Article Text

Abstract
BACKGROUND In a retrospective study bile acid malabsorption was observed in patients with collagenous colitis.
AIMS To study the occurrence of bile acid malabsorption and the effect of bile acid binders prospectively in patients with chronic diarrhoea and collagenous colitis.
METHODS Over 36 months all patients referred because of chronic diarrhoea completed a diagnostic programme, including gastroscopy with duodenal biopsy, colonoscopy with biopsies, and the 75Se-homocholic acid taurine (75SeHCAT) test for bile acid malabsorption. Treatment with a bile acid binder (cholestyramine in 24, colestipol in three) was given, irrespective of the results of the 75SeHCAT test.
RESULTS Collagenous colitis was found in 28 patients (six men, 22 women), 27 of whom had persistent symptoms and completed the programme. Four patients had had a previous cholecystectomy or a distal gastric resection. The 75SeHCAT test was abnormal in 12/27 (44%) of the collagenous colitis patients with 75SeHCAT values 0.5–9.7%, and normal in 15 patients (56%). Bile acid binding treatment was followed by a rapid, marked, or complete improvement in 21/27 (78%) of the collagenous colitis patients. Rapid improvement occurred in 11/12 (92%) of the patients with bile acid malabsorption compared with 10/15 (67%) of the patients with normal 75SeHCAT tests.
CONCLUSION Bile acid malabsorption is common in patients with collagenous colitis and is probably an important pathophysiological factor. Because of a high response rate without serious side effects, bile acid binding treatment should be considered for collagenous colitis, particularly patients with bile acid malabsorption.
- bile acid malabsorption
- collagenous colitis
- diarrhoea
- cholestyramine
- colestipol
Statistics from Altmetric.com
Chronic diarrhoea is a disabling symptom and represents a considerable diagnostic challenge. Two possible diagnoses which should be considered for every patient with chronic watery diarrhoea are collagenous colitis1-3 and bile acid malabsorption.4 The aetiopathogenesis of collagenous colitis is unknown. There is an over representation of autoimmune disorders in this condition.3 5-17 Furthermore, a luminal factor has been proposed as a possible aetiological agent.18 Despite the similarity in symptoms between bile acid malabsorption and collagenous colitis, few attempts have been made to study a possible relation between the two conditions. In a previous study, it was concluded that there is no evidence of bile acid malabsorption in patients with collagenous colitis.19However, according to the 75Se-homocholic acid taurine (75SeHCAT) test used, one of the eight patients in that study had apparent bile acid malabsorption, and another patient had a borderline value. A few patients have been reported to respond favourably to the bile acid binding agent cholestyramine.3 20 In one extensively investigated patient with collagenous colitis the symptoms and even the histological changes disappeared with cholestyramine treatment.20 There was no direct or indirect evidence of bile acid malabsorption in this patient.
In a small retrospective study of 10 patients with collagenous colitis we found the 75SeHCAT test to be abnormal in five patients, who subsequently responded to treatment with cholestyramine.21 These observations have prompted this further study of the role of bile acids in collagenous colitis.
The primary aim of the present study was to investigate prospectively the occurrence of bile acid malabsorption in patients with collagenous colitis. Secondly, we wished to elucidate the potential value of treatment with bile acid binding agents and to see whether the clinical effect was linked to the presence of bile acid malabsorption.
Methods
Over a period of 36 months all patients (n=404) referred to our Gastroenterology Unit because of severe chronic diarrhoea without blood and with negative faecal culture for bacteria, completed a diagnostic programme which included gastroscopy with duodenal biopsy, colonoscopy with biopsy, and the 75SeHCAT test for bile acid malabsorption.22 Some of the patients included had been referred to our hospital because of persistent symptoms and a previous, incomplete diagnostic evaluation. In total 28 patients with collagenous colitis were registered during the three year period. Twenty seven of the patients had persistent severe diarrhoea. In one male patient the symptoms decreased spontaneously after the colonoscopy; this patient declined the 75SeHCAT test and further treatment.
