Article Text

Abstract
Objective Concomitant non-alcoholic fatty liver disease (NAFLD) and coeliac disease (CD) have not been adequately studied. This study investigated the frequency of CD among NAFLD patients and the clinicopathological and immunological patterns and outcome of concomitant NAFLD and CD.
Design This prospective longitudinal study screened patients with NAFLD for CD (tissue transglutaminase antibodies (TTGA); anti-TTGA and antiendomysial antibodies (EMA)). Patients with concomitant NAFLD and CD and patients with either NAFLD or CD were enrolled and followed. Duodenal biopsy, transient elastography, tumour necrosis factor (TNF)-alpha, transforming growth factor-beta, interleukins (ILs) 1, 6, 10, 15 and 17, folic acid and vitamins B12 and D were performed at baseline and 1 year after gluten-free diet (GFD).
Results CD was confirmed in 7.2% of patients with NAFLD. Refractory anaemia and nutritional deficiencies were frequent in patients with concomitant NAFLD and CD who had advanced intestinal and hepatic lesions, higher levels of TNF-α, IL-15 and IL-17 compared with patients with CD and NAFLD. Patients concomittant CD and NAFLD showed clinical response to GFD, but intestinal histological improvement was suboptimal. Combining EMA-IgA or anti-TTGA with either IL-15 or IL-17 enhances the prognostic performance of both tests in predicting histological response to GFD.
Conclusion Concomitant NAFLD and CD is not uncommon. Recurrent abdominal symptoms, refractory anaemia, nutritional deficiencies in patients with NAFLD warrant screening for CD. The study has important clinical implications since failure in diagnosing CD in patients with NAFLD patients results in marked intestinal and hepatic damage and suboptimal response to GFD that can be alleviated by early diagnosis and initiation of GFD.
- celiac disease
- nonalcoholic steatohepatitis
- cytokines
- gluten free diet
- small intestinal biopsy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Non-alcoholic fatty liver disease (NAFLD) may be associated with coeliac disease (CD) in some patients.
The intestinal abnormalities in CD may contribute to NAFLD pathogenesis.
What are the new findings?
This large prospective study identified a set of clinical symptoms and signs that raise the clinical suspicion of CD and warrant testing and identified non-invasive markers that allow better monitoring of response to GFD.
Patients with concomitant NAFDL and CD achieve similar clinical improvement after adherence to gluten free diet. However, histological intestinal improvement is less and delayed in patients with concomitant NAFLD and CD.
How might it impact on clinical practice in the foreseeable future?
The study findings may result in better earlier diagnosis and management of CD among patients with NAFLD to improve the outcome and prevent complication of both diseases.
Affordable alternatives of gluten-containing foods will be produced according to the economic status of different communities
Introduction
Non-alcoholic fatty liver disease (NAFLD) is a major cause of chronic liver disease worldwide.1 2 The estimates of the worldwide prevalence of NAFLD ranges from 6.3% to 33%, with a median of 20% in the general population, based on the assessment method.3 However, the estimated prevalence of non-alcoholic steatohepatitis (NASH) is lower, ranging from 3% to 5%3 with prevalence rates of 20%–25% in Western countries and 25%–40% in the Middle East.3–7 NAFLD is an important cause of chronic liver disease in Egypt and Arabian Gulf countries such as Kingdom of Saudi Arabia (KSA), Bahrain and United Arab Emirates (UAE) in adults and paediatric due to the high prevalence of risk factors such as obesity, diabetes mellitus, dyslipidaemia and metabolic syndrome in these countries.8–12 The prevalence of NAFLD ranges between 10% and 15%, between 17% and 52% and between 8% and 11% in Egypt, KSA and UAE, respectively.7–13 NAFLD encompasses a spectrum of conditions ranging from hepatic steatosis, to NASH, to advanced liver fibrosis and cirrhosis.1 Histologically, NAFLD is categorised into non-alcoholic fatty liver (NAFL) and NASH. NAFL is defined as the presence of hepatic steatosis with no evidence of hepatocellular injury in the form of ballooning of the hepatocytes. NASH is characterised by the presence of hepatic steatosis and inflammation with hepatocyte injury (ballooning) with or without fibrosis.14 Several metabolic, genetic, inflammatory and environmental factors are involved in the pathogenesis of NAFLD.14–17
Coeliac disease (CD), the most frequent food intolerance in the world, is a chronic immune-mediated entropathy resulting from abnormal response to gluten leading to injury to the small intestine, chronic malabsorption, macronutrient and micronutrient deficiencies and a wide range of intestinal and extraintestinal manifestations.18–20 Active CD (aCD) may present with abdominal symptoms of different intensity.18 19 However, CD may be silent or latent in some instances.18–21 The prevalence of CD varies between countries and populations. In Europe and the USA, the mean frequency of CD in the general population is approximately 1%22 23 but reaches 1.5%, 1.8%, 2%, 3% in Italy, San Marino, Finland and Sweden, respectively.24–26 Few reports suggested that CD is a common disorder in some North African and Middle Eastern countries26–32; however, the diagnostic rate is still very low in these countries, mostly due to low availability of diagnostic facilities and poor disease awareness. The prevalence and features of CD in Egypt are not clear, and the diagnosis of CD is often missed particularly among adults.
