Article Text

Abstract
Aim The aim of this systematic review is to evaluate the efficacy and safety of rifaximin in the prophylaxis of spontaneous bacterial peritonitis (SBP) as compared with norfloxacin.
Methods We searched MEDLINE, CINAHL, Google Scholar and Cochrane databases from inception to January 2017. Reference lists of articles as well as conference proceedings were manually screened. We included studies that recruited patients with cirrhosis and ascites who met the criteria for primary or secondary SBP prophylaxis as defined by the European Association for the Study of the Liver and American Association for the Study of Liver Diseases. Two independent investigators reviewed the studies for eligibility, extracted the data and assessed study quality using the Cochrane risk of bias tool. The primary outcome was occurrence of SBP. Secondary outcomes included mortality and adverse events with therapy.
Results Of the 435 studies identified, a total of five were included for full-text review. Four studies were eligible for the systematic review, three of which were randomised controlled trials and one was a prospective observational study. The population examined in majority of studies was primarily hepatitis C cirrhosis. The results of individual studies indicated either superior efficacy of rifaximin or no statistical difference between rifaximin and norfloxacin for SBP prophylaxis.
Conclusions Moderate-quality evidence shows that long-term use of rifaximin appears to be a reasonable alternative to norfloxacin for SBP prevention in hepatitis C cirrhosis.
- CIRRHOSIS
- ASCITES
- PERITONITIS
- ANTIBIOTIC THERAPY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Liver cirrhosis, a major global health burden, accounts for ∼1 million deaths every year.1 Spontaneous bacterial peritonitis (SBP) is one of the most serious and life-threatening complications of cirrhosis, now carrying an in-hospital mortality of 16–23% in the USA.2 The proposed mechanism for development of SBP is translocation of intestinal bacteria into mesenteric lymph nodes and the ascitic fluid.3 ,4 On surviving an incident episode of SBP, the recurrence rate is ∼70% at 1 year.5 High recurrences coupled with substantial mortality warrant long-term antibiotic prophylaxis to prevent SBP.6 Various oral antibiotics have been studied to reduce the risk of occurrence and recurrence of SBP by achieving ‘selective intestinal decontamination’.6 The American Association for the Study of Liver Diseases (AASLD) and European Association for the Study of the Liver (EASL) recommend norfloxacin, a systemic antibiotic, as the first-line therapy for this purpose.7 ,8