During colonoscopy, biopsy specimens were obtained from the left colon in all patients, from the proximal colon in 22 patients, and from the distal ileum in nine patients. Conventional criteria for collagenous colitis were typical microscopic inflammation including an increased number of intraepithelial lymphocytes, and a subepithelial collagen layer of at least 10 μm.1 2 23 Gastroscopy was performed on all patients and a duodenal biopsy sample was taken for histological evaluation, including a coeliac disease test. In two of three patients with a history of coeliac disease, normalisation of the duodenal mucosa with a gluten free diet had been shown before this study.
75SeHCAT TEST
The procedure for measuring 75SeHCAT retention followed the technique described by Thaysen et al.22 A capsule containing 0.3 MBq75SeHCAT was swallowed. Measurements were performed with an uncollimated gamma camera with the patients in a supine position and the gamma camera positioned at a distance of 60 cm. The initial measurement (value for 100%) was performed three hours after ingestion of the capsule. Retention was then measured after four and seven days. A retention value of less than 10% on day 7 was considered abnormal.24 25 Medication that could have a potential effect on bile acid absorption was stopped before the test.
TEST FOR BACTERIAL OVERGROWTH OF THE SMALL BOWEL
The initial 20 patients were tested for bacterial overgrowth, either with the hydrogen breath test after ingestion of 50 g glucose in 250 ml water (19 patients) or direct culture on duodenal aspirate (one patient). In one patient with a positive breath test, bacterial overgrowth was confirmed by direct culture on a duodenal aspirate. The criteria for positive tests were an increase in the hydrogen concentration of more than 14 ppm over the baseline values26 and a culture containing more than 105 colonic type bacteria/ml,27 respectively.
STOOL FREQUENCY
The stool frequency was recorded daily and the registration time corresponded to the seven days when the 75SeHCAT test was performed. Data were available for 24 patients.
TREATMENT
All symptomatic patients (n=27) had a therapeutic challenge with an open label bile acid binder. Twenty four patients were prescribed cholestyramine (Questran, Bristol-Myers Squibb) in dose packets of 4 g. In the case of three patients who reported considerable problems with the smell and the taste of drugs, colestipol (Lestid, Upjohn) was given instead, in dose packets of 5 g. The patients were informed that there is no generally accepted “drug of choice” for collagenous colitis although bile acid binders have been reported to be effective in some patients with this disorder. The patients were instructed to start treatment with one packet two or three times daily. If the effect on diarrhoea was insufficient, they were instructed to increase the dose, if possible up to six packets a day. If constipation occurred, the patients were instructed to decrease the dose. The effect on diarrhoea was evaluated two months after the start of treatment. Rapid improvement was defined as a positive response, with no more than two stools/day, within one week after reaching the optimal dose, and the patients reporting a persistent marked improvement or complete recovery in the diarrhoeal symptoms at the two month control. A few patients had a slow gradual improvement, taking more than two weeks for a clear cut effect but remaining improved at the two month control point. These patients were not classified as rapid responders, although they preferred not to discontinue the bile acid binder treatment.
If bile acid binder treatment failed, we initiated an optional strategy, based partly on previous reports from small studies and partly on the possible risks of long term treatment: instead of the bile acid binder, sulphasalazine (Salazopyrin, Pharmacia) 1 g twice daily was prescribed for two months. If this therapy failed, metronidazole 0.4 g was given three times daily for two weeks followed by 0.4 g twice daily for six months. The final therapeutic option of oral steroids was not necessary as all patients had already responded to one of the previous treatments.
STATISTICAL ANALYSIS
The results for stool frequency are presented as medians, interquartile range, and 10th and 90th percentiles. A comparison between groups with and without bile acid malabsorption was performed using the Mann-Whitney U test for unpaired data.