Some studies reported an association of CD with NAFLD.33–39 A study33 showed that patients with NAFLD have 8.6-fold increased risk of CD (95% CI 5.5 to 13.3). Another study demonstrated that 3.4% of studied patients with NAFLD had proven CD.39 However, neither the characteristics nor the significance of such association has been adequately investigated. Therefore, we conducted this prospective, longitudinal, parallel-group, multicentre study to assess the frequency, clinicopathological manifestations, cytokine responses, NAFLD and CD outcome and management in a well-characterised cohort of patients with concomitant CD and NAFLD in addition to patients with either NAFLD alone or CD. We also evaluated the diagnostic and prognostic performance of some serum cytokines for detection of CD in patients with NAFLD and prediction of the response to gluten-free diet (GFD).
Patients and methods
Study design and study population
The current study consists of an initial cross-sectional screening phase followed by a prospective, longitudinal, parallel-group phase. The study was conducted in several Egyptian centres in Cairo, delta and upper Egypt (Ain Shams University Hospitals, Cairo, and gastroenterology centres in Cairo and Minya) and PSAU University Hospital from September 2011 to September 2016. The study protocol and patients’ informed consent were approved by the institutional review boards and independent ethics committees at the participating sites. The study was conducted in accordance with the Declaration of Helsinki and was consistent with the International Conference on Harmonization and Good Clinical Practice.
Hepatic steatosis grades were assessed by ultrasound (Philips EPIQ7G ultrasound machine; Philips, Reedsville, Pennsylvania, USA) based on visual analysis of the intensity of the echogenicity, provided that the gain setting is optimum. Steatosis is considered grade I (mild) when the echogenicity is slightly increased. In grade 2 (moderate) steatosis, the echogenic liver obscures the echogenic walls of portal vein branches. In grade III (severe steatosis), the echogenic liver obscures the diaphragmatic outline.40 41
Patients with ultrasound findings suggestive of NAFLD/NASH were further tested using ‘NAFLD liver fat score (NAFLD-LFS)’,42 ‘Fatty Liver Index (FLI)’43 and ‘Hepatic Steatosis Index (HSI)’44 and were then calculated according to the previously described formulas. Other causes of liver disease and hepatic steatosis were excluded by relevant tests (online supplementary material) .
Supplementary file 1
Patients were enrolled in the study if they fulfilled the following criteria: (1) presence of hepatic steatosis; (2) NAFLD-LFS values >−0.640, FLI values >60 and HSI values >36; (3) absence of any evidence of other chronic liver diseases and other causes of hepatic steatosis; (4) no history of significant alcohol consumption and (5) elevated aminotransferase levels found in one of three situations. Patients fulfilling the inclusion criteria were further evaluated for liver stiffness (LS) and fibrosis assessment by transient elastography (TE). Serial transient elastography (TE; Fibroscan, Echosens, Paris, France) at enrolment and follow-up as previously described and the results were reported in kilopascals (kPa).45
