
Abstract
Background
Endoscopic ultrasonography (EUS) is considered valuable for preoperative staging of gastric cancer and defining patient eligibility for enrollment in neoadjuvant protocols. The aim of this study was to correlate EUS staging with pathologic evaluation and outcome in patients undergoing curative R0 resection for gastric cancer.
Methods
All patients who underwent preoperative clinical assessment of T/N stage with EUS and subsequent R0 resection for gastric adenocarcinoma between 1993 and 2003 were identified from a prospective database. Patients who received neoadjuvant chemotherapy were excluded. Clinical staging results from preoperative EUS were compared with postoperative pathologic staging results and correlated with clinical outcome.
Results
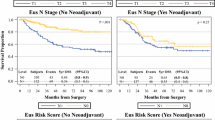
Two hundred twenty-five patients with gastric cancer underwent EUS followed by R0 resection, without preoperative chemotherapy. The accuracy of the individual EUS T stage was 57% (127 of 223) and was 50% for N stage (110 of 218). Although EUS was less able to predict outcome according to individual T stage, patients with lesions ≤T2 on EUS had a significantly better outcome than patients with lesions ≥T3. Preoperative assessment of risk was not predicted by EUS N stage alone. Patients identified as high risk on EUS and those with a combination of serosal invasion and nodal disease had both the highest concordance with pathology and a significantly worse outcome (P = .02).
Conclusions
The concordance between EUS and pathologic results was lower than expected for individual T and N stages. Patients with lesions ≤T2 had a significantly better prognosis than patients with more advanced lesions. Individual EUS N stage has limited value in preoperative risk assessment. Combined assessment of serosal invasion and nodal positivity on EUS identifies 77% of patients at risk for death from gastric cancer after curative resection.





Similar content being viewed by others


References
Cancer Facts and Figures 2006. Available at: http://www.cancer.org/docroot/stt/stt_0.asp, accessed on 5 September 2006
Brennan MF. Benefit of aggressive multimodality treatment for gastric cancer. Ann Surg Oncol 1995;2:286–7
Martin RC II, Jaques DP, Brennan MF, Karpeh M. Achieving R0 resection for locally advanced gastric cancer: is it worth the risk of multiorgan resection? J Am Coll Surg 2002; 194:568–77
Hochwald SN, Kim S, Klimstra DS, et al. Analysis of 154 actual five-year survivors of gastric cancer. J Gastrointest Surg 2000; 4:520–5
Macdonald JS, Smalley SR, Benedetti J, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 2001; 345:725–30
Cunningham D, Allum W, Stenning S, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. New Engl J 2006; 355:11–20
Botet JF, Lightdale CJ, Zauber AG, et al. Preoperative staging of gastric cancer: comparison of endoscopic US and dynamic CT. Radiology 1991; 181:426–32
Tio TL, Kallimanis GE. Endoscopic ultrasonography of perigastrointestinal lymph nodes. Endoscopy 1994; 26:776–9
Smith JW, Brennan MF, Botet JF, et al. Preoperative endoscopic ultrasound can predict the risk of recurrence after operation for gastric carcinoma. J Clin Oncol 1993; 11:2380–5
Miller FH, Kochman ML, Talamonti MS, et al. Gastric cancer. Radiologic staging. Radiol Clin North Am 1997; 35:331–49
Lowy AM, Feig BW, Janjan N, et al. A pilot study of preoperative chemoradiotherapy for resectable gastric cancer. Ann Surg Oncol 2001; 8:519–24
Ajani JA, Mansfield PF, Janjan N, et al. Multi-institutional trial of preoperative chemoradiotherapy in patients with potentially resectable gastric carcinoma. J Clin Oncol 2004; 22:2774–80
Shah MA. Recent developments in the treatment of gastric carcinoma. Curr Oncol Rep 2002; 4:193–201
Rosch T. Endosonographic staging of gastric cancer: a review of literature results. Gastrointest Endosc Clin North Am 1995; 5:549–57
Bando E, Kawamura T, Kinoshita K, et al. Magnitude of serosal changes predicts peritoneal recurrence of gastric cancer. J Am Coll Surg 2003; 197:212–22
Acknowledgments
The authors thank Marianne Beninati for her help with data collection. Supported by a grant from the Gelb Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bentrem, D., Gerdes, H., Tang, L. et al. Clinical Correlation of Endoscopic Ultrasonography with Pathologic Stage and Outcome in Patients Undergoing Curative Resection for Gastric Cancer. Ann Surg Oncol 14, 1853–1859 (2007). https://doi.org/10.1245/s10434-006-9037-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-006-9037-5