Article Text

Abstract
Objective Although the reasons for secondary loss of response to infliximab (IFX) maintenance therapy in Crohn’s disease vary, dose intensification is usually recommended. This study investigated the cost-effectiveness of interventions defined by an algorithm designed to identify specific reasons for therapeutic failure.
Design Randomised, controlled, single-blind, multicentre study. 69 patients with secondary IFX failure were randomised to IFX dose intensification (5 mg/kg every 4 weeks) (n=36) or interventions based on serum IFX and IFX antibody levels using the proposed algorithm (n=33). Predefined co-primary end points at week 12 were proportion of patients responding (Crohn's Disease Activity Index (CDAI) decrease ≥70, or ≥50% reduction in active fistulas) and accumulated costs related to treatment of Crohn’s disease, expressed as mean cost per patient, based on the Danish National Patient Registry for all hospitalisation and outpatient costs in the Danish healthcare sector.
Results Costs for intention-to-treat patients were substantially lower (34%) for those treated in accordance with the algorithm than by IFX dose intensification: €6038 vs €9178, p<0.001. However, disease control, as judged by response rates, was similar: 58% and 53%, respectively, p=0.81; difference 5% (−19% to 28%). For per-protocol patients, treatment costs were even lower (56%) in the algorithm-treated group (€4062 vs €9178, p<0.001) and with similar response rates (47% vs 53%, p=0.78; difference −5% (−33% to 22%)).
Conclusions Treatment of secondary IFX failure using an algorithm based on combined IFX and IFX antibody measurements significantly reduces average treatment costs per patient compared with routine IFX dose escalation and without any apparent negative effect on clinical efficacy.
Trial Registration No NCT00851565.
- IBD CLINICAL
- INFLIXIMAB
- COST-EFFECTIVENESS
- CROHN'S DISEASE
- TNF
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
-
Loss of clinical effect of infliximab (IFX) maintenance therapy is common in Crohn's disease.
-
International guidelines suggest intensifying the IFX regimen in this event.
-
Measurement of IFX and IFX Abs may help to identify specific reasons for therapeutic failure.
-
A treatment algorithm based on IFX and IFX Abs has been proposed to achieve optimised therapies in individual patients.
What are the new findings?
-
Individualised therapy based on immunopharmacological evidence resulted in similar clinical response rates to the current dose intensification strategy.
-
Treatment costs were substantially reduced in patients receiving algorithm-based therapy.
-
At the time of secondary IFX treatment failure, most patients had therapeutic IFX levels, indicating a pharmacodynamic mechanism for the failure. Low IFX levels due to drug immunogenicity or non-immune-mediated pharmacokinetics were less common.
How might it impact on clinical practice in the foreseeable future?