Rifaximin is a broad-spectrum ansamicin antibiotic that is poorly absorbed in the gastrointestinal tract and thereby reaches high levels in the gut lumen.9 Its role as an initial and add-on therapy for hepatic encephalopathy has been well established.10 Moreover, it has recently been evaluated as a prophylactic antibiotic to reduce the risk of recurrence of SBP. We conducted a systematic review to compare rifaximin to the standard of care (norfloxacin) for primary or secondary prevention of SBP.
Methods
Standard Cochrane guidelines and PRISMA statement for systematic review were followed during the review process11 ,12 (figure 1).
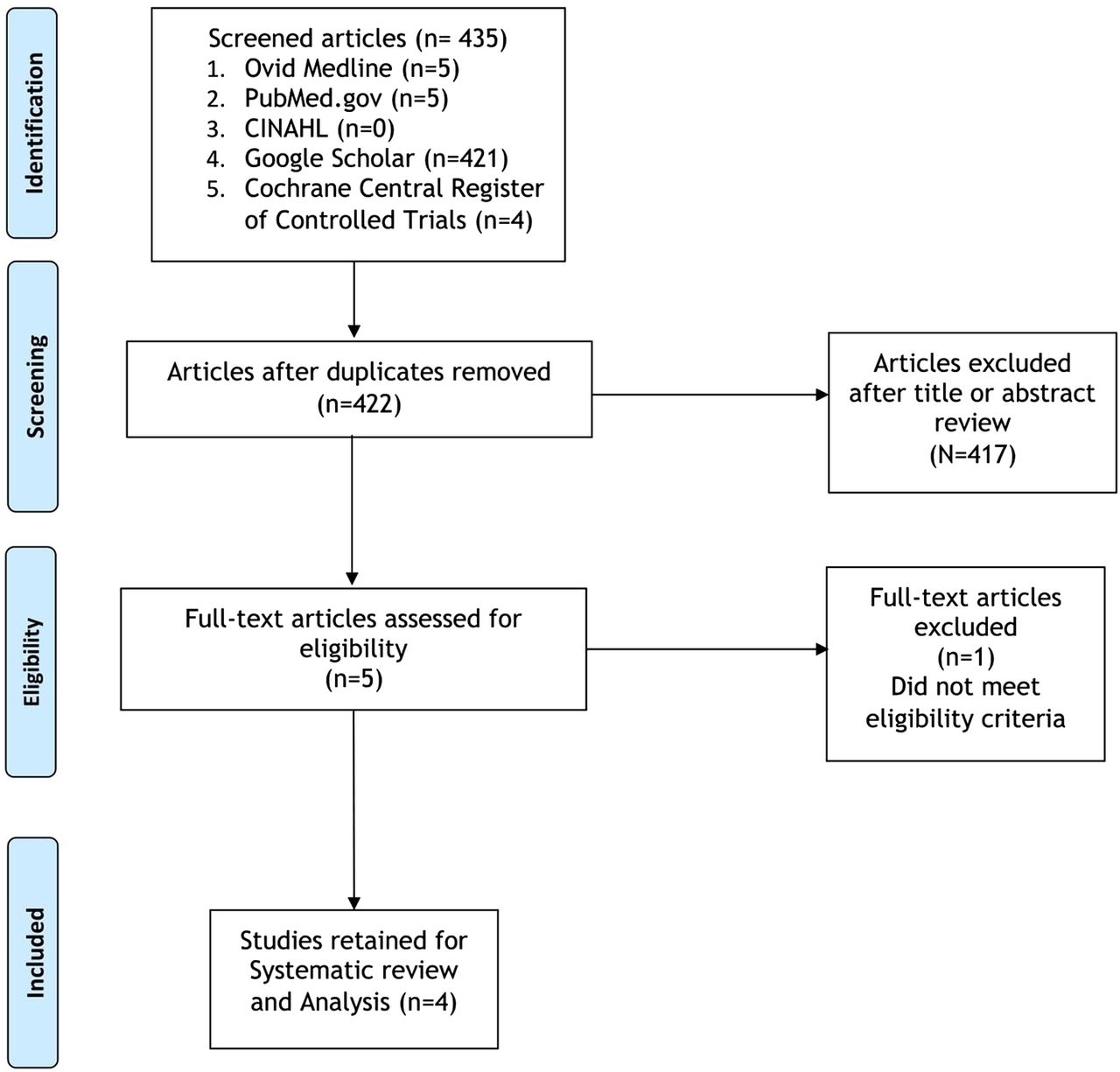
PRISMA flow diagram.
Criteria for considering studies for this review
Types of interventions
We included trials that studied long-term (>3 months) administration of rifaximin at any dose compared with norfloxacin for the purpose of primary or secondary prevention of SBP.
Types of participants
Studies that recruited patients with cirrhosis (irrespective of aetiology) and ascites were included in our analysis.
The indications for long term SBP prophylaxis included either primary (high risk patients with baseline ascitic fluid total protein <1.5 g/dL along with impaired renal function [serum creatinine ≥1.2 mg/dL, BUN ≥25 mg/dL or serum Na ≤130 mEq/L] or patients with liver failure [Child-Pugh score ≥9 and serum bilirubin ≥3 mg/dL]) or secondary prophylaxis (previous episode of SBP).7
Patients with active or recent gastrointestinal bleed, known liver malignancy or hypersensitivity to the planned drugs were excluded.
Types of outcome measures
The primary outcome measure across all studies was the occurrence of SBP. We used the AASLD definition of SBP, that is, the diagnosis is made in the presence of an elevated ascitic fluid absolute polymorphonuclear leucocyte (PMNL) count ≥250 cells/mm3 without an evident intra-abdominal, surgically treatable source of infection.7 The secondary outcome measure was all-cause mortality, defined as death due to any cause during the study period.
Study search and selection
We performed both computerised and manual searching of articles from digital dissertation databases, including Google Scholar, CINAHL, MEDLINE and Cochrane CENTRAL Register for Controlled Trials from 1950 until January 2017. We limited our search to studies involving humans only and articles published in the English language using keywords and/or medical subject headings (MeSH) for ‘rifaximin’ and ‘norfloxacin’ and ‘spontaneous bacterial peritonitis’.
