Article Text

Abstract
Background Sofosbuvir plus ribavirin (SOF+RBV) for 12 weeks is the standard treatment for chronic hepatitis C (CHC) genotype 2 (GT2) in most of Asia despite availability of new CHC medications. SOF-RBV real-world effectiveness has only been reported in small and/or single-centre studies. Our goal was to determine the real-world effectiveness of 12-week SOF+RBV therapy for CHC GT2 in Asia.
Methods A systematic search on PubMed and Embase was conducted through 30 June 2017. We identified full articles and conference proceedings of at least 10 adult patients with CHC GT2 treated with SOF+RBV for 12 weeks under real-world setting in Asia.
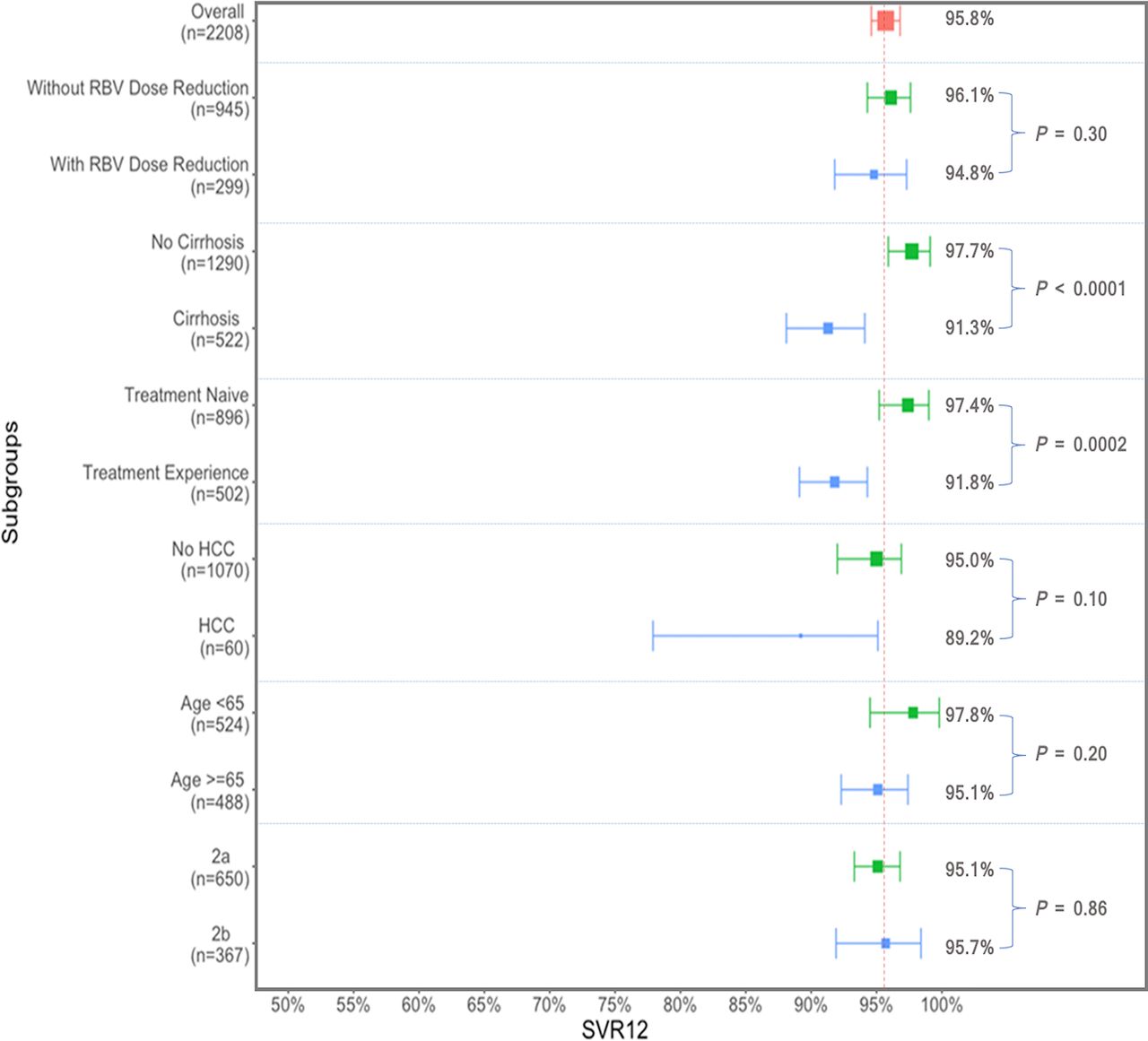
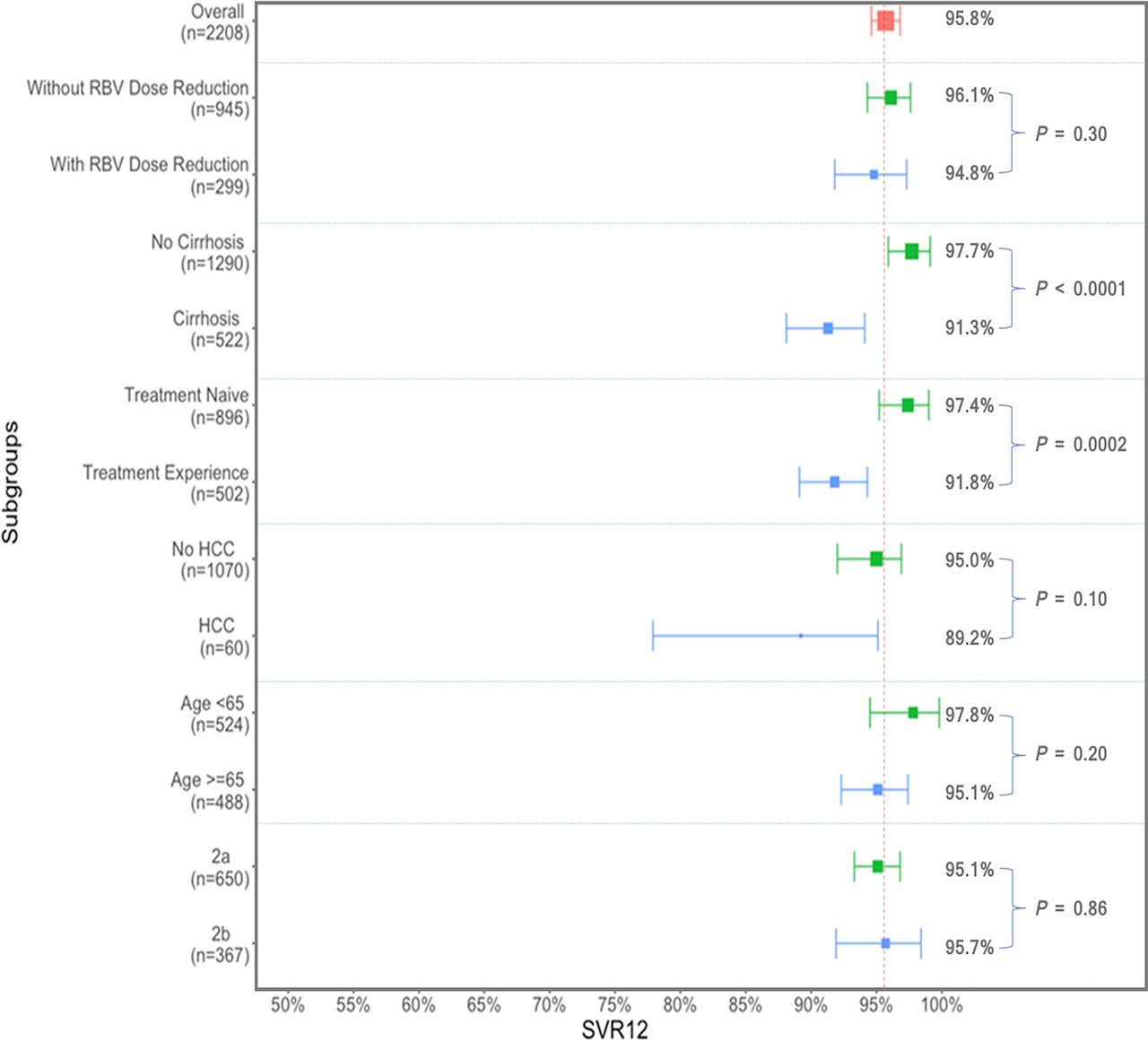
Results A total of 2208 patients from 13 studies were included. The pooled sustained virological response 12 weeks after the end of treatment (SVR12) was 95.8% (95% CI 94.6% to 96.9%) with non-significant heterogeneity (I2=34.4%). Anaemia (27.9%) was the most common adverse event (AE), with serious AEs in 2.0% and only 0.7% discontinued therapy prematurely. In subgroup analyses, patients with cirrhosis had 8.7% lower SVR12 than non-cirrhotic patients (P<0.0001), and treatment-experienced patients had 7.2% lower SVR12 than treatment-naïve patients (P=0.0002). Cirrhotic treatment-experienced patients had the lowest SVR12 at 84.5%. There were no significant differences in pooled SVR12 among patient subgroups: RBV dose reduction versus no dose reduction (P=0.30); hepatocellular carcinoma (HCC) versus no HCC (P=0.10); GT 2a versus 2b (P=0.86); and <65 vs ≥65 years of age (P=0.20).
Conclusions SOF+RBV for 12 weeks was safe and effective for patients with CHC GT2 in Asia, although those with cirrhosis and prior treatment failure had a lower pooled SVR12 rate.