-
Clinical interventions based on therapeutic monitoring of IFX and IFX Abs result in lower treatment costs with similar clinical outcomes.
Introduction
The monoclonal antibody (Ab) to tumour necrosis factor (TNF)-α, infliximab (IFX), effectively induces and maintains remission in patients with moderate to severe luminal or fistulising Crohn’s disease that is refractory to conventional immunosuppressive agents.1 However, a substantial fraction of patients with an initial response later experience the return of active disease despite ongoing IFX maintenance therapy.2 Optimal intervention in patients with secondary IFX failure is hampered by the limited number of therapeutic options including few alternative medications.1 ,3–5 International guidelines suggest intensifying the IFX regimen in the event of treatment failure.3–5 Changing to a different TNF inhibitor or another class of biological agent, if available, optimisation of conventional immunosuppressive drugs and/or surgery may also be considered.3–5 This treatment strategy may not always be optimal, as it may take a long time to regain control of inflammatory activity, leading to increased risk of irreversible tissue damage.6 Moreover, the dose intensification strategy is obviously very expensive, and anti-TNF biopharmaceuticals, which are also extensively used for a number of other chronic inflammatory diseases, now constitute one of the heaviest medicinal expenditures in Western countries.7
To address these issues, we have proposed the algorithm shown in figure 1, in which interventions are based on a combined assessment of IFX bioavailability and immunogenicity at the time of therapeutic failure.8 The key element is to intervene in accordance with the most likely cause of the loss of effect as suggested by pharmacoimmunological evidence obtained from each individual patient. Thus, IFX levels, classified as therapeutic or sub-therapeutic, and detectable or undetectable IFX Abs, are used to assess if loss of response is more probably due to immunogenicity than to non-immune-mediated pharmacokinetic or pharmacodynamic issues. This algorithm is supported by descriptive studies, and post hoc analyses from clinical trials, reporting relatively consistent associations between serum IFX and IFX Abs levels and clinical responses,9–12 by a retrospective observational study,13 and by several other investigators.13–15 However, clinical application of this algorithm remains controversial. The present study is the first clinical trial to investigate the utility of combined drug and drug Ab measurements to optimise IFX therapies in individual patients with therapeutic failure to achieve rational, cost-effective interventions.13 ,15 ,16
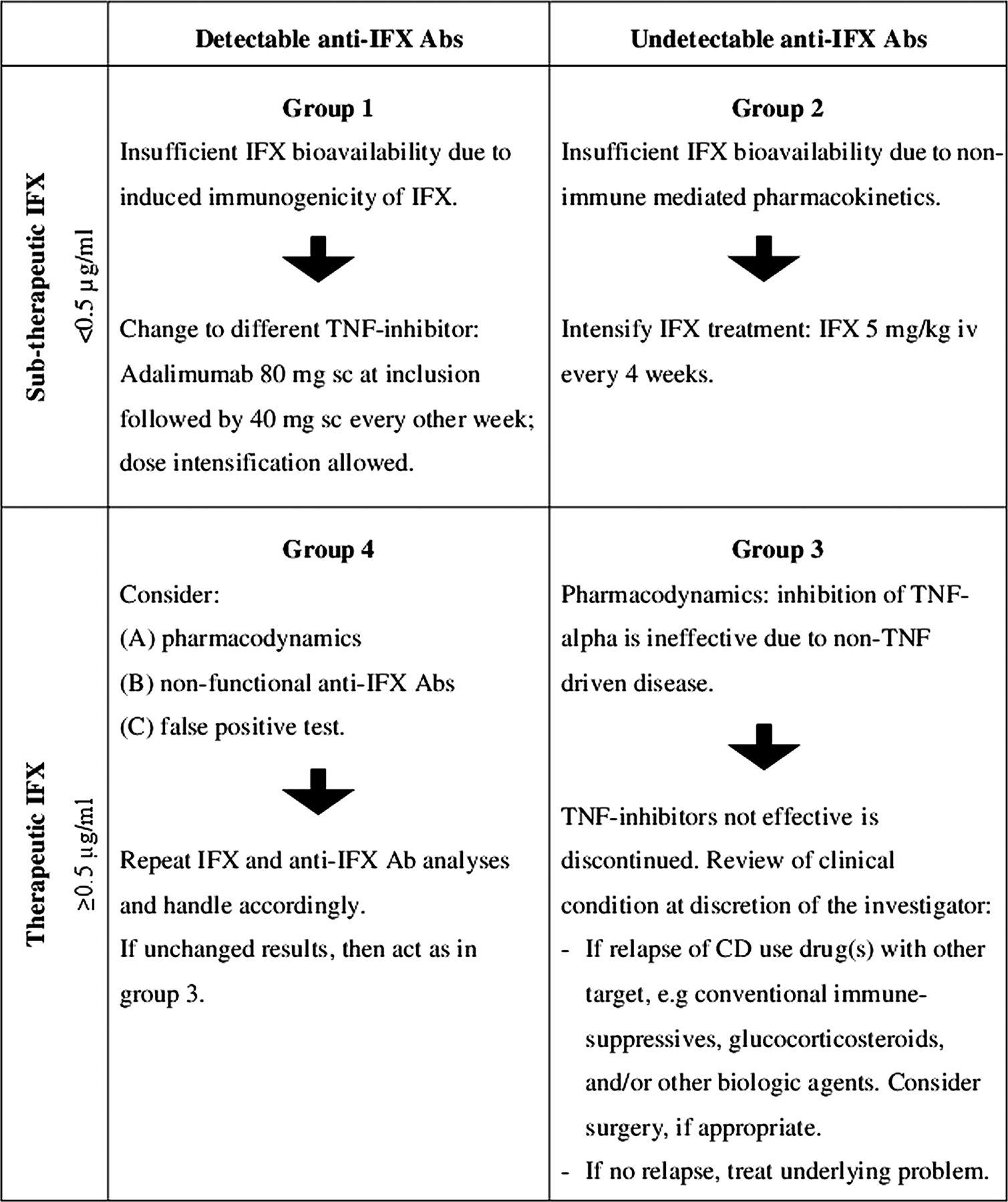
Treatment algorithm for patients with Crohn's disease (CD) with secondary loss of response to infliximab (IFX). Ab, antibody; iv, intravenously; sc, subcutaneously; TNF, tumour necrosis factor.
