Article Text

Abstract
Objectives Patients with clinical, genetic and histological features of coeliac disease (CD), but negative for serological markers, pose a significant clinical problem. The aim of this study was to outline a specific profile, and to evaluate the natural history and response to gluten-free diet (GFD) of patients with seronegative CD.
Methods patients with duodenal mucosa damage Marsh I, II and III stages, HLA DQ2/DQ8 haplotype and clinical features suggestive of CD, but negative for CD serology, were defined as seronegative CD patients. Other common causes of duodenal mucosa damage were excluded. HLA–DR and DQ genotype/haplotype between all Marsh stages of patients with seronegative and seropositive CD were compared. Clinical features, laboratory testing and histological findings were evaluated after a GFD and a gluten rechallenge. A long follow-up period was available.
Results 48 patients fulfilled diagnostic criteria over a 4-year period. Clinical phenotype and HLA−DR and DQ frequencies between patients with seronegative and seropositive CD was similar. However, Marsh I stage was more prevalent in seronegative patients (42% vs 22%; p<0.05). After a 1-year GFD trial, clinical symptoms, histological features and laboratory testing improved in 40 patients and worsened in those who underwent a 6-months gluten challenge. Five patients with seronegative CD (25%) experienced the occurrence of autoimmune diseases during a median follow-up of 133 months (range 72–192).
Conclusions Patients with seronegative CD did not display a specific profile. They benefitted from GFD as patients with seropositive CD. Waiting for more sensitive serological markers, the diagnosis of seronegative CD remains a diagnosis of exclusion.
- COELIAC DISEASE
- DUODENAL MUCOSA
- ABDOMINAL PAIN
- GLUTEN FREE DIET
- MALABSORPTION
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Seronegative coeliac disease occurs in a small proportion of patients.
▸ The diagnosis and treatment of patients with seronegative coeliac disease pose a clinical problem.
What are the new findings?
▸ In patients with seronegative coeliac disease, homozygosity for HLA–DQ-B1*02 genotype is less frequent compared with patients with seropositive coeliac disease.
▸ Clinical, histological and laboratory parameters improved in patients with seronegative coeliac disease following a gluten-free diet trial.
▸ Natural history of patients with seronegative coeliac disease is similar to patients with seropositive coeliac disease.
How might it impact on clinical practice in the foreseeable future?
▸ Waiting for more sensitive serological markers, the diagnosis of seronegative coeliac disease remains a diagnosis of exclusion.
▸ A long-term gluten-free diet is still the best treatment option in patients with seronegative coeliac disease.
Introduction
Coeliac disease (CD) is an immune-mediated disease characterised by inflammation and injury of the mucosa of small intestine following the ingestion of gliadin, a protein found in gluten, in genetically predisposed individuals.1 ,2 More specifically, CD occurs in carriers of HLA–DQ2 and/or DQ8 alleles, although HLA-unlinked loci may also contribute to the genetic susceptibility of the disease.3 Interactions between environmental and genetic factors are essential to trigger the immunological cascade leading to a complete loss of villi and nutrient malabsorption as a consequence.4 ,5
The first approach to diagnose CD is non-invasive.6 ,7 The preferred test is based on serology while patients are on a free diet. IgA anti-tissue transglutaminase (TTG) antibody is the most recommended test given its high accuracy. In patients with increased risk to develop CD, IgG-deamidated gliadin peptides (DGPs) may also be tested. Baseline IgA endomysial antibody (EMA) should be assessed in patients on a gluten-free diet (GFD).7 Patients with positive serologic tests should undergo an upper endoscopy with small-bowel biopsy to confirm the diagnosis of CD. The diagnosis is presumptively established when there is concordance between the serologic and the biopsy findings. However, it is definitely confirmed when symptoms improve following gluten avoidance.8 Demonstration of histological normalisation is not always required. In clinical practice, there are occasionally individuals with negative serologic tests despite the presence of features suggesting CD. These patients should be tested for HLA-DQ2 (DQA1*05; DQB1*02) and/or DQ8 (DQA1*03; DQB1*0302) haplotypes because CD is highly unlikely to occur in patients lacking these haplotypes.9 In positive patients, small-bowel biopsies are needed to confirm the diagnosis. Histologic findings in the duodenal mucosa are usually described using the Marsh-Oberhuber classifications.10 ,11 They may be characterised by solely a mild increase of intraepithelial lymphocytes (IEL), or enhanced apoptosis and crypt hyperplasia, up to a complete loss of villi and total mucosal atrophy.10 ,11 However, lymphocytic infiltration of the intestinal epithelium and villous atrophy are not specific for CD and may be present in a variety of other disorders such as small-intestinal bacterial overgrowth, Crohn disease, giardiasis and a number of other less frequent causes.12 Demonstration of histological and laboratory tests improvement and/or normalisation is always required after 6–24 months of a GFD, because a subgroup of patients with irritable bowel syndrome may have symptomatic benefit from a GFD.13 Owing to this phenomenon, some authorities recommend to repeat duodenal biopsy after a gluten rechallenge, although this approach remains uncertain, and more importantly, quite unpleasant for patients.