Trial registration number CRD42017067928.
- hepatitis C
- liver cirrhosis
- genotype
- adverse drug reactions
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Chronic infection with hepatitis C virus (HCV) is one of the major health burdens in the world affecting 71.1 million persons and causing 700 000 deaths per year.1 Of all the cases of chronic hepatitis C (CHC) in the world, two-thirds are from Asia, which has an overall HCV prevalence ranging from 0.1% to 4.7%.2 HCV genotype 2 (GT2) is the second most common genotype in many parts of Asia, especially in East Asia.3
From 2001 to 2011, pegylated interferon (Peg-IFN) plus ribavirin (RBV) for 24 weeks was the standard combination therapy for GT2.4 While HCV GT2 was considered the easiest-to-treat HCV genotype with this regimen, sustained virological response (SVR) rate was only 70%–80%. Peg-IFN-based therapy was also contraindicated in many patients due to its adverse event (AE) and serious adverse event (SAE) profiles.5
Sofosbuvir (SOF) is an oral direct-acting pan-genotypic HCV nucleotide polymerase inhibitor approved in the USA in 2013 and in Asia shortly thereafter.6 7 The new IFN-free regimen SOF plus RBV (SOF+RBV) for 12 weeks then became a recommended all-oral combination therapy for patients with HCV GT2 in Asia in 2014 until new regimens became available in selected parts of Asia very recently.8 9 SVR at 12 weeks after the end of the treatment (SVR12) instead of 24 weeks was used as the new standard for assessment of virological cure, especially as the overall SVR12 rate increased from 78% to 97%, provided a better side-effect profile (a decrease in AEs from 11% to 1%), a reduced discontinuation rate, and an allowance for many non-IFN candidates to be treated.4 10 11
However, clinical trial data in both the USA and Asia have shown that the SVR was higher in patients without cirrhosis (97%) than those with cirrhosis (91%), and in treatment-naïve (97%) than in treatment-experienced patients (88%–91%).4 12 In real-world studies where patients were not as highly selected and were more likely to have advanced liver disease and/or other comorbidities, lower SVR12 rates have been reported in Western population.13–15
Although newer direct-acting antiviral (DAA) regimens have recently become available in the USA and Europe and even parts of Asia, low-cost generic SOF+RBV may still be more accessible for patients in resource-constrained regions, such as most of Asia.16 17 Therefore, our goal was to perform a systematic review and meta-analyses with meta-regression to determine the real-world effectiveness of SOF+RBV at 12 weeks for patients with HCV GT2 in Asia.
Methods
Data sources and search strategy
We conducted a systematic search on PubMed and Embase for full article publications from inception through 30 June 2017. Abstracts from the recent 3 years (2015, 2016 and/or 2017) for major international conferences in gastroenterology and hepatology, including the American Association for the Study of Liver Diseases, the European Association for the Study of the Liver, Asian Pacific Association for the Study of the Liver, Digestive Disease Week, and Asian Pacific Digestive Week, were also reviewed. Our study protocol was registered in PROSPERO (CRD: 42017067928). We used a predefined search strategy: (‘ledipasvir’ OR ‘sofosbuvir’ OR ‘simeprevir’ OR ‘daclatasvir’ OR ‘asunaprevir’ OR ‘ombitasvir’ OR ‘dasabuvir’) AND (‘HCV’ OR ‘hepatitis C’). We included DAAs other than SOF and RBV in our search terms in case some of the studies included other DAAs in their keywords but not SOF+RBV although the regimen was a part of their study. There were no language restrictions.
A secondary search consisted of a manual review of the selected articles’ reference lists. Authors were also contacted via their correspondence address to confirm that their studies were conducted in Asia and to identify additional studies conducted in the region. Demographic tables of all included studies were also reviewed for race and ethnicity to confirm that the studies included only Asians from Asia. Online supplementary list 1 shows a list of countries/areas included in the study. The list was based on the PubMed MeSH category list of Asia.18 We excluded premarket clinical trials after manually reviewing the full articles.
Supplemental material
Inclusion and exclusion criteria
We defined real-world evidence based on Sherman and colleagues.19 Eligible studies were conducted in Asia, where 12-week SOF+RBV treatment was prescribed for CHC GT2 in adult (≥18 years) patients in a real-world setting. All included studies were postmarket observational studies without additional interventions or surveillance beyond routine clinical practice studies. The primary outcome of SVR12 and/or secondary outcome of tolerability such as AEs and SAEs, RBV dose reduction, and/or early discontinuation were required for inclusion. For studies with multiple genotypes, all outcomes were categorised by genotypes for data analysis. We excluded studies with sample sizes of 10 patients or less.
Two reviewers (BW and FJ) independently screened articles initially by titles and abstracts, followed by full article review to identify eligible studies. Discordance results were resolved by discussion between the two reviewers and/or by consulting a third senior researcher (MHN).