Methods
Study design and patients
This was a randomised, controlled, single-blind, clinical trial. Eligible adult patients had Crohn’s disease and a previous beneficial clinical response to standard IFX maintenance therapy with regular infusions of 5 mg/kg. At inclusion, all patients had secondary IFX treatment failure on IFX maintenance therapy defined as recurrence of active disease with a Crohn’s Disease Activity Index (CDAI) ≥220 and/or a minimum of one draining perianal fistula. Patients were equally randomised to receive either IFX at an increased dose frequency of 5 mg/kg every 4 weeks or treatment based on serum concentrations of IFX and IFX Abs at the time of IFX treatment failure in accordance with the algorithm in figure 1.8 Patients were allowed concomitant therapy with standard doses of thiopurines, methotrexate or antibiotics (duration ≥12 weeks) and stable dosing for ≥2 weeks of topical agents, loperamide, oral hydrocortisone (≤30 mg daily; duration ≥4 weeks) or budesonide (≤9 mg daily; duration ≥4 weeks). Exclusion criteria were any contraindication to continued IFX, short bowel syndrome, recent history of abdominal surgery or of a severe medical condition, pregnancy, or alcohol or drug abuse. Study duration was 12 weeks, with scheduled study visits at weeks 0, 4, 8 and 12. The trial was carried out at six Danish centres from June 2009 through August 2011. The study was monitored by independent Good Clinical Practice units from the Universities of Copenhagen, Aarhus and Odense. It was approved by the Danish Medicines Agency (EudraCT 2009-009926-94), the regional ethics committees (HA-2009-009) and the Danish Data Protection Agency (2007-58-0015; 750.89-2), and registered at ClinicalTrials.gov (NCT00851565; protocol summary available). All subjects gave oral and written informed consent.
Evaluations
Costs
Costs related to Crohn’s disease were defined as all costs of inpatient and outpatient contacts in hospitals related to treatment of Crohn’s disease. Data were obtained from the Danish National Patient Registry (NPR), which holds information on all patient contacts (public and private) in Danish hospitals. This unique register allows very accurate determination of medical expenses on an individual patient basis. The NPR includes administrative information, diagnoses, and diagnostic and treatment procedures. Disease-related procedures registered in combination with a diagnosis of Crohn’s disease were identified for each patient. Costs were calculated as hospitalisation and outpatient costs, weighted by use, for separate diagnosis-related groups, and specific outpatient costs (Diagnosis Related Grouping (DRG) tariffs) and obtained from the Danish Ministry of Health. Different usage of biological agents was not reflected in the tariff from NPR. Costs of contacts involving biological agents were therefore calculated separately and included drug expenses only (administrative costs were included in a sensitivity analysis). Pricing of biological agents was set to the standard price paid by all Danish hospitals as at 1 January 2012 (Amgros, Copenhagen, Denmark). A standardised IFX dose corresponding to 400 mg per infusion was used and based on the overall mean weight (72 kg) of included patients receiving IFX within the study period. Costs for each patient were calculated in Danish kroner (DKK) as accumulated costs from inclusion and converted into Euro. Expenses related to Crohn’s disease in the 12 months before inclusion were comparable between randomisation groups, and average elapsed time from inclusion until each study visit was similar.
Clinical
Patients were evaluated in the clinic and underwent physical examination at each study visit. Data were collected from diaries kept by the patients, adverse events and concomitant medications were recorded, and general laboratory tests were performed. Scores were determined on the CDAI and Short Inflammatory Bowel Disease Questionnaire (IBDQ). Perianal Disease Activity Index (PDAI) and number of draining fistulas were determined in patients with fistulising disease. Clinical response was defined as ≥70 point reduction in CDAI from baseline in luminal disease and a reduction in active fistulas of ≥50% from baseline in fistulising disease. Clinical remission was defined as an absolute CDAI score of ≤150 and complete closure of all fistulas despite gentle pressure.
End points
The primary objective was to demonstrate that treatment of patients with Crohn's disease with loss of response to IFX maintenance therapy using the algorithm shown in figure 1 was less expensive than a conventional intensified IFX regimen, without negatively affecting control of the disease. For the primary end point assessed at week 12 to be met, the accumulated costs related to treatment of Crohn’s disease, defined as mean costs per patient, needed to be significantly lower in the algorithm group. In addition, there should be no evidence that clinical response rates in the algorithm group are inferior to IFX intensification.
Analysis of serum IFX and IFX Abs
Serum samples for IFX and IFX Ab testing were collected at the time of reported IFX treatment failure. Samples were sent for immediate analysis by radioimmunoassay (Biomonitor A/S, Copenhagen, Denmark). Study intervention was based on these test results. Samples were also stored in a biobank and analysed by ELISA and homogeneous mobility shift assay (HMSA) after the study had been stopped (both at Prometheus Laboratories, San Diego, California, USA). All serum analyses were performed on the same sample material under blinded conditions.