Results
BILE ACID ABSORPTION
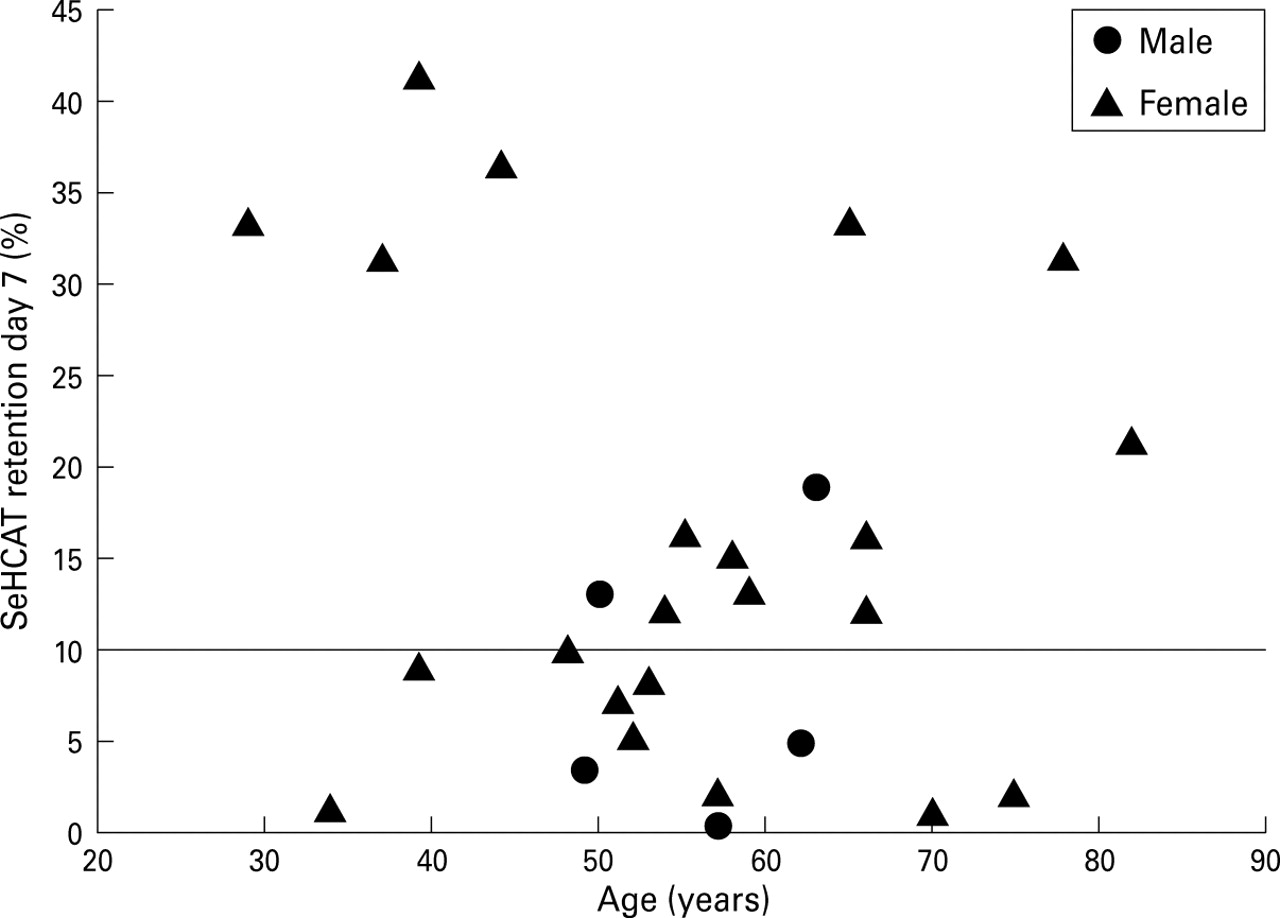
Bile acid malabsorption, defined as a 75SeHCAT retention less than 10% on day 7, occurred in 12 of 27 (44%) patients with collagenous colitis. Figure 1 shows the results of the75SeHCAT test in relation to age and sex. The occurrence of bile acid malabsorption was not significantly related to age or sex.