Screening for CD
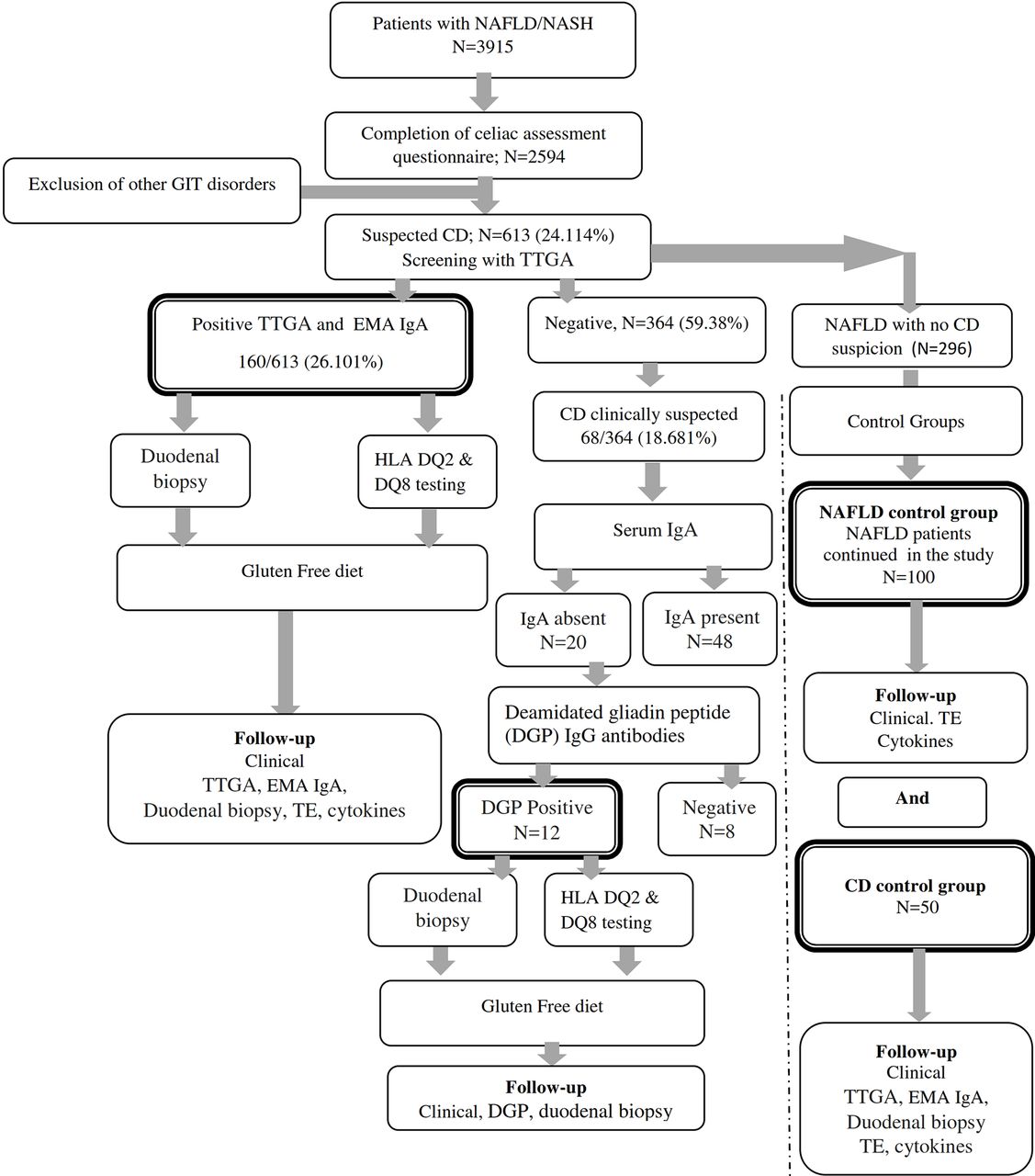
Figure 1 summarises the flow of patients through the study phases. Patients with NAFLD/NASH provided written informed consents before the screening phase of the study. Patients were invited to complete a validated Arabic version questionnaire adapted from the Coeliac UK assessment tool46 in addition to an Arabic locally validated food-frequency questionnaire that captures food intake and dietary intake over 7 days. Patients were then screened by tissue transglutaminase antibodies (TTGA; QUANTA Lite human-TTGA ELISA kit; INOVA Diagnostics, San Diego, California, USA) in which TTGA antibody titres greater than 10 U/mL were considered positive. Antiendomysial antibodies (EMA) (antiendomysial antibody IgA (EMA IgA, ELISA Kit; Biosource, San Diego, California, USA) were used for confirmation of results. Patients with symptoms suggestive of CD but negative TTGA/EMA results were tested for potential IgA deficiency (Abcam human IgA ELISA Kit). Serum IgA concentration <0.07 g/L was considered as IgA deficiency. Patients with IgA deficiency were screened by deamidated gliadin peptide (DGP) IgG antibody (DGP IgG ELISA kit). The cut-off levels for positive DGP IgG was 20 U/mL.

Flow of patients through the trial. CD, coeliac disease; DGP, deamidated gliadin peptide; EMA IgA, endomysial antibody IgA; GIT, gastrointestinal disorders; HLA, human leukocyte antigen; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; TE, transient elastography; TTGA, tissue transglutaminase antibody.
Patients with positive anti-TTGA, EMA IgA or DGP were informed that they may have CD and were invited to join the study and undergo further investigations. Those who accepted to be enrolled in the study signed another informed consent before entry and before any study-related investigation or upper endoscopy. Enrolled patients completed an Arabic version of the Gastrointestinal Symptom Rating Scale questionnaire (online supplementary material).47 Enrolled patients were subjected to careful history, clinical examination, laboratory investigations, fasting insulin and fasting glucose, homeostasis model assessment-insulin resistance (HOMA-IR),48 serum iron, ferritin, folic acid, vitamins D and B12, antinuclear antibodies, thyroid function tests, cytokine assessment and gastrointestinal endoscopy with duodenal biopsy. Lactose intolerance was assessed by lactose tolerance test and lactose hydrogen breath test as previously described.49 DQB1*02 and DQB1*0302 typing (PCR sequence-specific oligonucleotide typing (QIAxcel system and QIAxcel DNA Fast Analysis Kit Product # 929008, QiagenI, Stamford, Connecticut, USA) was performed in a subset of patients.