Radioimmunoassays
IFX and IFX Abs were measured by fluid-phase radioimmunoassay as previously detailed.17 ,18 IFX levels were classified as therapeutic (≥0.5 µg/mL) or sub-therapeutic (<0.5 µg/mL), and IFX Abs as detectable or undetectable (limit of quantification (LOQ) 10 arbitrary units (U)/mL), based on previously established, clinically validated, cut-off levels based on receiver operating characteristics.18
Randomisation and masking
Randomisation was performed centrally by an independent person (block randomisation in blocks of 20; sequentially numbered opaque envelopes). Patients were blinded to randomisation group and results of serum analyses. Physicians were blinded to IFX and IFX Ab test results from patients in the IFX escalation group. Physicians were not completely blinded because they had to use the results of analyses of serum IFX and IFX Abs in the treatment of those patients who were randomised to the algorithm group.
Sample size
Sample size was based on non-inferiority of clinical response rates at week 12 in the algorithm group compared with the IFX intensification group. Mean response rate in the IFX intensification group was estimated at 50%22; a similar response rate was expected in the intervention group. A wide non-inferiority margin corresponding to half the mean estimated response rate (δ=0.25) was applied in order to reach a feasible sample size. Given these assumptions, and with two-sided α=0.05 and β=0.2, the required sample size with equal allocation was estimated at 100 patients. However, owing to time constraints, inclusion of patients was stopped after 2.5 years.
Statistical analysis
Categorical variables were compared by Fisher’s exact test or χ2 test, and continuous variables by unpaired t test or by Mann–Whitney U test depending on distribution of data. Costs were compared using arithmetic means. Statistical significance of the cost estimates was assessed by non-parametric bootstrap analysis (bootstrap-t method).23 Data were analysed in intention-to-treat and per-protocol populations. Patients who dropped out were also included in the statistical analyses at subsequent study visits using the last observations carried forward for efficacy (response and remission), CDAI, PDAI, biochemical variables and safety and by using the actual direct medical costs related to Crohn’s disease. Missing data were handled as described for dropouts: clinical data were included at week 12 only, and economic data at all study visits. Patients who were withdrawn because of lack of effect of study treatment were classified as having no response and no remission at subsequent study visits, and all other parameters were handled as described for dropouts. Patients who were withdrawn for reasons other than lack of effect of study treatment were handled as dropouts. Statistical analyses were performed in SPSS V.18, Stata 12 and GraphPad Prism V.5. Two-sided p values <0.05 were considered significant.
Results
Patients
Characteristics
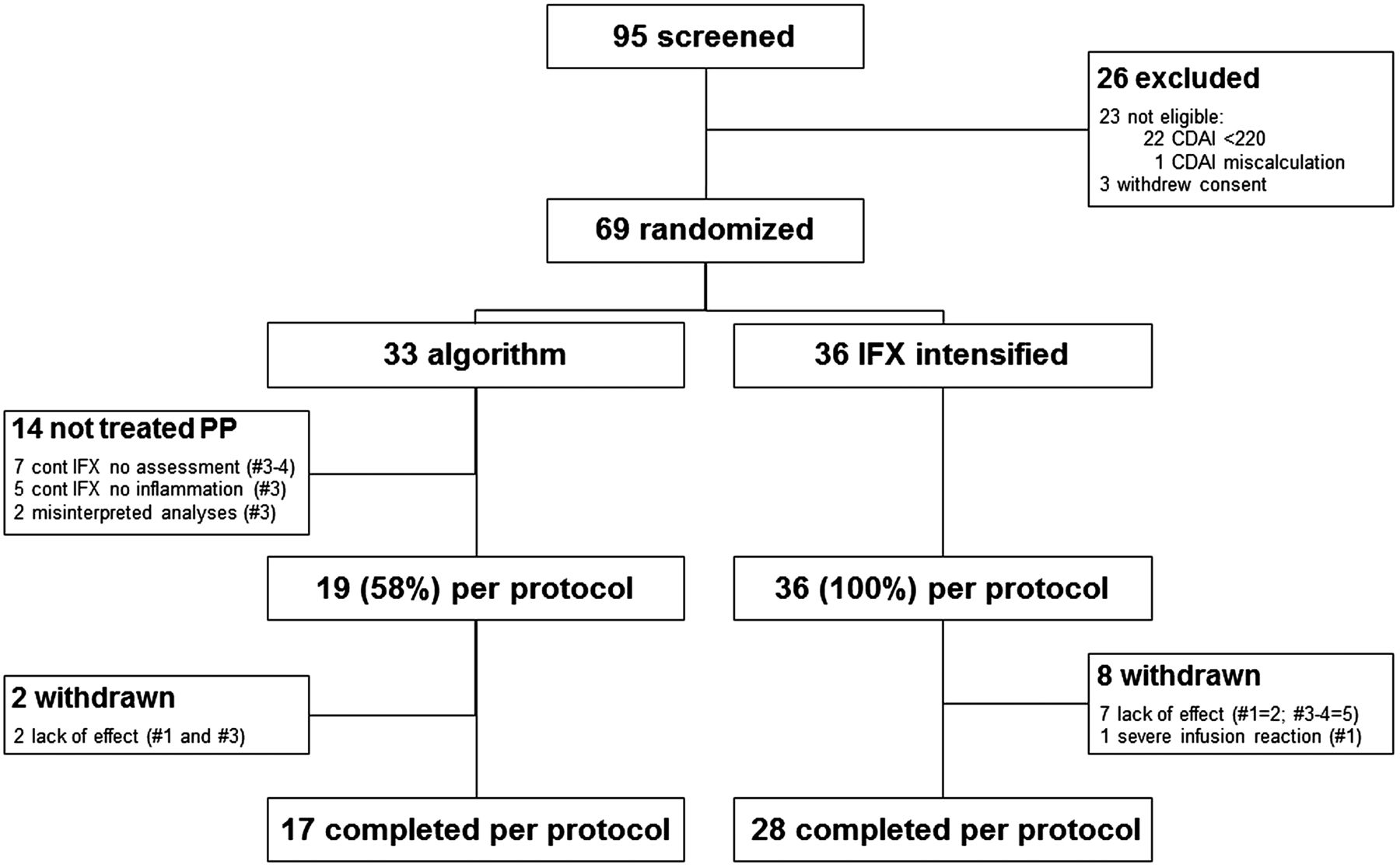
Of 69 randomised patients, 36 (52%) were assigned to IFX intensification with infusions every 4 weeks, and 33 (48%) to treatment in accordance with the algorithm shown in figure 1. Baseline characteristics were comparable between randomisation groups (table 1).