In this study, patients with different Marsh stages with clinical, histological and genetic features suggestive of CD but negative for serological markers were investigated and compared with patients with seropositive CD. In addition, natural history and response to a GFD and gluten rechallenge were evaluated.
Methods
Study design
This was a prospective cohort study. In the first step, patients with a ‘presumptive’ diagnosis of CD based on clinical features, HLA-DQ2 and/ DQ8 alleles and small-intestine histology, but negative for serology were enrolled in the study. Although the major Gastroenterological Societies2 define seronegative CD patients as those with villus atrophy, in order to make easier for readers, in our study the definition of ‘seronegative’ CD also included patients with Marsh I and II stages. Phenotype and HLA–DR and DQ haplotypes of patients with seronegative CD were compared with patients with seropositive CD. Seronegative patients were invited to undergo a GFD for 12 months followed by a second endoscopy with duodenal biopsy, laboratory testing and clinical assessment. In the third step, patients with seronegative CD were checked by an additional duodenal biopsy at the end of a full gluten challenge. A follow-up of patients with seronegative CD was also available.
Setting
Patients attending the Coeliac Disease Centre at the Clinica Medica, University of Sassari, Italy, from 2000 to December 2004, were evaluated for this study. The Clinica Medica hospital is a tertiary referral centre that provides care for patients with gastrointestinal problems including most adult cases of CD in Northern Sardinia. The population of this region is entirely white and one of the most genetically homogeneous in the world.14
Inclusion criteria
Patients with CD on the basis of clinical features, proximal small-intestinal biopsies compatible with CD according to Marsh classification and positive for HLA-DQ2 and/or DQ8 alleles but negative for serology markers were enrolled in the study. Written informed consent was obtained from each patient. The protocol was approved by the local ethics committee, Azienda Unità Sanitaria Locale N 1, Sassari, Italy.
Exclusion criteria
Patients with Helicobacter pylori infection, ova and parasites such as giardiasis and/or other intestinal infections in the stool, Crohn disease, small-intestinal bacterial overgrowth, drug-induced enteropathy and established diseases including liver and pancreas disease or cancer, and eosinophilic infiltrate in duodenal specimens were excluded from the study.
Control group
Patients with a new diagnosis of seropositive CD were evaluated in the same fashion as that of patients with seronegative CD. Clinical features, laboratory testing and genotyping were compared between patients with seropositive and seronegative CD.
Patient work-up
Before enrolment, patients underwent a diagnostic approach as follows:
History and clinical examination.
Laboratory tests: complete blood count, erythrocyte sedimentation rate, C reactive protein, protein electrophoresis, B12 vitamin and folic acid levels, ferritin, iron, calcium, thyroid hormones, serum immunoglobulins, albumin, triglyceride, cholesterol, liver and pancreas function tests and glycaemic levels.
Stool samples were examined for ova, bacteria and parasites.