Cytokines assessment
Tumour necrosis factor-alpha (TNF-α), interleukin (IL) 1, IL-6, IL-10, IL-15 and IL-17 (ELISA Kits, Biosource) and YKL-40 (human YKL-40 ELISA kit, Quidel, San Diego, California, USA) were measured at baseline and end of follow-up according to the manufacturers’ instructions (online supplementary material).
Endoscopy and small intestinal biopsy
At baseline, all patients with serological evidence of CD had upper endoscopy and duodenal biopsy, which were repeated 1 year after GFD in a subset of patients who agreed to the follow-up endoscopy. At least six mucosal biopsies were taken from the second part of duodenum and bulb. Sections were stained with H&E and Giemsa and were examined by an experienced gastrointestinal pathologist (author: LN) according to the Modified Marsh classification for CD50 (online supplementary material). Villous atrophy was defined as a Marsh 3 lesion or villous height: crypt depth ratio below 3.0.
Initiation of GFD, monitoring GFD adherence and assessment of response to GFD
Patients diagnosed with CD were informed about the disease and the importance and benefits of following a lifelong GFD. A full nutritional consultation and information sheet including detailed diet regimen and different affordable, easily prepared gluten-free food items were provided to all patients. Adherence to GFD was assessed during clinical visits scheduled every 3 months. During each visit, GFD compliance was assessed by follow-up of initial symptoms or the appearance newly developed ones in addition to completing an Arabic version of Gluten-Free Diet Compliance Questionnaire51 (online supplementary material). After 1 year of GFD, patients repeated EMA IgA or DGP, cytokines, performed follow-up biopsy and TE. Complete clinical improvement was defined as the complete resolution of baseline symptoms after 1 year of GFD. Clinical partial improvement was defined as a resolution of at least 50% of the baseline symptoms after 1 year of GFD. Complete histological improvement is defined as resolution of villous atrophy associated with the absence of crypt hyperplasia and ≤40/100 intraepithelial lymphocytes. Partial histological recovery is defined as improvement of at least one grade on the Marsh classification compared with the initial histology.
Statistical analysis
Baseline demographic and clinical characteristics were analysed descriptively for all patients using Student’s t tests, analysis of variance (ANOVA) or Kruskall-Wallis test as appropriate for continuous variables and χ2 or Fisher’s exact tests were used for categorical variables. Cytokine levels were examined in box plots as continuous variables. A Kruskal Wallis one-way ANOVA test tested for a significant overall shift in cytokine levels in cases and controls, and the Mann-Whitney U test examined identified sample pairs. Comparison of cytokine levels and upper endoscopy findings before and after GFD was assessed by paired t-test. Pearson r correlation test was used to assess the relation between cytokines levels and Marsh class. Using Wilson method, the 95% CIs of the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. Logistic regression was used to predict CD among patients with NAFLD. Results are expressed as mean values±SD. Statistical analysis was performed using SPSS V.22, GraphPad Prism software (GraphPad Software, La Jolla, California, USA) and Med Calc Statistical software (MedCalc Software, Ostend, Belgium).
Results
Of the 2542 patients with hepatic steatosis who completed the screening questionnaire, 1873 (73.78%) patients fulfilled the criteria of NAFLD and 669 (26.32%) had NASH (data not shown). CD was suspected in 613/2542 patients who were screened by anti-TTGA, which was positive in 160/613 (26.101%) patients. Patients were further tested by EMA IgA. Despite negative TTGA and EMA, CD was still clinically suspected in 68 patients (11.093%). Those patients were tested for serum IgA and DGP IgG antibodies. DGP was positive in 12/68 (17.647 %) tested patients. Thus, serodiagnosis identified 182 NAFLD patients with CD, which represents 7.2% of the patients with NAFLD who completed the initial screening questionnaire. Patients with concomitant NAFLD and CD comprised group A (n=182), patients with NAFLD alone comprised group B (n=100) and 50 patients with proven CD were enrolled in group C.
