Article Text

Abstract
Background Severe colitis flare from ulcerative colitis (UC) or Crohn’s disease (CD) may be refractory to corticosteroids and antitumour necrosis factor (TNF) agents resulting in high colectomy rates. We aimed to describe the utility of tacrolimus to prevent colectomy during second-line vedolizumab initiation after corticosteroid and anti-TNF treatment failure in paediatric severe colitis.
Methods A retrospective cohort analysis was performed between 1 October 2014 and 31 October 2016 at a single tertiary care centre. Inclusion criteria were patients with severe colitis who received tacrolimus before or during vedolizumab induction and previous exposure to anti-TNF therapy with or without corticosteroids. The initiation of tacrolimus was clinician dependent based on an institutional protocol.
Results Twelve patients (10 UC, two CD; median age 16 years; three female) received at least one dose of vedolizumab 10 mg/kg (max of 300 mg) due to anti-TNF therapy failure and persistent flare not responsive to corticosteroids. Of the 12 patients, eight (67%) and four (33%) had failed one or two anti-TNF agents, respectively. Tacrolimus was initiated for acute disease severity during hospitalisation (58%) or ongoing flare during outpatient care (42%). 9 (75%) of 12 patients avoided colectomy or inflammatory bowel disease-related surgery at 24 weeks and eight (68%) continued on vedolizumab maintenance with no adverse events out to 80 weeks.
Conclusion We report real-world data on the outcome of tacrolimus around vedolizumab initiation in paediatric UC or CD after corticosteroid and anti-TNF therapy treatment failure. Our pilot experience indicates a potential benefit of concomitant tacrolimus when initiating vedolizumab therapy.
- vedolizumab
- tacrolimus
- acute severe colitis
- colectomy
- ulcerative colitis
- Crohn’s disease
- inflammatory bowel disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- vedolizumab
- tacrolimus
- acute severe colitis
- colectomy
- ulcerative colitis
- Crohn’s disease
- inflammatory bowel disease
Summary box
What is already known about this subject?
Severe colitis from inflammatory bowel disease (IBD) can be refractory to antitumour necrosis factor (TNF) agents, and corticosteroid dependency may result in high morbidity or unacceptable side effects, particularly in paediatric patients.
Vedolizumab is an acceptable second-line maintenance biologic, but therapeutic onset can take 8–12 weeks.
It is unknown whether tacrolimus may be an effective, corticosteroid-sparing ‘bridge’ therapy from anti-TNF failure to vedolizumab maintenance in severe colitis.
What are the new findings?
We present a standardised protocol for concomitant tacrolimus therapy in severe IBD colitis who have failed anti-TNF therapy and initiating vedolizumab induction.
A pilot cohort analysis indicates a 75% probability of avoiding colectomy using concomitant tacrolimus with vedolizumab therapy.
There was a 67% of successfully continuing on vedolizumab maintenance with no adverse events out to 80 weeks.
How might it impact clinical practice in the foreseeable future?
Understanding available medical treatment options in severe IBD is important to optimise health outcomes. Standardising concomitant tacrolimus use—possibly underutilised in clinical IBD management—may decrease corticosteroid dependency and toxicity, reduce IBD-related surgery rates and bridge therapeutic momentum when transitioning between maintenance biologic agents.
Introduction
When inflammatory bowel disease (IBD), consisting of ulcerative colitis (UC) or Crohn’s disease (CD), presents with treatment-refractory severe colitis, hospitalisation is often required and IBD-related surgery, including total colectomy and diverting ileostomy, is considered to be part of standard of care. Children with severe IBD colitis, compared with adults, are more likely to be refractory to corticosteroids and require escalating medical therapy including anti-TNF agents.1 2 Reported colectomy rates in paediatric severe colitis were approximately 40% at 1 year.3 Colectomy rates in paediatric patients with IBD refractory to corticosteroids were 20% at 6 months and 60% at 26 months.4
Traditionally, antitumour necrosis factor (TNF) agents, especially infliximab, are considered first-line biologics in severe IBD colitis with varying response rates. More recently, vedolizumab, a humanised monoclonal antibody α4–β7 integrin receptor antagonist,5 demonstrated clinical benefit in small, retrospective paediatric studies.6 It was approved by Food and Drug Administration in May 2014 to induce and maintain remission in adults with UC or CD who have an inadequate response to anti-TNF agents, immunomodulators, corticosteroids or demonstrated steroid dependence.7–9 Onset of therapeutic response is often seen at 8–12 weeks. It is unknown whether tacrolimus, a calcineurin inhibitor, can be safely and effectively used as concomitant therapy during vedolizumab initiation in patients with IBD previously refractory to first-line biologics and corticosteroids.