Serology markers for CD: IgA and IgG antibodies for native gliadin (AGA), EMA and TTG.
Breath tests (BTs): the presence of H. pylori infection was confirmed by 13C-urea BT (UBT). Lactose malabsorption and small-intestinal bacterial overgrowth were assessed by conventional hydrogen BT.
Endoscopy: each patient underwent upper endoscopy. Tissue specimens were taken from the antrum, angulus, and from the corpus of the stomach. Three additional biopsies were obtained from the duodenum.
HLA–DQ2/DQ8 proteins.
Diagnostic criteria
Serology
Antibody testing was based on the identification of IgA and IgG TTG antibodies by a validated, standardised and reliable commercial kit (Eurospital, Trieste, Italy). IgA and IgG AGA antibodies were assessed by the immunocup system (Pharmacia & Upjohn Diagnostic, Uppsala, Sweden) and IgA EMA antibodies were detected by indirect immunofluorescence on monkey oesophagus (ALPHADIA sa/nv, Diagnostic Products, Wavre, Belgium).
Breath tests
The presence of H. pylori infection was confirmed by 13C-urea BT (AB Analitica Srl, PD, Italy).15 Lactase status was evaluated using the conventional hydrogen BT after ingestion of 25 g of lactose. Small-intestinal bacterial overgrowth was assessed by hydrogen BT after administering a dose of 50 g of glucose.16
Histology
Mucosal sections were evaluated by two expert gastrointestinal pathologists (VV and AM) independently. In the case of CD histologic features, the Marsh classification was applied. Briefly, a Marsh I stage corresponded to a cut-off of >25 IEL per 100 enterocytes, increased IEL associated with crypt hyperplasia was classified as Marsh II, and partial, subtotal or total villi atrophy as Marsh IIIa, IIIb and IIIc, respectively. The presence of CD3 lymphocytes was also confirmed by immunostaining.
HLA-DQ2/DQ8 proteins
The presence of HLA-DQ2/DQ8 was assessed by an ELISA commercial kit (Eurospital, Trieste, Italy).
Genotyping
DNA was extracted using the Chelex method. PCR amplification of the polymorphic second exon of the HLA-DRB1, DQB1 genes and dot-blot analysis of amplified DNA with sequence-specific oligonucleotide (SSO) probes were carried out as previously reported.17
Statistical analysis
Mann-Whitney U test was used to compare the age of seronegative versus seropositive CD patients at diagnosis, as well as the other continuous variables. Pearson χ2 test was used to compare the categorical variables between the patient subgroups. For histological analysis, the Marsh IIIa, IIIb and IIIc categories were merged together.18 Similarly, the presence of osteoporosis and osteopenia was recoded into a single category.
The association of the Class II HLA–DR-DQ haplotypes with CD was assessed with data points arranged in contingency tables and assessed by the Fisher's exact test. Haplotypes were grouped for DQ2 according to their association with DR3 haplotype or with DR5/DR7 haplotypes. DQ8, encoded by DQB1*0302 allele, is generally associated to DR4 haplotype.
All tests were performed as two-tailed and differences were considered statistically significant when p<0.05. Statistical analysis was carried out using SPSS V.16.0 software (SPSS Institute, Illinois, USA).
Results
First step
A total of 48 patients with a median age of 36 years; range 16–76, were included in the study (40 female patients; F/M 5:1). All cases were negative for CD serology markers (except four for AGA IgG and one for AGA IgA) and positive for histological alterations in the small-intestinal mucosa according to Marsh classification, CD3 immunostaining and HLA DQ2/DQ8 alleles. Patients were tested for bone mineral density and invited to undergo a GFD for 12 months (figure 1).