Data extraction
We developed a case report form (CRF) for data extraction. The CRF included study information such as publication year, study location, study period, study centre and sample size; and study participants’ characteristics, including mean/median age, gender distribution, genotypes with subtypes, overall SVR12 rate, number of AEs and SAEs, RBV dose reduction and early treatment discontinuation. SVR12 rates for various patient subgroups were also recorded as available (eg, RBV dose reduction status, cirrhosis status, HCC status, prior treatment experience status, HCV GT2 subtypes (2a vs 2b), and age (<65 vs ≥65 years)).
Quality assessment
We developed a quality assessment scale for our study based on the Newcastle-Ottawa Scale (NOS) to evaluate risk of bias. This tool includes evaluation in selection, comparability and outcome dimensions of 9 scores in total. We considered studies with a total score of 8 or higher to be of high quality, 4–7 as fair quality and 1–3 as low quality.20 All studies included in the study analysis were evaluated by two reviewers. Discordance was discussed with a third review and resolved by consensus.
Statistical analysis
Meta-analyses were performed for overall study population and for various subgroups as mentioned above. For each outcome of interest, pooled estimates with 95% confidence intervals (CIs) were calculated using the DerSimonian-Laird method random-effects model.21 22 A Freeman-Tukey double arcsine transformation and Wilson score CI for individual studies were performed because SVR12 rates were expected to follow the binomial distribution; and in some subgroups, SVR12 rates were expected to approach the boundaries with extreme values.23 Heterogeneity was quantified by I2 statistics and Cochran Q test. We set I2 with cut-offs of 25%, 50% and 75% to suggest low (25%–50%), moderate (50% -75%) and high (>75%) heterogeneity, respectively.24
For subgroup analyses, we calculated the pooled SVR12 within each subgroup and tested the between-subgroup differences with the statistical level of significance defined with a P-value <0.05. If there were statistically significant differences between subgroups, a meta-regression was performed to quantify and to indicate the direction of difference by using separate estimates of the between-study variance. We also reported R2 index as a measure of the proportion of explained variation over the total estimated variation (R2 = T2explained/T2Total) to quantify the magnitude of impact of subgroup effectors.25
We evaluated for potential small study bias with the Egger’s test and Begg’s test, as well as the funnel plot.26 27
To evaluate for consistency among studies, we also performed sensitivity analyses for overall pooled SVR12 estimates, by executing meta-analyses on excluded abstracts, single-centre studies, sample sizes less than 100 or NOS quality scores lower than 8.
All analyses were carried out in R V.3.3.2 (R Foundation for Statistical Computing, Vienna, Austria) with ‘meta’ and ‘ggplot2’ packages.28–30
Results
Study characteristics
Figure 1 shows the summary of the search strategy and selection process in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.31 Following the previously described selection process, 13 studies including 12 articles from Japan and 1 from China, 3 conference abstracts and 10 full-text articles (with 1 written in Japanese) were included in the current study analysis.32–44 In total, 2208 participants with HCV GT2 from these 13 studies were eligible for the data synthesis (table 1). Seven studies specifically noted that decompensated patients were excluded.32 33 36 37 41 43 44 The other six studies did not provide specific information regarding this criteria.34 35 38–40 42 However, all these six studies were from Japan, where the practice at the time did not include patients with decompensated cirrhosis.

Screening of articles based on the PRISMA flow diagram. AASLD, American Association for the Study of Liver Diseases; APASL, Asian Pacific Association for the Study of the Liver; APDW, Asian Pacific Digestive Week; DDW, Digestive Disease Week; EASL, European Association for the Study of the Liver; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SVR12, sustained virological response 12 weeks after end of treatment.
Summary of included studies for systematic review and meta-analysis
Overall pooled SVR12 for SOF+RBV 12 weeks
A total of 13 studies (n=2208 patients) were included in our primary analysis, yielding an overall pooled SVR12 rate of 95.8% (95% CI 94.6% to 96.9%) (figure 2).32 34–44 There was low heterogeneity among the studies (I2=34.4%, P=0.11).

Overall sustained virological response (SVR12) to 12-week therapy with sofosbuvir and ribavirin for chronic hepatitis C genotype 2.