Reference lists of returned search articles were manually screened. Two authors independently reviewed all articles for inclusion. First, all titles and abstracts were assessed and irrelevant articles were rejected. Second, full-text articles were assessed and studies were selected based on meeting the inclusion criteria. After identifying relevant titles, all abstracts were read and eligible articles were selected.
Data extraction
Two authors independently extracted the following data from the included studies using a standardised data form: author(s), year of publication, journal of publication, type of study, sample size, inclusion/exclusion criteria, dose/duration/frequency of rifaximin and norfloxacin administration, cointerventions (if any), outcome measure(s), follow-up period and whether or not data were presented as an intention-to-treat analysis.
Results
Four studies were eligible for our systematic review (table 1). Three were randomised trials and one was a prospective longitudinal study. All studies were published in English language. Three studies were conducted in Egypt and one was a multicentre study involving centres in Egypt and Saudi Arabia. Baseline characteristics of the patients in individual studies were also examined (table 2).
Studies assessing efficacy of rifaximin versus norfloxacin for SBP prophylaxis
Baseline characteristics
Assessment of risk of bias
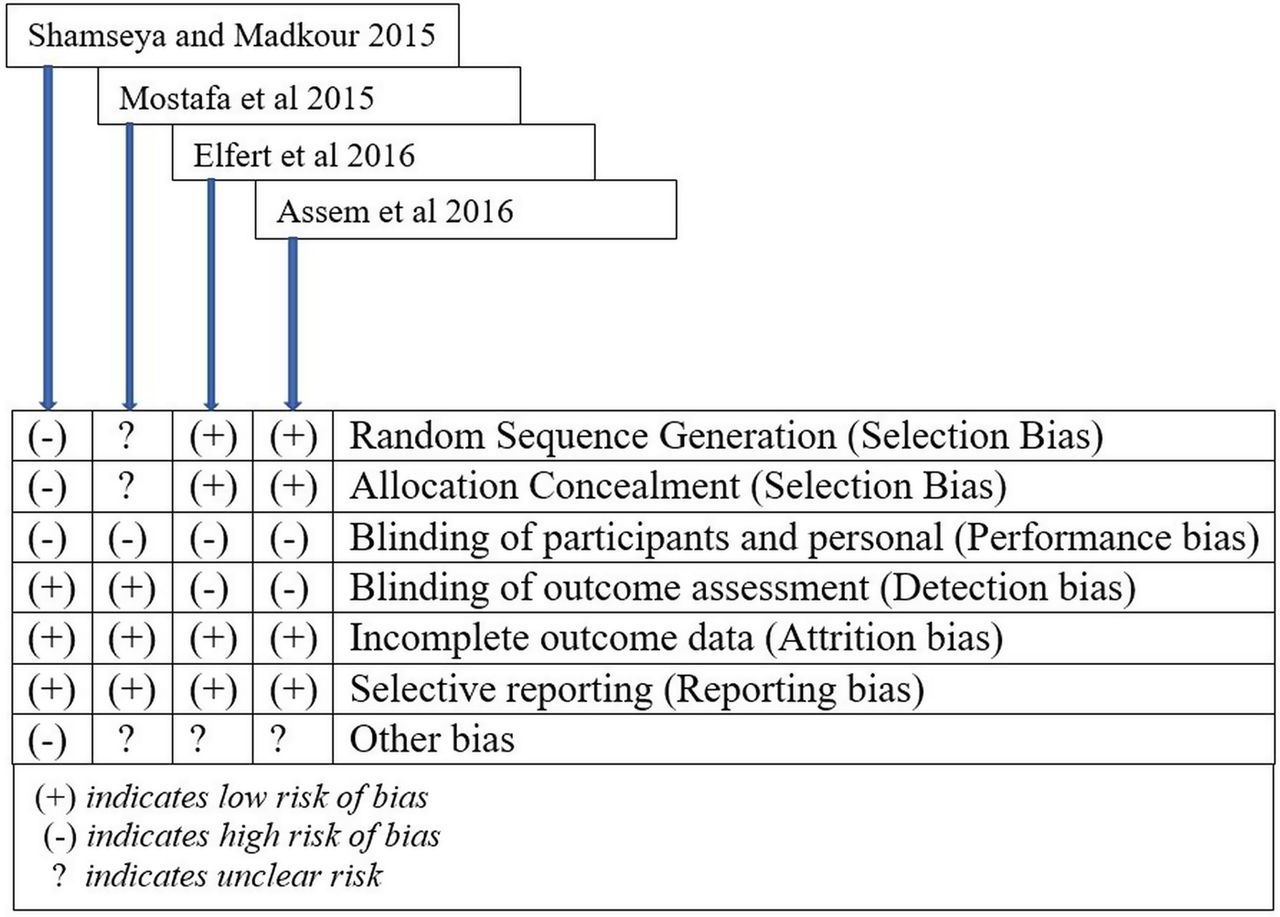
We independently assessed the risk of bias of all trials, without blinding the trial names, using the Cochrane risk of bias tool (figure 2).13 Risk assessment was carried out using four components: randomisation, blinding, attrition and intention-to-treat analysis.