Patient characteristics
Enrolment and treatment
All patients randomised to the intensified IFX regimen were treated as outlined in the protocol (figure 2). A total of 28 (78%) completed the 12-week trial as per protocol. Withdrawals were due to insufficient effect of IFX intensification, except in one patient who developed an acute severe infusion reaction to IFX.

Enrolment and treatment of patients. # denotes grouping according to the algorithm presented in figure 1. CDAI, Crohn's Disease Activity Index; IFX, infliximab; PP, per protocol.
Among patients randomised to treatment using the algorithm, 19 (58%) were handled accordingly, and 17 of these (89%) completed the trial as per protocol (figure 2). The subgroup of patients not treated in accordance with the algorithm all had therapeutic serum IFX concentrations above the predefined cut-off (groups 3 and 4) (figure 1 and see online supplementary figure) and should therefore have been evaluated for aetiology of reported symptoms, and treated in accordance with these findings but without use of anti-TNF biopharmaceuticals. However, IFX was continued on clinical grounds without assessment of disease activity or despite inactive disease (figure 2).
Mechanisms for secondary IFX treatment failure
The majority (70%) of patients with secondary IFX treatment failure had therapeutic serum IFX levels and undetectable IFX Abs at the time of therapeutic failure, suggesting a pharmacodynamic mechanism for the failure (see online supplementary figure). This subgroup of patients (per protocol) were in the algorithm group handled according to a review of the clinical condition by examinations for ongoing inflammatory disease activity, non-inflammatory complications, or other reasons for reported symptoms. As a result, these patients were treated for bile acid malabsorption (n=3), strictures (n=1) or irritable bowel syndrome (n=1) or were optimised on conventional agents (n=2 conventional immunosuppressives, n=2 with fistulising disease using antibiotics, n=2 oral hydrocortisone or budesonide, n=1 natalizumab, n=1 topical agents). Less commonly, failure was presumably due to immunogenicity of IFX, with IFX Abs and sub-therapeutic IFX levels (20%), or to non-immune-mediated pharmacokinetics, with sub-therapeutic IFX and undetectable IFX Abs (4%) (see online supplementary figure). Few patients had therapeutic IFX levels in the presence of IFX Abs (6%). There was no difference between randomisation groups with respect to classification (p=0.443).
Co-primary end points
Economic
As shown in table 2, costs related to treatment of Crohn's disease at the end of the trial at week 12 were significantly lower in the algorithm group than in the IFX intensification group in both the intention-to-treat population (mean difference per patient €−3141 (−4617; −1373), p<0.001) and the per-protocol population (€−5116 (−6482; −3561), p<0.001) (figure 3).
Primary and secondary end points at week 12

Co-primary economic end point in per protocol populations. Shown is average treatment per patient at end of trial at week 12, and at study visits at weeks 4 and 8. *p<0.001. IFX, infliximab.