Adverse events
Ten studies provided AE data, RBV dose reduction and/or early discontinuation rate due to AEs.32 35–37 39–44 A total of 25.9% (95% CI 17.7% to 35.0%) of 1365 patients had RBV dose reduction, but only 0.7% (95% CI 0.3% to 1.2%) of 1720 patients discontinued therapy prematurely.32 35–37 39–44 The most common AE was anaemia (27.9%; n=968 patients from five studies, 95% CI 14.2% to 44.1%).32 39 41–43 Other common AEs were erythema or rash (5.5%, 95% CI 2.7% to 9.0%) and headache (3.2%, 95% CI 0.0% to 13.0%). SAEs (haemorrhagic gastric ulcer, bradycardia, haemolytic anaemia or severe anaemia and eruption) occurred in 2.0% of patients (95% CI 1.0% to 3.3%).32 39 43
Subgroup analyses
Pooled SVR12 in subgroup analyses
We performed subgroup meta-analysis and meta-regression by presence of RBV dose reduction in 1244 patients from 6 studies (online supplementary figure S1),32 36 40–43 by cirrhosis status in 1812 patients from 11 studies (figure 3),32 33 36–44 by prior treatment status in 1398 patients from 9 studies (figure 4),33 36 37 39–44 by presence of HCC in 1130 patients from 6 studies (online supplementary figure S2),32 36 37 39 42 43 by genotype subtypes in 1017 patients from 6 studies (online supplementary figure S3), and by age in 1012 patients from 6 studies (online supplementary figure S4).32 36 37 39 42 43 The results of all subgroup analyses are summarised in figure 5 and online supplementary table S1.

Forest plot and bubble plot for sustained virological response (SVR12) in patients with chronic hepatitis C genotype 2 treated with sofosbuvir and ribavirin, by cirrhosis status.
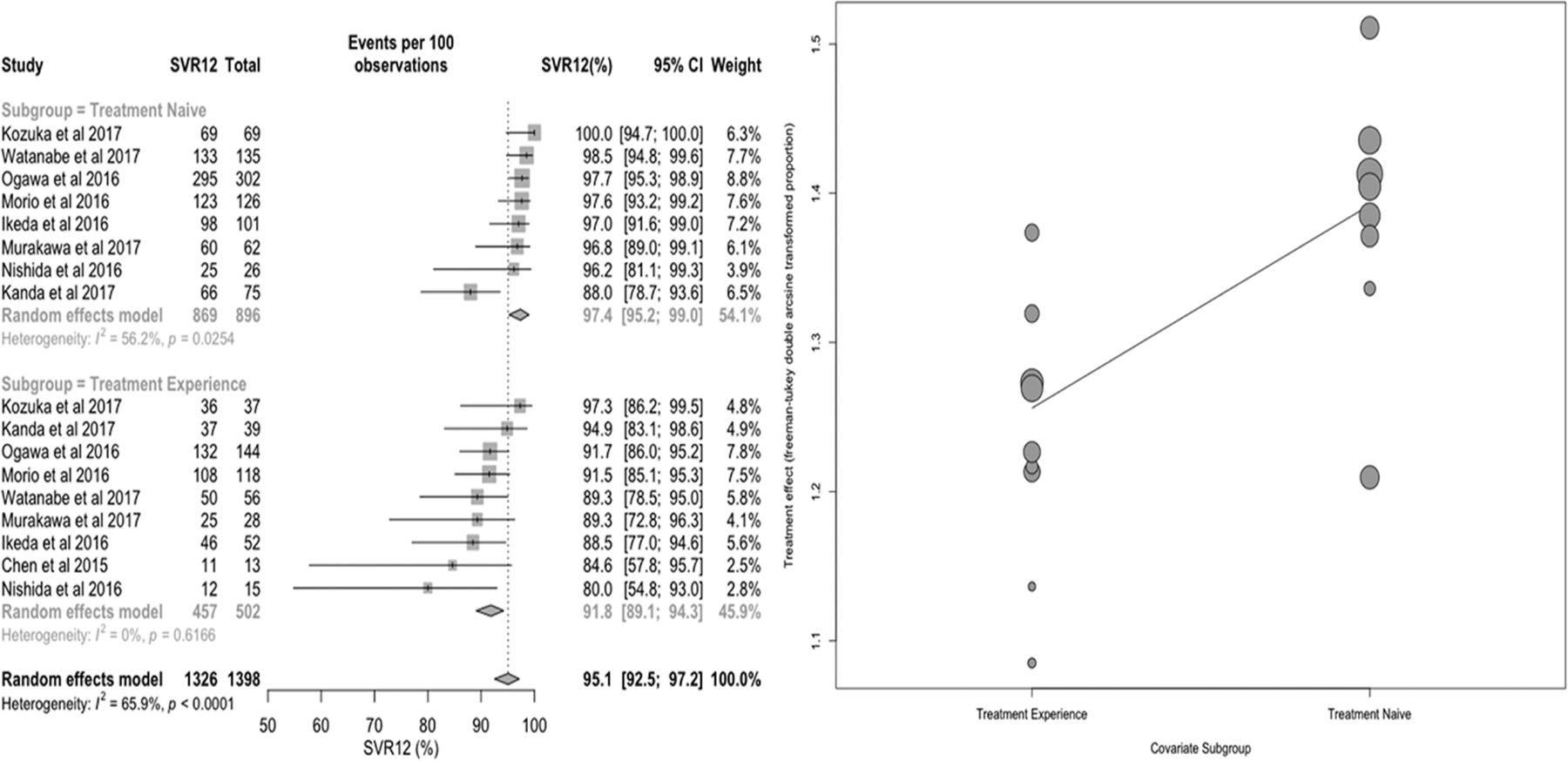
Forest plot and bubble plot for sustained virological response (SVR12) in patients with chronic hepatitis C genotype 2 treated with sofosbuvir and ribavirin, by treatment history.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary plots for overall and subgroup analyses in patients with chronic hepatitis C genotype 2 treated with sofosbuvir and ribavirin. HCC, hepatocellular carcinoma; RBV, ribavirin; SVR12, sustained virological response 12 weeks after end of treatment.