Patients’ demographics, clinical characteristics and laboratory results
Patients with concomitant CD and NAFLD had significantly lower BMI than those with NAFLD alone (p<0.0001). CD was symptomatic in 123 (67.7%) and 44 (88%) in groups A and C patients, respectively, while silent coeliac was detected in 56 (30.8%) and 6 (12%) patients in groups A and C patients, respectively (table 1). Recurrent bloating, diarrhoea, abdominal pain dyspepsia and nausea were frequently reported by patients with CD with or without NAFLD (table 1). Such abdominal symptoms in NAFLD patients strongly suggested CD (OR: 10.2784; 95% CI 5.9099 to 17.8760; p<0.0001). Dermatitis herpetiformis was detected in 67 (36.8%) and 20 (40%) patients in groups A and C, respectively. Oral ulcers/angular stomatitis occurred in 92 (50.5%) and 21 (42%) of patients with CD with or without NAFLD, respectively (table 1) and strongly predicted CD in patients with NAFLD (OR: 19.4222, 95% CI 7.5483 to 49.9743; Z statistics: 6.152; p<0.0001). Clinical symptoms suggestive of lactose intolerance with positive lactose tolerance test were detected in 15 (8.24%) patients with concomitant coeliac and NAFLD versus 17 (34%) patients with CD (p<0.001). Coeliac crisis with severe diarrhoea and electrolyte disturbances requiring hospitalisation was the presenting symptom in five patients (2.747%) with concomitant NAFLD and CD (who were not aware that they had CD) versus one patient (2%) with proven CD who had a gluten-rich diet. Thyroiditis and diabetes mellitus showed no significant differences in the three groups.
Demographics and baseline clinical characteristics and laboratory data of patients with concomitant NAFLD and CD
Patients with concomitant NAFLD and CD had significantly higher serum bilirubin, alanine aminotransferase (ALT) and asparta aminotransferase (AST), cholesterol and triglyceride levels and HOMA-IR compared with groups B and C. Patients with CD with or without NAFLD showed low haemoglobin, serum iron, ferritin, folic acid, vitamin D and vitamin B12 compared with patients with NAFLD alone (p<0.0001 for all) (tables 1 and 2). The following findings were significantly associated with CD in patients with NAFLD: haemoglobin levels <10 gm/dL (OR: 9.8358; 95% CI 5.6457 to 17.1355; p<0.0001), iron levels <60 µg/dL (OR: 13.0473; 95% CI 7.4001 to 23.0038; p<0.0001), folic acid levels below 2 ng/mL (OR: 11.0968; 95% CI 6.2783 to 19.6134; p<0.0001) and vitamin B12 levels below 200 pg/mL (OR: 6.4286; 95% CI 3.8458 to 10.7460; p<0.0001). DQ2 and DQ8 were positive in 51 (91.07%), 42 (42%) and 5 (8.93%) patients in groups A, B and C, respectively.
Serum iron, folic acid, vitamins, EMA IgA, TTGA and cytokine levels at baseline and after GFD in patients with concomitant NAFLD and coeliac disease versus patients with coeliac disease control group
Clinical response to GFD in patients with concomitant NAFLD and CD versus patients with CD alone
Complete clinical improvement after GFD was achieved in 159 (87.363%) and 47 (94%) patients in groups A and C, respectively (p=0.3092). Partial improvement was detected in 18 (9.89%) and 3 (1.648%) patients in groups A and C, respectively (p=0.5813). Five patients with concomitant NAFLD and CD showed refractory CD (data not shown). Adherence to GFD resulted in clinical improvemnt as well as improvement in the nutritional parameters such as serum iron, folic acid and vitamins B12 and D (table 2).
Baseline and follow-up intestinal biopsy
At baseline, Marsh stage 3 (a, b and c) intestinal changes were detected in 181 (99.45%) and 47 (94%) patients in groups A and C, respectively (p=0.0323) (table 3). Thus, according to clinical manifestations, serology and baseline intestinal biopsy, patients with CD were classified into: (1) symptomatic CD with manifestations related to coeliac with positive serology and histological manifestations in intestinal biopsy; (2) silent CD with no or minimal symptoms, ‘damaged’ mucosa and positive serology; and (3) latent CD with positive serology but with normal intestinal mucosa and no symptoms (table 1). After 1 year of GFD, intestinal biopsy was performed in 101 patients with concomitant NAFLD and CD and 42 patients with sole CD. Complete histological improvement was achieved in 13 (12.87%) and 42 (84%) patients in groups A and C, respectively (p<0.0001). Partial histological improvement was detected in 79 (78.217%) and 8 (16%) patients in groups A and C, respectively (p<0.001). No improvement was detected in nine (8.91%) patients with concomitant NAFL and CD (table 3).
Modified Marsh Classification of histological findings (Oberhuber) in patients with concomitant CD and patients with CD alone at baseline and after GFD
Baseline and follow-up serum TTGA, EMA and cytokines
At baseline, anti-TTGA, IL-1, TNF-α, IL-6, IL-15, IL-17 cytokines were significantly higher in patients in groups A and C compared with those in group B (table 2, figure 2). TTGA, EMA, TNF-α, IL-15 and IL-17 titres correlated swith the severity of intestinal lesions in groups A and C patients (figure 3). TGF-β and YKL-40 were significantly higher in patients with NAFLD with or without CD compared with those with NAFLD alone (p<0.0001) (figure 2B) with significant differences between patients with concomitant NAFLD and CD and NAFLD alone (TGF-β: p=0.005, YKL-40: p=0.001). As shown in table 2, clinical improvement was associated with significant reduction in TTGA, IL-1, TNF-α, IL-6 as well as IL-15 and IL-17.