75SeHCAT retention on day 7 in 27 patients with collagenous colitis.
STOOL FREQUENCY
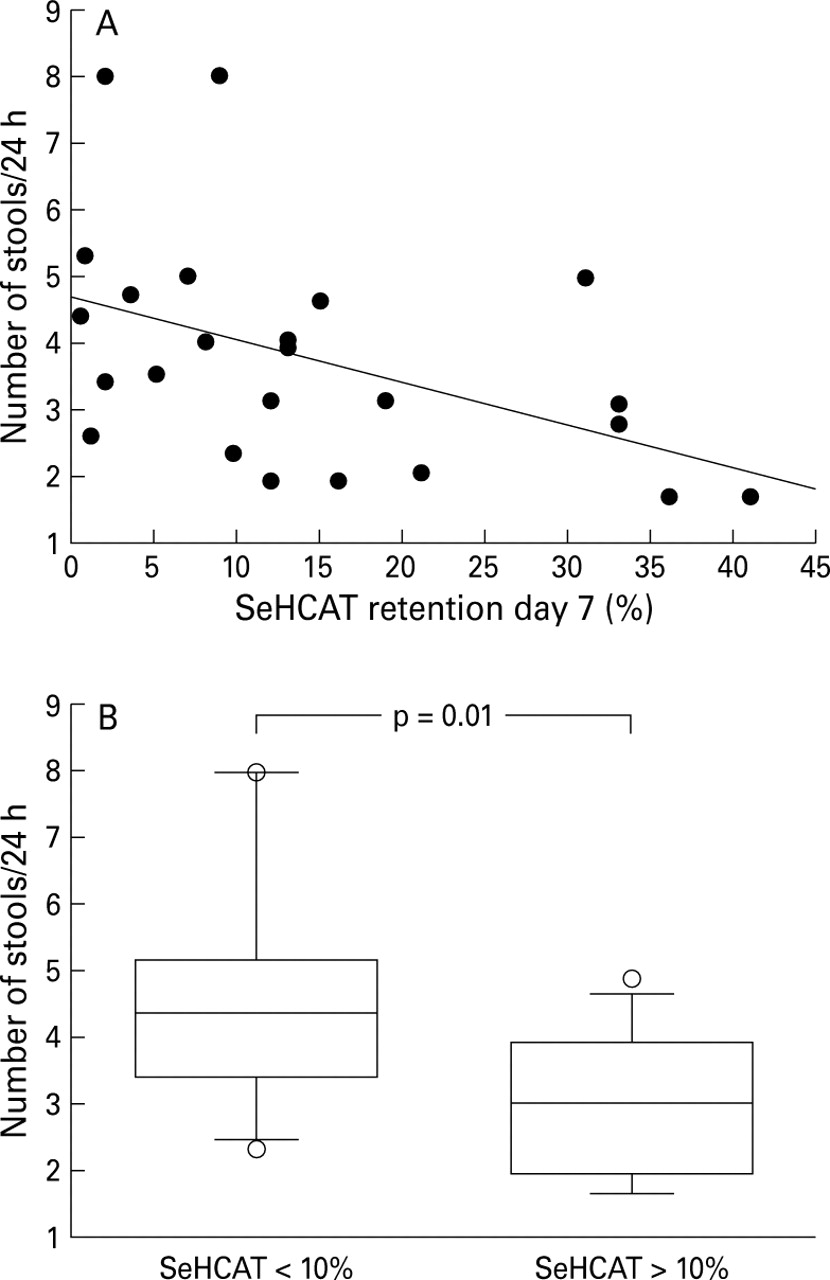
Figure 2A shows the mean number of stools per day for individual patients during the week of symptom registration. There was a significant negative correlation between the mean number of stools and the 75SeHCAT retention on day 7 (p=0.02). Figure 2B shows that stool frequency was significantly higher in patients with collagenous colitis and bile acid malabsorption than in those without bile acid malabsorption.