Subgroup analysis with meta-regression by cirrhosis status
There were significant differences in the pooled SVR12 rate between the cirrhotic and non-cirrhotic subgroups (figure 3 and online supplementary table S1). This analysis included 11 studies with 1290 non-cirrhotic patients and 522 patients with cirrhosis.32 33 36–44 The pooled estimate of SVR12 for non-cirrhotic and cirrhotic subgroups were 97.7% (95% CI 95.9% to 99.1%) and 91.3% (95% CI 88.1% to 94.1%), respectively (P<0.0001). Heterogeneity was low among the cirrhotic subgroup (I2=14.8%) but moderately high in the non-cirrhotic subgroup (I2=65.4%). In meta-regression analysis, compared with non-cirrhotic patients, patients with cirrhosis had 8.7% (95% CI 3.8% to 13.6%) lower chance of achieving SVR12. In addition, R2 index was 65.0%, indicating that cirrhosis status may contribute 65.0% of the overall observed heterogeneity.
Subgroup analysis with meta-regression by treatment history
There were also statistically significant differences in the SVR rates in patients by treatment history (figure 4 and online supplementary table S1). Nine studies provided data for this subgroup analysis.33 36 37 39–44 In total, there were 896 treatment-naive patients and 502 treatment-experienced patients (479 were interferon-experienced and 23 patients were not specified). The pooled SVR12 estimates were 97.4% (95% CI 95.2% to 99.0%) for the treatment-naïve subgroup and 91.8% (95% CI 89.1% to 94.3%) for treatment-experienced subgroups (P=0.0002). Heterogeneity was low in the treatment-experienced subgroup (I2=0.0%) but moderately high in the treatment-naïve subgroup (I2=56.2%). In meta-regression analysis, compared with treatment-naive patients, treatment-experienced patients had 7.2% (95% CI 2.5% to 11.9%) lower chance of achieving SVR12. In addition, the R2 index showed that 78.1% of the overall heterogeneity might come from patients’ treatment history.
SVR12 stratified by cirrhosis status and treatment history
We also did a stratified subgroup analysis by cirrhosis status and treatment history for the 573 patients with HCV GT2 with available data from three studies, which included 306 treatment-naïve non-cirrhotic patients, 71 treatment-naïve patients with cirrhosis, 128 treatment-experienced non-cirrhotic patients and 68 treatment-experienced patients with cirrhosis.33 37 43 We found that cirrhotic treatment-experienced patients (n=68) had the lowest SVR12 at 84.5% (95% CI 74.2% to 92.9%, I2=0.0%). On the contrary, treatment-experienced patients without cirrhosis (n=128) had much higher SVR12 at 96.4% (95% CI 92.1% to 99.2%, I2=0.0%). Treatment-naïve patients with cirrhosis (n=71) also had comparatively high SVR12 at 93.3% (95% CI 84.9% to 98.7%, I2=16.0%). As expected, treatment-naïve non-cirrhotic patients (n=306) had high SVR12 at 94.5% (95% CI 80.2% to 100.0%, I2=87.8%).
Other subgroup analysis
In the remaining subgroup meta-analyses, as shown in online supplementary table S1, there were no significant differences in pooled SVR12 rates in regard to RBV dose reduction, HCC, by age cut-off of 65 and by GT2 subtypes.
Publication bias
There was no significant publication bias for the studies included in the primary analysis of this study, based on the Egger’s test (P=0.10) and Begg’s test (P=0.14), as well as in the funnel plot (online supplementary figure S1).
Quality assessment and sensitivity analyses
The average score in the quality assessment was 6.7 (maximum score: 9 points). We considered studies with scores of 8 or higher to be high-quality studies, 4–7 to be fair, and less than 4 as poor. In total, there were six high-quality studies,32 37 39 40 43 44 six fair-quality studies,33 34 36 38 41 42 and one low-quality study (online supplementary table S2).35
We performed sensitivity analyses on full-text publication studies, multicentre studies, sample size greater than 100 participants and high-quality studies, and no significant differences showed on pooled SVR12, which were 95.6% (95% CI 94.2% to 96.9%), 95.9% (95% CI 94.9% to 96.8%), 95.9% (95% CI 94.7% to 96.9%) and 95.9% (95% CI 94.0% to 97.4%), respectively. The I2 dropped dramatically to 0.0% on multicentre studies analysis (online supplementary table S3).