Question 1: Efficacy of rifaximin versus norfloxacin for prevention of occurrence/recurrence of SBP (tables 3 and 4)

{kind=link}
{kind=link}
Cochrane risk of bias tool.
Interventions and follow-up
Comparison of rifaximin and norfloxacin for spontaneous bacterial peritonitis event rate
In 2015, Mostafa et al14 conducted a single-centre randomised trial and enrolled 70 patients at the National Liver Institute in Egypt who were previously diagnosed with SBP—the definition of which was any prior ascitic fluid with >250 PMNL, with or without positive culture, and an absence of other source of intraabdominal infection. The aetiology of cirrhosis in all patients was hepatitis C. Patients were excluded if they had hepatocellular carcinoma or active/recent gastrointestinal bleeding. Forty patients were assigned to the rifaximin group, receiving 800 mg per day, and 30 patients to the norfloxacin group, receiving 400 mg per day. Therapy was given for 6 months. Three months after initiation of therapy, there were five patients in the norfloxacin group (16.67%) who developed SBP compared with none in the rifaximin group. The study was designed specifically to measure outcomes of blood levels of liver function tests, cytokines and other markers of inflammation with time, thus no p value for the outcome of recurrent SBP was stated.
Another trial in 2015 was conducted in Egypt by Shamseya and Madkour.15 They enrolled 86 patients in a prospective observational study. All patients had cirrhosis as a result of hepatitis C. They excluded patients with other aetiologies for cirrhosis, hepatocellular carcinoma and hypersensitivity to the study drugs. More than 70% of patients received the medications for primary prophylaxis of SBP, while the rest received them for secondary prophylaxis. A prior episode of SBP was defined as ascitic fluid with >250 PMNL. The groups were equally divided into the norfloxacin group, receiving 400 mg per day, and rifaximin group, receiving 1200 mg per day in three divided doses. They were matched for age, sex and Child-Pugh class. Renal function and ascitic fluid albumin concentrations were also similar across both groups. At the end of 1 year of follow-up, six patients developed SBP in the norfloxacin group (14%) compared with two patients in the rifaximin group (4.7%), with a p value of 0.265.
Assem et al16 conducted a multicentre randomised controlled trial to compare rifaximin, norfloxacin and combined therapy for primary prevention of SBP at five centres across Saudi Arabia and Egypt. All aetiologies for cirrhosis were included. Patients were enrolled so long as no prior history of SBP existed—defined as ascitic fluid >250 PMNL. Patients with recent gastrointestinal bleeding or hepatocellular carcinoma were excluded. Patient were divided into three groups—norfloxacin 400 mg per day, rifaximin 1100 mg per day in two divided doses and alternating norfloxacin/rifaximin receiving 1100 mg per day rifaximin for 1 month alternating with 400 mg per day norfloxacin. The patients were followed up for a duration of 6 months. Thirty-four patients in the norfloxacin group (34/78=43.6%) developed SBP as compared with 26 patients in the rifaximin group (26/82=31.7%) with a p value of 0.121. These results were based on intention-to-treat principle, though data for per-protocol analysis were also presented. Of interest, in the comparison of all three groups, the highest rate of success in both intention-to-treat and per-protocol analysis was in the combined group which used alternating norfloxacin and rifaximin regimen.
Another trial was conducted by Elfert et al,17 who enrolled a total of 262 patients with cirrhosis and one prior episode of SBP—again defined as ascitic fluid with >250 PMNL. Follow-up period was 6 months, with patients enrolled to receive either norfloxacin 400 mg per day or rifaximin 1200 mg per day in three divided doses. The recurrence rate of SBP was 3.9% in the rifaximin group compared with 14.1% in the norfloxacin group, with a p value of 0.04 when analysing the reported per-protocol results.