Relation between stool frequency and bile acid malabsorption in patients with collagenous colitis. (A) The mean individual number of stools was negatively correlated to the75SeHCAT retention on day 7 (p=0.02). (B) Box plot of stool frequency in patients with and without bile acid malabsorption.
DURATION OF SYMPTOMS
Patients with bile acid malabsorption had a significantly longer history of diarrhoea than patients without bile acid malabsorption (median 8 years, range 0.5–30 years, n=12 versus median 2 years, range 0.5–15 years, n=15; p<0.05). There was no significant relation between the duration of symptoms and the age of the patients.
ASSOCIATED DISEASES
Table 1 presents the occurrence of autoimmune diseases and previous abdominal surgery. Eleven patients (41%) had at least one associated autoimmune disease. Four patients had had one or two abdominal operations, including three patients with cholecystectomy, all showing bile acid malabsorption. Fourteen patients (52%) had no history of autoimmune disease or a history of abdominal surgery. There was no statistical correlation between autoimmune disease and the occurrence of bile acid malabsorption or between autoimmune disease and sex.
Number of patients with associated conditions, and the individual 75SeHCAT values in 27 patients with collagenous colitis
EFFECT OF TREATMENT WITH BILE ACID BINDERS
Treatment with a bile acid binder was given to all symptomatic patients (cholestyramine to 24 patients, colestipol to three patients) with collagenous colitis. A rapid improvement with a clear cut decrease in diarrhoea within one week was noted in 21 of the 27 patients (“rapid responders” to bile acid binders). Six patients did not show this rapid response. Eleven of 12 patients with bile acid malabsorption (92%) showed a rapid response, while in patients with a normal 75SeHCAT test this response rate was 67%. Another two patients, including the non-responding patient with bile acid malabsorption, improved slowly over a period of one to two months. All the non-responders were women over 50 years old. However, there was no statistically significant relation between sex or age and the outcome of treatment with bile acid binders.
The daily dose of bile acid binder needed to control diarrhoeal symptoms ranged from 0.5 to 6 (median: 2.5) packets daily (cholestyramine 4 g or colestipol 5 g per packet). The highest dose needed was cholestyramine 24 g daily, in one particular patient. This dose could later be reduced to 16 g daily. All three patients treated with colestipol, one with and two without bile acid malabsorption, responded rapidly to treatment.