Finally, we summarised the data from three important real-world studies completed in Western populations and the Asian population in this current real-world meta-analysis (online supplementary table S4).
Discussion
In our systematic review and meta-analysis of 13 studies and 2208 patients, we found that the 12-week SOF+RBV regimen was effective and well tolerated in real-world treatment of patients with HCV GT2 in Asia except for those with cirrhosis and treatment failure history. The overall pooled SVR12 rate was 95.8%, with only 0.7% early discontinuation rate. Approximately, a quarter of patients required RBV dose reduction, but the SVR12 rates for those with RBV dose reduction were still very high at 94.8%, which was not significantly different from those who did not require RBV dose reduction. Subgroup analyses also showed that no single patient characteristic significantly predicted lower SVR12, and only those who had both cirrhosis and a history of treatment failure had lower SVR12 (84.5%).
Although significant RBV reduction is known to reduce SVR in the Peg-IFN era, we did not find RBV dose reduction to have a substantial negative effect on SVR12 in our study. This finding could be due to the higher potency of the DAA sofosbuvir, such that treatment response was not as dependent on RBV as previous IFN-based regimens. In addition, since IFN also causes anaemia, it is possible that RBV dose reduction during the IFN era was more profound and/or occurred earlier in the treatment course.45 Finally, as the DAA treatment regimen only lasted for 12 weeks (vs 24–48 weeks in the IFN era), patients may have tolerated their haemoglobin decline better, resulting in less RBV reduction even in the dose reduction population. Compared with individual studies in which RBV dose reduction data were often available in only few participants, our study included 299 patients with RBV dose reduction from six real-world studies, thus allowing for more precise estimate of SVR12 and potential effects of RBV dose reduction on SVR12.
Previous phase III clinical trials for HCV GT2 in Japan, Korea, and Taiwan showed that SVR12 rates with 12 weeks of SOF+RBV therapy were about 98% in treatment-naive patients, >95% in treatment-experienced patients, >97% in non-cirrhotic, and 94% in patients with cirrhosis, with an overall anaemia prevalence rate of 12%.5 7 46 However, our study results for real-world effectiveness are slightly lower than previously reported for clinical trials. We found the overall SVR12 rate was 95.8%, with an SVR12 rate of 91.3% for patients with cirrhosis and 91.8% for treatment-experienced patients.
The lowest SVR12 rate was for those with both cirrhosis and prior treatment failure (84.5%). The lower SVR12 in patients with two or more difficult-to-treat characteristics has been previously described in other real-world studies with ombitasvir/paritaprevir/ritonavir±dasabuvir±RBV for GT1 and GT4, or simeprevir and SOF for GT1.47 48 Therefore, longer treatment duration with SOF+RBV has been suggested for some of the more difficult-to-treat populations.15
While the lower observed SVR12 in this real-world analysis compared with results from clinical trials is not totally unexpected, the differences were relatively small. Clinical trials generally select motivated patients with few comorbid conditions.49 In addition, clinical trial patients are also rigorously monitored with strict study visit schedule, whereas our analyses included patients treated in real-life practices who only had routine clinical monitoring and may have had various comorbidities. Nevertheless, the 12-week SOF+RBV therapy for patients with HCV GT2 was still more effective than the former 24-week Peg-IFN+RBV therapy (74%) even in the most difficult-to-treat group.50 Thus, our real-world data indicated that 12 weeks of therapy with SOF+RBV is effective in general for patients with HCV GT2 in Asia and for most HCV GT2 subgroups that have been historically more difficult to treat.