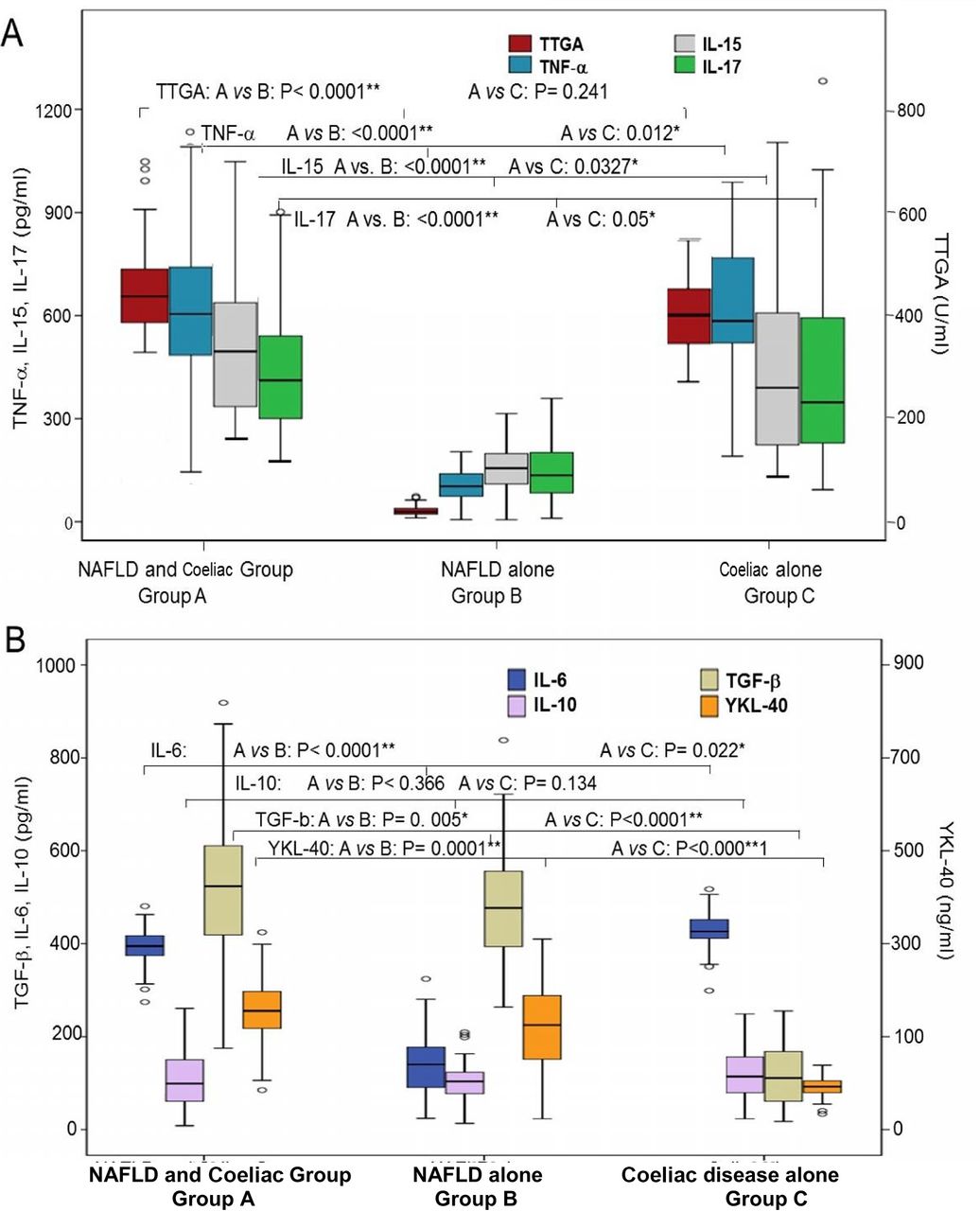
Baseline cytokines in the three groups. (A) Baseline TTGA, TNF-α, IL-15 and IL-17 and (B) IL-6, IL-10 and TGF-β and YKL-40 in patients of the three groups. Group A: concomitant NAFLD and coeliac disease (n=182); group B: NAFLD (n=100); group C: coeliac disease (n=50). In the box plot, the black centre line represents the median for each dataset. The first and third quartiles (IQR) are located at the edges of the box. The points represent outliers. *Significant. **Highly significant. IL, interleukin; NAFLD, non-alcoholic fatty liver disease; TNF-α, tumour necrosis factor-alpha; TGF-β, transforming growth factor beta; TTGA, tissue transglutaminase antibody; YKL-40: chitinase-3-like-1 human cartilage glycoprotein-39.