OUTCOME OF TREATMENT STRATEGY
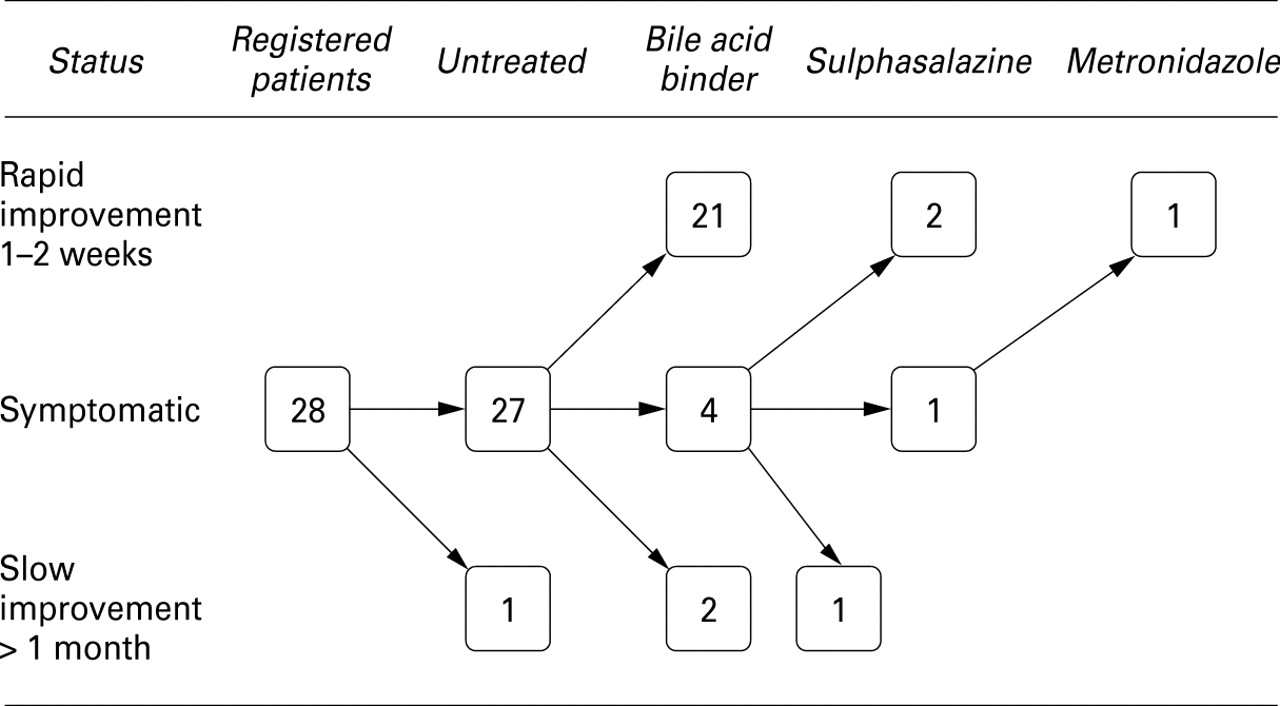
Figure 3 illustrates the outcome of treatment of the 27 symptomatic patients with collagenous colitis. Twenty three of the symptomatic patients improved rapidly or slowly when treated with a bile acid binder alone. Three of the remaining four patients, with no improvement or only a slight improvement with a bile acid binder, responded to either sulphasalazine alone (two patients) or an inadvertent combination of cholestyramine and sulphasalazine (one patient). The remaining symptomatic patient responded to metronidazole within two weeks and remained asymptomatic during the long term treatment period of six months with metronidazole 0.8 g per day.

{kind=link}
{kind=link}
{kind=link}
Resolution of diarrhoea in 28 patients with collagenous colitis.
As all patients with collagenous colitis had sufficient control of the diarrhoea before the fourth optional treatment, steroids were not used in this study.
COLLAGEN LAYER
Ten of the patients with collagenous colitis had a collagen layer thicker than 20 μm. The remaining patients had a collagen layer thickness in the range 10–20 μm. There was no statistical difference in the 75SeHCAT test between the patients with a thick layer (median 75SeHCAT value 11%) and those with a layer 10–20 μm (median 75SeHCAT value 11%).
Eight of the nine patients who had ileal biopsies performed had normal histology. Three of these had low 75SeHCAT values. One patient with coeliac disease had atrophy of the ileal and the duodenal mucosa but had a normal 75SeHCAT value of 13%. All of the remaining patients had a normal duodenal histopathology. Consequently, none had collagenous changes of the duodenal or the ileal mucosa.
TEST FOR BACTERIAL OVERGROWTH OF THE SMALL BOWEL
Nineteen patients had a hydrogen breath test and one patient had a culture from duodenal aspirate to test for bacterial overgrowth. Nine of these patients had bile acid malabsorption and 11 patients had normal 75SeHCAT values. The bacterial culture on the duodenal aspirate was negative and the breath test showed increased hydrogen values compatible with bacterial overgrowth in only one of the patients tested. In this particular patient, bacterial overgrowth was confirmed by a positive bacterial culture on duodenal aspirate. This patient had a history of cholecystectomy and Billroth I gastric resection due to peptic ulcer disease. As 19 of the first 20 patients tested were negative, and the patient with bacterial overgrowth had a strong predisposing factor, the remaining seven patients were not tested for bacterial overgrowth.