In this study, we aimed to describe the utility of tacrolimus to prevent colectomy during second-line vedolizumab initiation after corticosteroid and anti-TNF treatment failure in paediatric severe colitis.
Methods
We performed a retrospective analysis of inpatient and outpatient vedolizumab initiation between 1 October 2014 and 31 October 2016. Hospital-wide longitudinal data were available from a total of 123 infusions, representing a total of 21 unique patients. Patient-level information from electronic medical records was cross-referenced with electronic pharmacy records of inpatient and outpatient medication history of corticosteroids, anti-TNF agents and tacrolimus. Patients with severe colitis (UC or CD) who received at least one vedolizumab infusion and were initiated on tacrolimus were included in the analysis. Patients with any abdominal surgery prior to vedolizumab initiation were excluded from the study. Negative cytomegalovirus (CMV) status was confirmed by histology and immunohistochemistry staining from ileal-colonic biopsies. A Kaplan-Meier analysis was performed from the IBD-related surgery data for the cohort.
Tacrolimus bridge therapy protocol
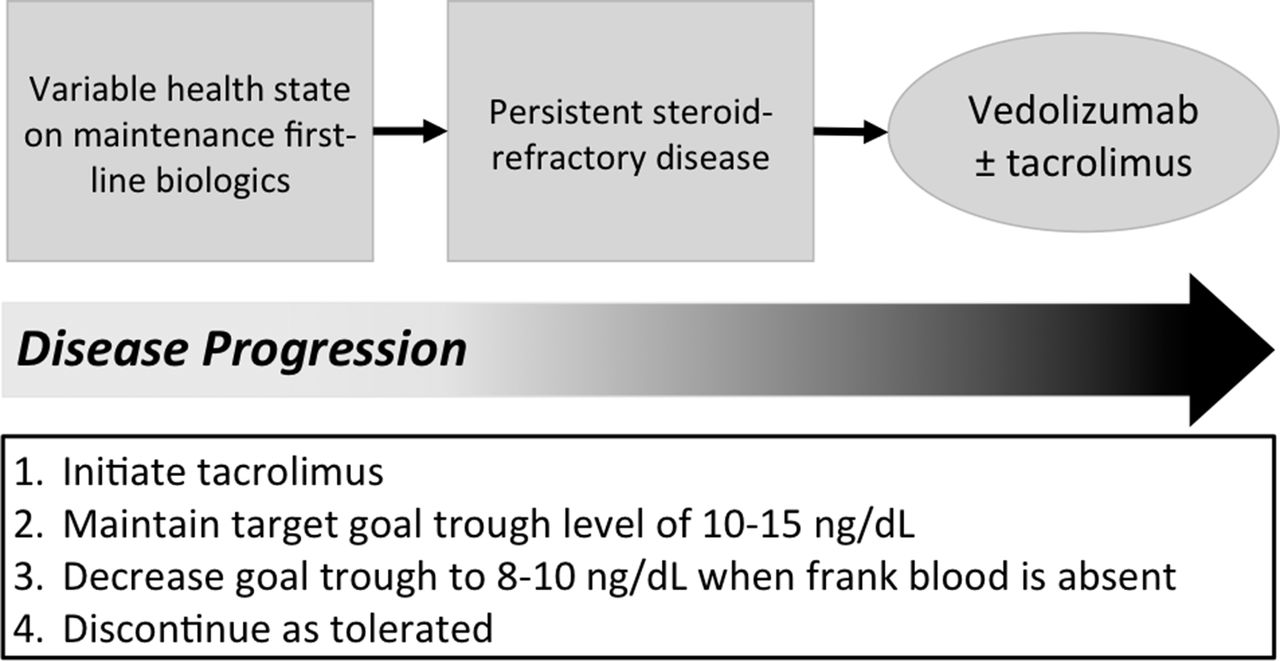
As per institution protocol, tacrolimus was initiated as bridge therapy to vedolizumab based on progression of disease and attending physicians’ clinical judgement using the care pathway as outlined in figure 1. Serum tacrolimus levels are followed within a week of therapy initiation with a goal trough of 10–15 ng/dL and decreased to 8–10 ng/dL in the absence of visible blood in the stool. Tacrolimus therapy was discontinued when vedolizumab maintenance therapy was determined to reach therapeutic efficacy along with each patient’s overall clinical improvement.

Tacrolimus bridge therapy protocol. Institutional care pathway for tacrolimus therapy as bridge to vedolizumab maintenance.