Correlation between individual cytokines and Modified Marsh classification for coeliac disease that assesses the intraepithelial lymphocytes per 100 enterocytes (IEL/100 enterocytes), crypt hyperplasis and villi.42 IL, interleukin; TNF-α, tumour necrosis factor-alpha; TTGA, tissue transglutaminase antibody.
Diagnostic performance of TTGA, EMA IgA and serum cytokines in predicting CD in patients with NAFLD
Considering histological changes in intestinal biopsy as the gold standard for diagnosis of CD, we assessed the diagnostic performance of TTGA, EMA IgA and the tested cytokines. EMA IgA, IL-17, TTGA, TNF-α and IL-15 showed the high sensitivity, specificity, PPV and NPV in predicting the status of CD (Table 4). Combining the results of EMA IgA and TTGA with either TNF-α, IL-15 or IL-17 further improved the diagnostic performance of such cytokines (table 4).
Diagnostic performance of different antibody tests and cytokines in predicting coeliac disease in patients with NAFLD
Impact of CD in liver histology and hepatic fibrosis progression
Baseline and follow-up LS values and TGF-β and YKL-40 levels showed significant differences between groups A, B and C patients. At the end of follow-up, more patients with concomitant NAFDL and CD progressed to NASH than patients with NAFLD alone (figure 2b, figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Baseline and follow-up transient elastography (TE) in patients with concomitant NAFLD and coeliac disease (n=182; group A), patients with NAFLD (n=100; group B) and patients with coeliac disease alone (n=50; group C). NAFLD, NAFLD, non-alcoholic fatty liver disease.
Discussion
Given that the features and outcome of concomitant NAFLD and CD are not adequately investigated, we conducted the current prospective longitudinal study to investigate the frequency of CD among adult patients with NAFLD and investigate the clinical, histological and immunological features as well as the management of these patients.
In the current study, CD was diagnosed by TTGA/EMA IgA or DPG and intestinal biopsy in 7.2% of our patients with NAFLD, which is within the range of 2%–14% that was reported in previous studies.33–36 38 Although two-thirds of patients with concomitant NAFLD and CD had gastrointestinal symptoms of varying intensity, CD was neither diagnosed or suspected prior enrolment in the study due to either low awareness of celiac disease or the unavailability and high costs of CD diagnostics. In the current study, undiagnosed recurrent bloating, repeated diarrhoea with or without angular stomatitis or dermatitis herpetiformis or suboptimal BMI (<24) or refractory anaemia, nutritional (vitamin B12, vitamin D and folic acid) in patients with NAFLD deficiencies were associated with high likelihood of CD and represented important warning signs raising the clinical suspicion of CD in patients with NAFLD and warranting screening.
The advanced intestinal inflammation and villous atrophy and higher levels of proinflammatory cytokines observed in our patients with concomitant NAFLD and CD suggest advanced intestinal injury in such patients compared with those with sole CD. Also, patients with concomitant NAFLD and CD had higher levels of hepatic steatosis, LS, hepatic fibrosis progression rates and profibrotic mediators compared with those with either NAFLD or CD alone. Such differences in severity of intestinal and hepatic damage may have several potential explanations. The previous diagnosis of coeliac enteropathy in several patients with sole CD and the initiation of GFD at some time point (despite lack of GFD strict compliance in the majority of patients) may have reduced intestinal lesions to some extent. In contrast, none of our patients with NAFLD was previously diagnosed with coeliac so patients pursued consuming typical Egyptian gluten-rich diet resulting in ongoing enteropathy, significant intestinal damage with release of proinflamatory cytokines, increased intestinal permeability and gut bacteria dislocation.52 53 The intestinal microbiome may increase influx of fatty acids intestinally derived toll-like receptor 4 and toll-like receptor 9 agonists into the efflux of the liver through the portal circulation which, in turn, activate hepatic TNF-α mediating the pathogenesis of NAFLD and its progression to NASH.53 Another explanation may be that patients with concomitant NAFLD and CD initially developed hepatic steatosis (due various risk factors), which represented the primary hit and CD gut-derived endotoxaemia represented the second hit that accelerated progression of NAFLD.37 54
Initiation and compliance to a GFD has been a real challenge in the current study. Gluten-containing foods are the cornerstone of the typical Egyptian diet characterised by inclusion of wheat and bread in almost all Egyptian meals. GFDs are rarely available in the Egyptian market, and if found they are extremely expensive and beyond the reach of the majority of patients. In the current study, it was mandatory to provide patients with detailed nutritional consultation and recipes of affordable GFDs from corn and rice flour. In the current study, CD patients with or without NAFLD showed significant clinical improvement after adherance to GFD. However, complete histological recovery was less or delayed in patients with concomitant NAFLD and CD. This might be due to consumption of minimal amounts of gluten or due to potential cross-contamination while preparing food or due to the more baseline advanced intestinal damage in patients with concomitant NAFLD and CD.