Discussion
In this prospective study on the potential role of bile acids in collagenous colitis we found using the 75SeHCAT method that bile acid malabsorption occurred in a considerable proportion (44%) of the patients. This is in accordance with a few earlier observations in small studies, including our own initial report on the effect of cholestyramine on patients with collagenous colitis.3 20 21 As in the previous series of patients with collagenous colitis, our patient group was female dominated and there was a high prevalence of autoimmune diseases, comparable to previous reports.3 5-17 However, the occurrence of bile acid malabsorption in our collagenous colitis patients showed no statistical association with sex, presence of autoimmune disease, or age. The association between bile acid malabsorption and cholecystectomy or gastric resection has been described previously,22 28 although the present study shows that collagenous colitis might also contribute to diarrhoea in these patients.
The simultaneous occurrence of bile acid malabsorption in patients with collagenous colitis may influence the clinical presentation of the patients. Despite similar histological findings, including the thickness of the collagen layer and similarities in other parameters between patients with and without bile acid malabsorption, patients with bile acid malabsorption had more symptoms, manifested as significantly higher stool frequency.
The patients with collagenous colitis and concomitant bile acid malabsorption had a significantly longer history of diarrhoea than patients without bile acid malabsorption. The reason for this is not obvious from the present data.
The aetiopathogenesis of bile acid malabsorption and collagenous colitis is in many aspects still obscure. The high occurrence of autoimmune disorders in the present and previous reports suggests a genetic predisposition to collagenous colitis.3 5-17 The occurrence of small bowel bacteria or toxins of bacterial origin has also been suggested.14 20 However, we found no obvious relation between small bowel bacterial overgrowth and collagenous colitis. Only one of 20 patients tested for bacterial overgrowth in this study showed small bowel bacterial overgrowth. This particular patient, apart from a previous cholecystectomy, had also had a previous Billroth I operation predisposing for bacterial overgrowth.29 She responded to continuous cholestyramine treatment. This patient had a few later relapses of diarrhoea during cholestyramine treatment. These relapses ceased when treatment for intestinal bacteria with norfloxacin was given for periods of one to two weeks, during which she still had to maintain the ordinary dose of cholestyramine to control the diarrhoea. In this interesting case, the diarrhoea promoting factors bacterial overgrowth and bile acid malabsorption were apparently independent of each other.
Ileal biopsy specimens were available from nine patients, three of whom had bile acid malabsorption. However, ileal histology and duodenal histology were normal except in one patient, who had coeliac disease and atrophy of the ileal and the duodenal mucosa but a normal75SeHCAT value. As in previous series of patients with microscopic colitis,3 8 9 there was also an increased proportion of coeliac disease in our study. None of the patients showed signs of collagenous duodenitis or collagenous ileitis, conditions that have been previously described in a few case reports.30-33 In the present study, small bowel factors as shown by tests of bacterial overgrowth and by the histology of duodenal and ileal mucosa, could not explain the occurrence of collagenous colitis and the associated bile acid malabsorption.
The main pathophysiological mechanism for the occurrence of diarrhoea in collagenous colitis is suggested to be reduced permeability for electrolytes and water in the colonic mucosa,1 14 34while the active absorption of bile acids occurs in the terminal ileum.35 Other diarrhoeal disorders of colonic origin have not been shown to cause abnormal 75SeHCAT values.36 37 Diarrhoea per se might reduce the75SeHCAT value but not to an abnormal level.25 38 39 This suggests that the low75SeHCAT values found in the present study correspond to a reduced capacity to absorb bile acids in the ileum and are not due to a colonic malabsorption secondary to the diarrhoea caused by collagenous colitis.