Results
A full description of the cohort’s patient characteristics is shown in table 1. Individual patient-level biologic history is shown in table 2. A total of 13 patients were identified meeting inclusion criteria. One patient was excluded due to loss of follow-up. A total of 12 paediatric patients with IBD (25% female) with severe colitis (Paediatric Ulcerative Colitis Activity Index >65 for UC and Pediatric Crohn’s Disease Activity Index >35 for CD) treated between 1 October 2014 to 31 October 2016 were included in the analysis. All patients received at least 1 dose of vedolizumab 10 mg/kg (max of 300 mg total) due to anti-TNF therapy failure, corticosteroid dependency or failure and persistent disease exacerbation. All patients were concomitantly treated with tacrolimus as bridge therapy to vedolizumab induction. None of the 12 patients had evidence of or required treatment for active CMV colitis. Median age at vedolizumab initiation was 16 years with a range of 7–19 years. Seven (58%) were hospitalised due to acute disease severity. Ten (83%) had UC and two (17%) had CD. Prior to initiating vedolizumab, infliximab was used in nine (75%) and adalimumab in three (25%).
Patient characteristics
Patient-level biologic therapy history
Kaplan-Meier analysis is shown in figure 2. Among the 12 patients, nine (75%) achieved clinical remission without requiring IBD-related surgery. One of the nine switched back to anti-TNF therapy after initiating vedolizumab. The probability to avoid surgery and remain on corticosteroid-free vedolizumab maintenance at 24 weeks was 68% (eight out of 12) with no further events out to 80 weeks. At the end of follow-up, four of eight (50%) were able to discontinue tacrolimus. Patient-specific timing of tacrolimus in relation to vedolizumab intiation among the 12 patients is shown in figure 3.

Probability of avoiding colectomy in paediatric severe IBD colitis. The probability to avoid colectomy at 24 weeks was 75% (9 of 12) (not shown) in the entire cohort and 68% (8 of 12) in patients who maintained on vedolizumab with no additional events out to 80 weeks.

{kind=link}
{kind=link}
{kind=link}
Timing of tacrolimus in relation to vedolizumab initiation. The duration of therapy is charted for the vedolizumab+tacrolimus group (n=12). The vertical line at time 0 indicates the relative start date of vedolizumab for each patient. Horizontal bars represent the relative start, duration and stop date of tacrolimus. Clear bars (n=3) represent patients who had colectomies. Light grey bars (n=4) represent patients who were able to discontinue tacrolimus and maintained on vedolizumab maintenance. Dark grey bars (n=4) represent patients who were maintained on vedolizumab+tacrolimus until the end of study follow-up. The solid black bar (n=1) represents the patient who was switched back to antitumour necrosis factor from vedolizumab therapy.
Discussion
We report real-world outcomes data on vedolizumab therapy in paediatric severe IBD colitis after treatment failure of anti-TNF therapy and corticosteroids. There is increasing use of vedolizumab as a second-line biologic therapy in paediatric UC and CD. Onset of therapeutic response for vedolizumab is often seen at 8–12 weeks. Given this delayed onset of action, longer-term corticosteroid exposure is often necessary as temporary ‘bridge’ therapy. In our investigation, we report the experience of using tacrolimus, a calcineurin inhibitor, as a corticosteroid-sparing alternative therapy. Our report is the first to propose the utility of concomitant tacrolimus bridge therapy between anti-TNF withdrawal to vedolizumab maintenance.
Tacrolimus has been previously shown to have benefit in steroid-refractory paediatric IBD and carries a fairly limited and reversible side effect profile without the gradual weaning of corticosteroids.4 10 Our finding that approximately 75% of patients with treatment-resistant colitis are able to avoid IBD-related surgery corroborates the limited literature10–12 using tacrolimus as rescue therapy in paediatric acute severe colitis. We acknowledge the need to further validate findings of safety and efficacy in future, larger-scale longitudinal studies generalisable to children and adults with IBD. Specifically, our report serves to support the rationale for larger-scale studies evaluating tacrolimus bridge during biologic induction therapy for severe colitis.
In summary, tacrolimus therapy may be useful as bridge therapy when transitioning between maintenance therapy options in moderate-to-severe IBD. In steroid-dependent patients who endure adverse side effects, including progressive bone loss, growth stunting in children, Cushingoid features, hypertension, tacrolimus may be a strategic and underutilised therapy in the IBD treatment armamentarium, particularly as a temporary, non-maintenance therapy.
References
Footnotes
Contributors BH and KTP contributed equally to the design of the study. BH, MW and EOH collected and analysed the data. BH and KTP wrote the article and all the other authors contributed with critical revision of the manuscript for important intellectual content and interpretation of the data. All authors read and approved the final version of the manuscript.
Funding No funding was obtained for this research. KP has received research support from Janssen and Takeda unrelated to this work.
Competing interests None declared.
Patient consent Not required.
Ethics approval Stanford University Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it first published. The spelling of the word ’corticosteroid' in the article title has been corrected.