Clinical
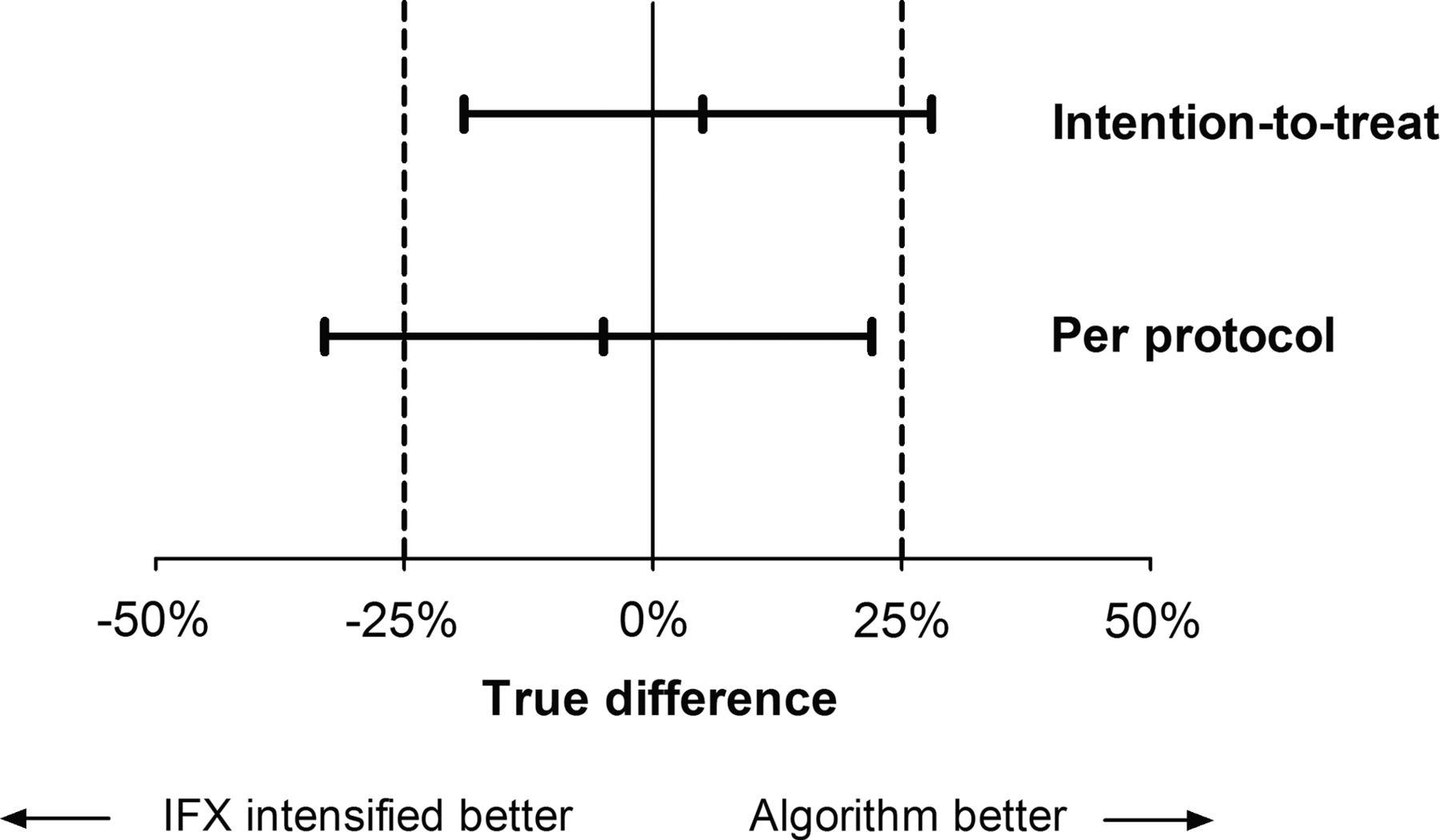
Response rates to study interventions at the end of the trial in the intention-to-treat population were 58% in the algorithm group and 53% in the IFX intensification group: relative risk (RR) 1.091 (0.713–1.673, 95% confidence interval), p=0.810. The difference between response rates was 5% (−19% to 28%) in favour of the algorithm group. This difference was within the predefined non-inferiority margin of −25% (table 2 and figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Co-primary clinical end point in intention-to-treat and per protocol populations. Shown is difference between response rates including 95% CIs among patients treated according to the algorithm presented in figure 1 compared with an intensified infliximab (IFX) regimen. Dashed lines illustrate the predefined non-inferiority margin.
In the per-protocol population, 47% in the algorithm group and 53% in the IFX intensification group showed a clinical response: RR 0.898 (0.510–1.580), p=0.781. The difference between response rates was −5% (−33% to 22%) (table 2 and figure 4).
Secondary end points
Secondary end points assessing clinical, life quality and biological responses were generally comparable between randomisation groups (table 2).
Subgroup analyses
Predefined subgroup analyses shown in the online supplementary table included assessment of co-primary end points in patients stratified for C-reactive protein (CRP) level at inclusion, disease phenotype and grouping in algorithm. Findings were similar to the above.