The present prospective study tested whether the clinical response of patients with collagenous colitis to treatment with an open label bile acid binder is related to simultaneous bile acid malabsorption—that is, whether the result of the 75SeHCAT test could predict the outcome of treatment. All patients with bile acid malabsorption, defined as a low value with the 75SeHCAT test, responded to bile acid binders. Eleven of 12 patients showed a rapid response. The twelfth patient showed a slower but positive response, which could be a drug effect or it could represent the natural course of the disease similar to the spontaneously improved patient.
There was no statistically significant difference in the response rate in patients with and without bile acid malabsorption. This was due to the relatively high response rate (67%) in non-bile acid malabsorption patients. The results suggest that in patients with collagenous colitis and bile acid malabsorption, treatment of the observed bile acid malabsorption was sufficient to obtain a clinical response and none of the drugs used for inflammatory bowel disease was needed. It seems less likely that the rapid response, often within a few days, could correspond to a normalisation of the colonic mucosa. However, no detailed information is as yet available regarding the regression of histological inflammation during bile acid binder treatment although this issue is now under investigation (Ung et al, to be published).
The high response rate to the bile acid binders, even in patients with a normal 75SeHCAT test value, suggests that cholestyramine and colestipol may also have clinical effects on collagenous colitis through mechanisms other than pure bile acid binding. This would be in agreement with a previous case report, where the patient with collagenous colitis responded to cholestyramine. However, direct tests of bile acid malabsorption were not performed in that patient. The mechanisms of cholestyramine were suggested to be binding of toxins and other effects on the intraluminal contents.20Alternatively, the colonic inflammation may be the result of an abnormal reaction to normal amounts of bile acids entering the colon. In this context, it is of interest that in none of our patients could the collagenous colitis related diarrhoea be linked to small bowel bacterial overgrowth.
Hitherto, there has been no generally accepted drug of choice for the treatment of patients with collagenous colitis. In the present study we had a treatment strategy with additional options based on the previously reported effects of sulphasalazine, antibiotics, and steroids. The risk of long term treatment with metronidazole, particularly neuropathy, prompted us to choose sulphasalazine as the second line drug and metronidazole as the third option, should bile acid binders fail. Remarkably, all 27 patients responded to one of the first three choices and steroids, the fourth option, were not prescribed. Further studies are needed to evaluate the histological improvement during the course of the various types of treatment. As steroids do not heal the inflammatory changes in the colonic mucosa in patients with collagenous colitis,40 the strategy of using a bile acid binder as the first line treatment with 5-acetylsalicylic acid/sulphasalazine and antibiotics as alternative drugs, seems attractive. Apart from the taste problem and for some patients the smell, as well as the potential need for vitamin supplements, side effects from bile acid binders are rare.
In patients with collagenous colitis without bile acid malabsorption, bile acid binders may also be the first option. However, apart from bile acid binders, bismuth subsalicylate has recently been reported to have a good clinical effect on patients with microscopic colitis.41 42 In one patient with microscopic colitis, a normal 75SeHCAT value, and disabling diarrhoea, refractory to six different drugs including cholestyramine, the response to bismuth subsalicylate was excellent.42 Further placebo controlled studies should take various aetiopathogenic factors into consideration and evaluate the effect of bile acid binders, bismuth, and other drugs of potential interest.
In conclusion, the present study shows that a considerable proportion of patients with collagenous colitis have bile acid malabsorption and that in these patients bile acid binders seem to be the first line treatment. Moreover, in collagenous colitis patients without bile acid malabsorption, two thirds responded to a bile acid binder (cholestyramine or colestipol). The results show that bile acids may be an important aetiopathogenic factor, although not the only factor, in patients with collagenous colitis.
Acknowledgments
This study was supported by the Swedish Medical Research Council (grant 8288) and by the Faculty of Medicine, University of Göteborg. This work was presented in part at the 1997 meeting of the American Gastroenterological Association and published in abstract form (Gastroenterology1997;112:A1108).
References
Footnotes
- Abbreviation used in this paper:
- SeHCAT
- Se labelled homocholic acid taurine