Question 2: Mortality benefit with rifaximin as compared with norfloxacin
Elfert et al observed a distinct mortality benefit with rifaximin (13.8% vs 24.4%), which was statistically significant when compared with norfloxacin with a p value of 0.044. Both trials from Shamseya and Madkour and Assem et al demonstrated a numerical difference in mortality rates between rifaximin and norfloxacin groups, though they were not statistically significant. Shamseya and Madkour showed a reduction in mortality rate from 9.3% in the norfloxacin compared with 7% with rifaximin group. Assem et al similarly showed a reduction in mortality rate with the rifaximin group (2.4%) versus the norfloxacin group (7.6%). There were no deaths during the 6 month follow-up in the Mostafa et al study groups. The leading causes of mortality across all studies were hepatorenal syndrome, sepsis, variceal bleeding and hepatic encephalopathy.
Question 3: Safety profile of rifaximin as compared with norfloxacin
No serious adverse events were reported in any of the trials with either of the drugs. Minor adverse events such nausea, abdominal pain, flatulence and headache were reported, with similar incidences in the trials conducted by Shamseya and Madkour and Assem et al. The Elfert et al trial, however, reported a statistically significant lower overall incidence of these adverse events in the rifaximin group as compared with norfloxacin (p=0.033). Though the adverse symptom event rates were different, they did not appear to be limiting enough to suspend consumption of the drug or alter the outcomes of SBP or death.
Discussion
The purpose of this systematic review is to compare the efficacy of rifaximin with the standard of care (norfloxacin) in the prevention of SBP. Our review is based on summarising evidence from three randomised controlled trials and 1 prospective observational study.14–17 In brief, the trial by Elfert et al was remarkable for significantly superior efficacy of rifaximin, while Shamseya and Madkour and Assem et al showed statistically insignificant difference between rifaximin and norfloxacin.15–17 Another trial by Mostafa et al showed a numerical difference in event rate favouring rifaximin for SBP prevention.14 It appears that rifaximin may have a role in prophylaxis of SBP in patients with cirrhosis. It may also be associated with a greater reduction in the risk of death in these patients, compared with norfloxacin. The clinical relevance of this review stems from the high mortality associated with SBP in patients with decompensated cirrhosis.
Hanouneh et al18 first studied rifaximin for prevention of SBP. They compared it with placebo in a group of 404 patients with cirrhotic ascites and found a 72% reduction in the occurrence rate of SBP for rifaximin as compared with placebo. Another study by Vlachogiannakos et al19 demonstrated significantly lower risks of variceal bleeds, SBP, hepatic encephalopathy and hepatorenal syndrome in the rifaximin group compared with matched controls. Lutz et al20 conducted a study evaluating the use of antimicrobial prophylaxis with rifaximin versus ciprofloxacin for SBP prevention in 152 patients with cirrhotic ascites. They found the SBP prevention rate to be higher in the ciprofloxacin group, than both rifaximin and placebo groups. However, the follow-up duration was extremely short (4 weeks) and the patient population was small (17 patients in ciprofloxacin group). We limited our review to studies evaluating long-term SBP prophylaxis and excluded studies with follow-up periods <3 months.
The results might partly be explained by the recent advances in understanding of the pathogenic microbiota responsible for SBP. Selective intestinal decontamination, using norfloxacin, may have led to the emergence of antibiotic-resistant microorganisms in the gut flora.21 This might also be responsible for the recent increase in cases of SBP caused by gram-positive organisms.21 ,22 Elfert et al and Mostafa et al demonstrated a majority of the cases of SBP in the norfloxacin group were due to gram-positive cocci, of which most were resistant to norfloxacin. It was hypothesised that broader spectrum coverage of rifaximin including gram-positive organisms is responsible for efficacy demonstrated in those clinical trials. There is growing evidence that there are other factors at play and that the actual mechanism(s) may be unclear. Bajaj et al23 evaluated the relative changes in stool microbiome in cirrhotics with infections including SBP versus uninfected cirrhotics. The authors found a relative increase in pathogenic (both gram-positive and gram-negative) compared with non-pathogenic flora in infected cirrhotics represented by low cirrhosis dysbiosis ratio (CDR) with increasing dysbiosis related to severity of liver disease. They speculated that this increased dysbiosis may potentiate the complications of the cirrhosis including infections. Bajaj et al in another study looked at the effects of rifaximin on stool microbial flora in patients with minimal hepatic encephalopathy and did not find any significant difference in overall composition of stool microbial flora after the prolonged administration (>8 weeks) of rifaximin.24 Extrapolating the results of these two studies, it is possible that the rifaximin's mechanism of action may not be linked to improving the state of intestinal dysbiosis. In a systematic review, rifaximin appears to be effective in the treatment of small-intestinal bacterial overgrowth (SIBO).25 However, the issue of SIBO as an independent risk factor for SBP is controversial as studies in the past have yielded conflicting results.26 ,27 There is some evidence based on studies involving virulent species of Escherichia coli and Shigella known to cause traveller's diarrhoea that rifaximin diminishes the expression of bacterial virulence factors as well as adherence molecules resulting in decreased cellular invasion.23 ,28 ,29 Rifaximin may also alter the host cell physiology to provide cytoprotection against bacterial invasion.30 ,31 Further investigations are needed to fully elucidate the effects of rifaximin in preventing SBP.