To date, histology of intestinal biopsy is the gold standard for the diagnosis of CD and confirming complete response to GFD in many regions because other diagnostic procedures maybe unavailable.55 However, upper endoscopy is an invasive, expensive procedure, and repeating endoscopy for follow-up of the response of patients to GFD is inconvenient to many patients. Thus, we investigated the clinical utility of other potential non-invasive methods for screening, diagnosis and follow-up of CD. The current study showed that anti-TTGA was a good screening test with reasonable sensitivity, specificity, PPV and NPV; however, EMA IgA may be beneficial in confirming CD in anti-TTGA positive cases particularly in patients with concomitant NAFLD/NAASH. Some studies showed false-positive TTGA results in patients with connective tissue disorders, inflammatory bowel diseases and in chronic liver disease of different aetiologies. False-positive results of human TTGA in chronic liver disease may arise from evoking an immune response that is to some degree related to the amount of liver fibrosis probably because of the hepatic expression of TTGA.56–59 A study showed that that TTGA may play a role in the course of hepatic repair following a prolonged toxic injury, stress-induced damage and may be expressed in the progression of liver damage. However, the current study showed that EMA followed by TTGA with IL-17 or IL-15 have better sensitivity, specificity, PPV and NPV and more accuracy in predicting histological response to GFD than TTGA alone. Comparing the costs and benefits of endoscopic intestinal biopsy with EMA IgA or TTGA with cytokine use favours serology.
In accordance with previous studies,19–21 HLA DQ2 and DQ8 were detected in our CD patients with or without NAFLD. Although the current study shows that HLA DQ2 seems less prevalent in patients with concomitant NAFLD and CD, it is hard to make reliable conclusions since HLA phenotyping was performed only in a subset of patients. Taken together, HLA testing may not be incorporated as a routine diagnostic procedure for CD, particularly in resource-limited countries since it does not reflect the activity of the disease and adds to the costs of diagnosis.
The current study has several strengths such as the prospective longitudinal design, the well-characterised cohort, the comprehensive assessment of clinical, histopathological, immunological characteristics of patients with concomitant NAFLD and CD and the long follow-up. The study provided a set of clinical warning signs and non-invasive diagnostic and prognostic methods for detection of CD and in monitoring the response to GFD. The study also demonstrate the negative impact of CD on NAFLD. However, the study also has some limitations including screening patients for CD according to self-reported symptoms so latent CD may have been missed. Post-GFD intestinal biopsies were performed in a subset of patients who approved endoscopy. However, the missing follow-up intestinal biopsy results in some patients were statistically handled. Liver biopsies were not performed, and diagnosis of NAFLD depended on ultrasound and the FLI and HSI. Given the high prevalence of NAFLD in general population, it may be argued that the presence of NAFLD in patients with CD can be accidental, which cannot be entirely ruled out in the current study. Some studies28–30 55 showed that the frequency of CD in the general population is 0.53% and 6.4% among at-risk groups. However, large studies are needed to accurately assess the true prevalence of CD in patients with NAFLD and NASH in comparison with its prevalence in the general population.
Taken together, our study provided important new data that have various clinical implications. Our study showed that CD is not uncommon among patients with NAFLD but is often missed or ignored. The study identified a set of clinical warning signs and non-invasive biomarkers that increase the identification of CD in patients with NAFLD and monitoring of both diseases. Concomitant NAFLD and CD may have advanced intestinal damage and more advanced forms of NAFLD suggesting that both disorders have negative impact on each other. Thus, current study highlighted the importance of early detection and management of CD in patients with NAFLD to improve the outcome and reduce complications of both disorders.
Acknowledgments
The authors are grateful to the Deanship of Scientific Research at Prince Sattam bin Abdulaziz University. The authors would like to thank Dr Yasmin Massoud for her contribution in enrollment, clinical examination and follow-up of the patients.
References
Footnotes
Contributors All authors contributed in clinical work, patient enrolment, data collection, data entry and writing of the manuscript.
Funding This study is funded by Prince Sattam bin Abdulaziz University (grant no: PSAU291625), Ain Shams University (grant no: R-2094-2011), Science & Technology Development Fund (STDF) (grant no: STDF/384/2011-2015).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ain Shams University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional anonymous unpublished data from the study are available. The data may be accessed by the investigators.