Exploratory analyses
Application of alternative IFX cut-off values for classification of drug levels as therapeutic or sub-therapeutic and measurement of IFX and IFX Abs by different types of assay based on ELISA and HMSA resulted in similar findings to the above (see online supplementary material).
Sensitivity analyses
Robustness of economic findings was assessed in independent sensitivity analyses of primary and secondary end points. The sensitivity analyses included (1) inclusion of estimated administrative costs for biological drugs, (2) use of actual IFX dosing and (3) price reductions of 3.5% and 7% on biological agents. All analyses revealed similar findings to the above.
Discussion
Loss of response to IFX maintenance therapy is currently handled by an empirical strategy of going through the available Crohn’s disease therapies including an intensified IFX regimen, change of TNF inhibitor, switching to a different biological drug class, and optimised use of conventional immunosuppressive drugs, glucocorticosteroids or surgery.3–5 It has been proposed that treatment of the individual patient may be optimised more cost-effectively by trying to determine the mechanism leading to treatment failure and then selecting interventions based on this knowledge. In this strategy, measuring levels of drug and drug Abs may assist clinical decisions.24
The present clinical trial is the first randomised, controlled testing of whether a personalised patient treatment based on IFX bioavailability and immunogenicity at the time of therapeutic failure (in order to identify the most likely mechanistic cause of loss of response) would guide rational clinical interventions and thus prove more cost-effective than standard IFX intensification.8 The main finding of our study is that interventions based on the algorithm achieved similar clinical, biological and life quality outcomes to dose intensification, but at a substantially, highly significantly, lower cost. Findings were also robust and consistent in subgroups stratified according to proposed mechanisms for therapeutic failure, disease phenotype and CRP levels, application of different types of assay, and changes in economic variables. A recent mathematical model analysis supports our findings.16
Our estimation of costs attributable to treatment of Crohn’s disease had high internal validity, as the Danish healthcare system provides a unique system that allows accurate determination of all health costs at an individual level. This is done on the basis of exact patient diagnosis, and the exact amount of each type of expense is uniformly defined by the Danish Health and Medicines Authority. Even though exact figures cannot be directly extrapolated to other countries, there is no reason to expect fundamentally different results in other healthcare settings, as expenses for intensified IFX are substantially higher than all other available interventions. Patients randomised to an intensified IFX regimen received infusions every 4 weeks to achieve maximal clinical efficacy. However, in everyday clinical practice, patients may alternatively receive infusions every 6 weeks, for example, and, in the case of a beneficial response to the intensified regimen, some patients may even later return to their original infusion regimen. These alternative strategies of dose intensification were not part of the study design and not reflected in the cost estimations.
The present algorithm operated with three distinct proposed mechanisms for secondary IFX failure: immunogenicity, non-immune-mediated pharmacokinetics and pharmacodynamics.8 Immunogenicity has been considered a common cause of IFX failure not only in Crohn’s disease but also in rheumatoid arthritis and other IFX-treated chronic inflammatory diseases.10 ,14 ,24 However, it was observed in only 20% of our patients. Non-immune-mediated sub-therapeutic IFX bioavailability due to individual variations in, for example, inflammatory load was rare.25 The vast majority had therapeutic IFX levels at failure, indicating a pharmacodynamic mechanism. It can be speculated that recurrence of disease activity in these patients arises from, for example, activation of alternative immunoinflammatory pathways bypassing TNF-α as one of the central mediators of Crohn's disease.24 ,26 However, for a notable fraction, there were non-inflammatory reasons for the erroneous reporting of secondary IFX failure, such as strictures, bile acid malabsorption and irritable bowel disease. On the basis of this observation, and in line with previously proposed treatment algorithms, it appears relevant to exclude non-inflammatory mechanisms for symptoms of relapse of Crohn's disease at an early stage of treatment optimisation.13 ,14 This study does not allow conclusions on how to optimally assess disease activity at reported IFX treatment failure.
While the concept of classifying IFX levels as therapeutic or sub-therapeutic to identify and distinguish mechanisms for secondary IFX treatment failures is intuitively attractive, the exact cut-off values are debatable and probably depend on the specific analytical method used. The cut-off values used in this study can be questioned as they originate from a single retrospective study.18 However, exploratory analyses using an alternative cut-off value resulted in reclassification of only a few patients, with unchanged study findings. Samples were obtained at manifest IFX failure, with timing corresponding to the next potential IFX administration (ie, trough level), and thus reflected conditions in vivo at the time of treatment failure, which is the relevant time point for defining individual treatment decisions. There are currently no defined gold standard assays for quantification of IFX and IFX Abs, and clinical investigations have thus far been carried out using a number of non-standardised, heterogeneous techniques.9 ,13 ,17 ,18 In order to extrapolate our findings, we also measured IFX and IFX Abs by a commercially available ELISA commonly used in North America and in pivotal clinical trials,9 ,13 and by a novel HMSA.19 Exploratory analyses revealed that, in this cohort, the previously mentioned assays resulted in similar classifications according to the proposed algorithm in the majority of patients (72–78%) and that the overall study results were not influenced by the type of analytical technique (see the online supplementary material). However, this study was designed to test the algorithm and not compare individual assays. A larger study directly comparing each assay is warranted to confirm these results.
