and another was a shard of plastic in the stomach during an admission for complications related to HIV. One-third incidental FBI was a rubber ball in the stomach (figure 4) identified during routine gastroscopy for Barrett’s oesophagus surveillance, which was removed with a net. Two patients were admitted under acute psychiatry, one for an acute psychotic disorder with endoscopic retrieval of an ingested fabric hair accessory during their 46-day admission. The other patient was admitted following an uncomplicated, intentional polypharmacy overdose, with an ingested bottlecap identified in the stomach on imaging, managed expectantly.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidental rubber ball found in stomach on elective gastroscopy.
The median length of stay (LOS) was 1 day (IQR: 1–1) and median total admission cost was $A2551 (IQR: $A950–$A5664). However, this included three prolonged admissions with FBI as a secondary diagnosis for: acute psychotic disorder (LOS: 46 days, total admission cost: $A52 056), HIV complications (LOS: 15 days, total admission cost: $A21 060) and unwitnessed fall (LOS: 15 days, total admission cost $A24 699). Costs were recalculated after excluding these admissions as well as two others where FBI was a secondary issue (polypharmacy overdose, elective gastroscopy for Barrett’s oesophagus surveillance). The median LOS remained 1 day (IQR: 1–1), and median total admission cost was $A1989 (IQR: $A643–$A4976). The sum total admission cost over the three financial year period was $A84 448.
Discussion
This study suggests that at our tertiary metropolitan hospital, FBI: occurs relatively infrequently at less than 10 cases per year, is managed well with 81% adherence to guideline-based care and absence of complications or surgical intervention, and has low impact on healthcare resources with a 1-day median length of stay and median admission cost less than $A2000. While our patient demographics are similar to overseas data regarding age and sex, only 35% of our cohort had a diagnosed psychiatric, personality, or neurodiverse condition, compared with 79%–85% in prison referral centres.1 2
Although the majority of FB pass spontaneously, theoretical complications can include perforation, peritonitis, mediastinitis, bowel obstruction and death.1 The initial management must, therefore, include a detailed history and examination to ensure both early identification of complication and risk assessment for potential complications. Sharp, oesophageal foreign bodies, such as the two emergent cases we describe, have the greatest risk of injury, which can include obstruction, perforation, tracheo-oesophageal fistula, aorto-oesophageal fistula and abscess formation.14 Examination findings may guide suspicion for complications such as oesophageal perforation with neck swelling or crepitus; or airway obstruction with stridor. One should only proceed to gastroscopy in the absence of airway compromise.15 Features that indicate identification of FB during emergent endoscopy may include immediate onset symptoms following ingestion, dysphagia and absence of pharyngeal localisation.16 There are limited minimally invasive alternative treatments to endoscopy however bougienage with an oesophageal dilator has been trialled for impacted oesophageal coins in children.17
Despite the low volume of cases observed at our centre, we are reassured by the 81% adherence to guidelines and uncomplicated management. Of the six cases that were non-adherent to guidelines, two could not identify the foreign body on imaging and were thought to have passed. Reduced access to emergency theatre caused delay to endoscopy in two cases and resulted instead in a monitoring plan with serial abdominal X-rays. Although no complications were identified in these six cases, it is likely that more could be done to advocate for guideline-based care for these patients. Four cases involved patients with psychiatric diagnosis, and a ‘code grey’ for physical aggression was called for two cases. This retrospective study cannot identify associations between these features and non-adherence to guidelines, however, does highlight the vulnerability of this cohort. There is variability of recommendations among international societies, particularly when comparing ESGE to ASGE guidelines. For example, management of oesophageal foreign bodies is recommended within 2–6 hours by ESGE and within 24 hours by ASGE.8 Additionally, endoscopic retrieval within 24–72 hours is recommended by ESGE for gastric or proximal small bowel foreign bodies, however, ASGE suggest conservative outpatient management for asymptomatic gastric foreign bodies. The reasons for differing recommendations may be associated with citation of more recent literature in the 2016 ESGE guidelines, compared with the 2011 ASGE guidelines; or local variations in clinical presentations or populations.
Our centre differs from recently published international data with regards to lower case volume, lower frequency of psychiatric comorbidity and absence of female predominance. Reasons for these differences may include that the centre is not associated with a prison. It is unclear the impact of the COVID-19 pandemic on both ours and international cohorts of patients reporting FBI, however, the isolation, rise in mental health issues18 and substance use disorders19 may also contribute, particularly in Melbourne, Victoria where the lockdown strategy was particularly prolonged.20
Only one admission was discharged after the acute presentation with a scheduled elective gastroscopy for retrieval of intragastric shard of glass. By the time of the elective procedure at day 24 from presentation, the foreign body was unable to be located. The cost of the initial emergency presentation was $A1989.09 for the overnight stay, and the cost of the elective gastroscopy as a day procedure was $A918.13. This compares favourably with the median admission cost of $A4917.18 (IQR: $A2752.76–$A5881.71) for patients undergoing in-patient gastroscopy.
Limitations of this study include the small sample size attributable to confinement to a single centre, and absence of prison referrals which limits volume. Due to the retrospective nature, time to endoscopy was measured from time of hospital presentation rather than time of ingestion, and intentional FBI could not be accurately assessed. Only local hospital admissions data and costs were accessible, and therefore, presentations or procedures at other health services were not accounted for.
Conclusions
FBI in a metropolitan, non-prison referral centre is infrequent, safely managed and has limited impact on healthcare utilisation. The majority of cases can be managed expectantly, however, evidence-based guidelines should be applied to ensure that high-risk cases are managed appropriately. Early, outpatient endoscopy could be considered for non-urgent cases to reduce both hospital-related costs and length of stay, while also maintaining quality and safe care.
Data availability statement
Data are available on reasonable request. The data that support the findings of this study are available from the corresponding author, NN, upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was granted by Alfred Health Human Research and Ethics Committee
References
Footnotes
Contributors NLYN and KT were involved in the conception and design of the article, NLYN and JK undertook data collection. NLYN undertook data analysis, all authors were contributed to writing, editing and revising the manuscript. KT is the principal investigator and guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.