When compared with real-life studies from the Western world, our SVR rate was higher and closer to clinical trials results (online supplementary table S4). The overall SVR12 rates in real-world patients with GT2 treated with 12 weeks of SOF+RBV in Western countries ranged from 79.0% to 88.3%.13–15 One of the largest Western country studies published so far was from the US Veteran Affairs. The study consisted of 468 treatment-naïve and 151 treatment-experienced veterans with HCV GT2 who were treated with SOF+RBV for 12 weeks. This reported study results were demonstrably lower than in our reported analyses, including an SVR12 rate of 81.6% for treatment-naïve patients and 70.9% for treatment-experienced patients, and a much higher early discontinuation rate of 14.3%.13 Results from the Germany Hepatitis C Registry also reported a low SVR12 of 84.2%, 79.5%, 84.7% and 74.1% in treatment-naïve, treatment-experienced, non-cirrhotic patients with and patients with cirrhosis, respectively.14 Finally, an international cohort (mostly USA and no Asia), HCV-TARGET, reported an overall SVR12 rate of SOF+RBV for 12 weeks of 88.3% (91.0% in non-cirrhotic patients and 79.0% in patients with cirrhosis).15
These disparate results between our study findings and those from the Western world have been previously reported in the IFN-based therapy era. Potential explanations for Asian patients with HCV GT2 experiencing higher SVR12 rates include Asian patients having a more favourable IL28B genotype, which is associated with being more responsive to therapy, a lower body mass, which may allow for more drug bioavailability, as well as our exclusion of patients with decompensated cirrhosis in our meta-analysis.51 However, further study is needed to better understand the drug response differences in patients with HCV GT2 from Asia and the Western world. Newer pan-genotypic DAAs sofosbuvir/velpatasvir (Epclusa), sofosbuvir/velpatasvir/voxilaprevir (Vosevi), and glecaprevir/pibrentasvir (Mavyret) have been available in Western countries, and some of these have also recently become or soon to become available in parts of Asia.16 17 52 However, it is not clear when the reimbursement policy and cost of the newer regimens will become less prohibitive for most patients in Asia while generic SOF+RBV are available at relatively low cost in many areas.53 54
Our study has some limitations. Despite our extensive literature search, all but one study was from Japan due to the earlier approval of SOF in Japan, as well as the favourable medication reimbursement policy in this country.12 Therefore, our results may not be generalisable to non-Japanese Asian patients. This lack of data from other Asian countries other than Japan also highlights a real-world reality of the limited access to care and efficacious therapy for the vast majority of HCV-infected patients in Asia, suggesting the need for improvement of the access to care for this region. Additionally, although our study included a large number of patients for the overall analysis and several important subanalyses, the sample size was still limited for some subgroups, such as the one on HCC, which only included a total of 60 patients with HCC from six studies. In addition, the results from RBV dose reduction subanalyses were also limited by the fact that RBV dose reduction was done in real-world routine practice and did not follow standardised protocols as clinical trial. Thus, the data analysis was largely based on evaluable patient with evaluable SVR12 data. There was also some heterogeneity among the ‘upstream’ studies included in our meta-analysis. However, heterogeneity is unavoidable in meta-analysis, especially for real-world data, and the heterogeneities in our study were generally acceptable with I2<50% for our overall analysis as well as most of the subgroups analyses. We also performed meta-regression by cirrhosis status (11 studies) and treatment history (9 studies) to examine the effect of various moderators when data were available as per meta-regression principles.25
In conclusion, treatment with 12 weeks of SOF+RBV appears to be very effective overall and effective for various historically difficult-to-treat populations such as patients with cirrhosis, patients with prior treatment failure and older patients. Even though this treatment regimen may not be optimal for those with cirrhosis plus prior treatment failure, the SVR12 rate was 84%, which is a substantial increase compared with the prior IFN-based treatments, and offers patients a reasonable alternative until newer DAA regimens are available in Asia at acceptable costs. Further effort is needed to improve access to care and HCV cure for the vast majority of affected patients in this region.
Acknowledgments
The authors wish to thank Dr Akihiro Tamori, MD, PhD, and Dr Naoshi Nishida, MD, for their kind support and generous sharing of their study data, and Dr Guido Schwarzer, PhD, for his kind assistance with the R programming for our meta-regression analysis.
References
Footnotes
BW and FJ contributed equally.
Contributors BW and FJ: study design, data collection, data analysis, data interpretation, and drafting of the manuscript. YHY: data analysis, data interpretation and critical review of the paper. EO: data collection, data interpretation and critical review of the paper. RCC: study design, data collection, data interpretation and critical revision of the manuscript. CDS, SD, BZ, ZL, NF: data collection, data interpretation and critical review of the paper. MHN: study conception, study design, data collection, data analysis, data interpretation, drafting of the manuscript and supervision of the study. All authors read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests RCC: grant/research support, Gilead Sciences. NF: grant/research support: MSD, Gilead Sciences, Bristol-Myers Squibb and Janssen Pharmaceuticals; speaker’s bureau: Gilead Sciences, MSD, Bristol Myers, and Janssen Pharmaceuticals; advisory board: Gilead Sciences, AbbVie and Bristol-Myers Squibb. MHN: grant/research support: BK Kee Foundation, Asian Health Foundation, Bristol-Myers Squibb, Gilead Sciences, Janssen Pharmaceutical, National Cancer Institute, and Pfizer; pharmaceutical; advisory board member or consultant: Dynavax Laboratories, Gilead Sciences, Intercept Pharmaceuticals, Alnylam Pharmaceutical, Bristol-Myers Squibb, Novartis Pharmaceutical and Janssen Pharmaceutical.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Presented at This study had been presented as poster at the 2017 AASLD Conference.