The co-primary end point was attained in the intention-to-treat population, as the 95% CI around the point estimate of the treatment difference was within the prespecified non-inferiority margin. Although the per-protocol analysis yielded numerically similar results to the intention-to-treat analysis (ie, point estimates of treatment difference close to 0, figure 4), the 95% CI in this analysis was wider and included the prespecified non-inferiority margin. This was probably because a number of patients were not treated completely according to the algorithm and thus had to be excluded from the per-protocol analysis, making the number of subjects too small to provide a sufficiently narrow CI. Thus formal non-inferiority could not be declared in this analysis. Furthermore, when interpreting the results, it should be noted that a fairly wide non-inferiority margin corresponding to half the mean estimated response rate (δ=0.25) was applied in order to reach a feasible sample size. However, as pointed out previously, the point estimates of the difference between treatments were very close to 0 and, furthermore, all secondary clinical end points were also similar between randomisation groups. Thus, in spite of the previously mentioned limitations, the present efficacy data indicate that the algorithm-based approach does not result in substantially inferior efficacy compared with dose intensification.
In conclusion, managing secondary IFX treatment failure by an algorithm based on serum IFX and IFX Abs to define the mechanistic basis and corresponding interventions is more cost-effective than an intensified IFX regimen. The basis for this difference is the lower costs attained by avoiding inappropriate use of drugs—without apparent negative consequences for clinical efficacy.
Acknowledgments
The authors would like to thank Biomonitor A/S (Copenhagen, Denmark) and Prometheus Laboratories (San Diego, California, USA). Further, thanks for technical assistance go to: Hanne Fuglsang, Anne Hallander, Vibeke Hansen, Birgit Kristensen, Yvonne Krogager, Charlotte Kühnel, Lene Neergaard, Lise Olsen and Anni Petersen (Department of Gastroenterology, Herlev University Hospital, Denmark); Pierre Nourdine Bouchelouche and Sussi Holbæk (Department of Medical Gastroenterology, Køge University Hospital, Denmark); Tove Nygaard (Department of Medical Gastroenterology, Aalborg University Hospital, Denmark); Rikke Charlotte Andersen, Lisbet Gerdes, Catriona Nairn Marcussen, Birgitte Sperling Wilms Nielsen and Inger Schjødt (Department of Hepatology and Gastroenterology V, Aarhus University Hospital), Carina Blixt (Department of Gastroenterology, Hvidovre University Hospital, Denmark); Anne Berg (Department of Medical Gastroenterology S, Odense University Hospital, Denmark).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors Study design and interpretation of data: CS, MAA, OØT, JB. Collection of data: all authors. Analysis of data: CS, MAA, ASO, JK. Drafting the manuscript: CS. Revising the manuscript and approval of final manuscript: all authors.
-
Funding Support for this study was provided by unrestricted grants from Aase and Ejnar Danielsen's Foundation, Beckett Foundation, Danish Biotechnology Program, Danish Colitis-Crohn Society, Danish Medical Association Research Foundation, Frode V Nyegaard and Wife's Foundation, Health Science Research Foundation of Region of Copenhagen, Herlev Hospital Research Council, Lundbeck Foundation, P Carl Petersen's Foundation, Ole Østergaard Thomsen’s Research Foundation and Jørn Brynskov’s Research Foundation.
-
Competing interests CS has served as speaker for MSD and Abbvie and as a consultant for MSD and Takeda Pharmaceutical Company. JB has served as advisory board member for Abbvie. OØT has served as a speaker and consultant for UCB and Zealand Pharma, speaker for MSA, and primary investigator for Amgen, Biogen, Novo-Nordisk and Pfizer. LKM has served as a speaker for MSD and participated in a safety study with Abbvie. JF has served as primary investigator for Centocor, Abbvie, MSD and UCB and as a consultant for Abbvie and MSD. LAC has served as a speaker for Abbvie, Tillotts Pharma and Ferring, and as a consultant for MSD. JK has served as a speaker for MSD, Abbvie and Tillotts. KB has served as a speaker for Pfizer, Roche, Novo-Nordisk, Bristol-Meyers Squibb and Biomonitor and owns stocks in Novo-Nordisk and Biomonitor. BAJ has served as an advisory board member at Tillots Pharma.
-
Ethics approval Danish Medicines Agency (EudraCT 2009-009926-94), the regional ethics committees (HA-2009-009) and the Danish Data Protection Agency (2007-58-0015; 750.89-2).
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.