Rifaximin has minimal systemic side effects and is a fairly well-tolerated medication.32 It has very low absorption in healthy volunteers; however, it is significantly increased in patients with advanced liver disease, although there are no definitive data whether to recommend or to avoid its use in this population.33 Fluoroquinolones, on the other hand, are readily absorbed and may have notable systemic side effects. Serious ones include tendinopathies and QTc prolongation, predisposing to life-threatening arrhythmias.34 These side effects are more common with ciprofloxacin than norfloxacin, owing to its higher systemic absorption.35 Trimethoprim-sulfamethoxazole, the other agent that has been used for SBP prophylaxis, has an unfavourable side-effect profile as well, with hyperkalaemia, hypersensitivity reactions and cytopenias being the limiting ones.36 The dual use of one single agent for prevention of both hepatic encephalopathy and SBP in the same patient makes rifaximin an ideal choice in this setting. Randomised trials and systematic reviews have clearly demonstrated its benefits in the treatment and prevention of hepatic encephalopathy.37 ,38
The high cost might limit the use of rifaximin. A cost and outcome analysis of using rifaximin ± lactulose for hepatic encephalopathy, in addition to norfloxacin for SBP prophylaxis, compared with using rifaximin ± lactulose alone would be of clinical interest. Additionally, it is worth mentioning that Assem et al16 proposed an alternating regimen of norfloxacin and rifaximin, which presumably has differing bioeffects on the body and had better efficacy than norfloxacin.
There are several limitations to our review. The number of studies and the patient groups in each study are independently small. Elfert et al presented data regarding SBP as per-protocol treatment analysis. However, lost to follow-up information was explicitly stated in the study, thus minimising the risk of bias. There is clinical heterogeneity among the individual studies, particularly in relation to the indication for SBP prophylaxis (primary vs secondary) and the aetiology of chronic liver disease. Our conclusion may only be applicable to a particular group of patients with ascites, notably that the vast majority of included patients had hepatitis C-related cirrhosis. There is some literature suggesting that alcoholic cirrhotics are at a higher risk of bacterial infections than patients with non-alcoholic cirrhosis.39 Whether a particular cause of cirrhosis leads to a higher risk of development of SBP is still largely unknown and requires further investigation.40 These studies are incidentally from the same geographic region and thus the results may not be applicable to the demographics and characteristics of cirrhotics in the Western world, where other aetiologies such as alcohol may be more prevalent.
Conclusion
Moderate-quality evidence (per the GRADE system41) shows that the use of long-term rifaximin could be considered as a reasonable alternative to norfloxacin for patients with a qualifying indication for SBP prophylaxis in hepatitis C-related chronic liver disease. With the growing evidence of its use for hepatic encephalopathy,42 it may be an attractive choice to improve compliance in using a single antibiotic for dual purposes. Further high-quality, higher powered studies are required to firmly establish rifaximin as the first-line therapy for SBP prevention.
References
Footnotes
Contributors GSS and AG conceptualised and designed the study. GSS, HRM and SAP were involved in literature research. GSS, HRM, SA and SAP acquired and interpreted data. GSS, AG, HRM, SA and SAP drafted the manuscript. GSS, HRM, BMA, AG, SA and SAP revised the manuscript for important intellectual content. All authors approved the final version of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.