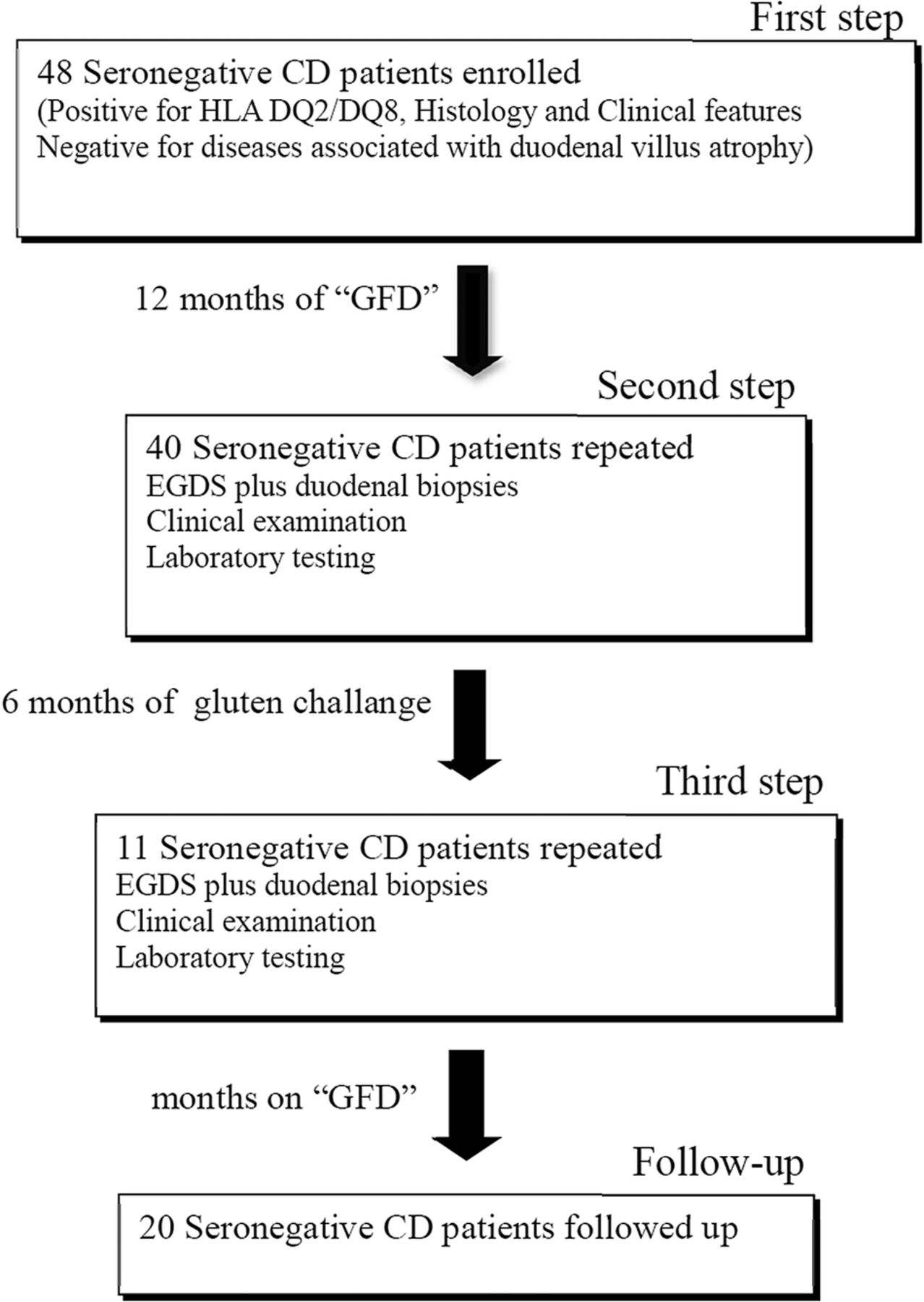
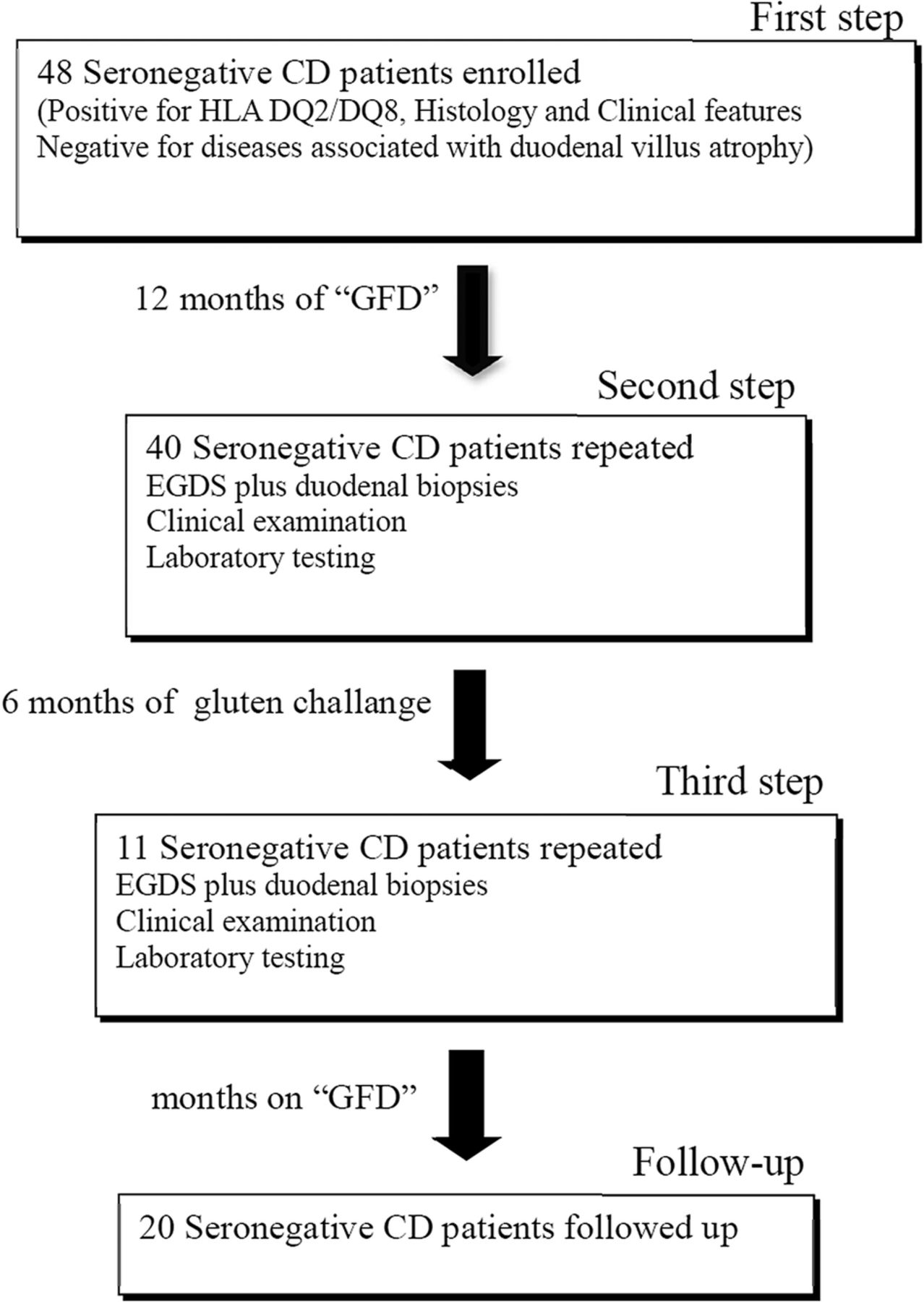{kind=link}
Flow diagram of the patients with seronegative coeliac disease prospectively studied according to each step.
Patient features
Clinical features of patients with seronegative CD are shown in table 1. Abdominal pain lasting for at least 1 year, in the majority of cases associated with abdominal bloating, was the most common symptom (44/48; 92%). Laboratory tests were altered in most patients (table 1). Notably, low IgA levels were not detected in any patient.
Clinical features of 85 patients with seropositive coeliac disease and 48 patients with seronegative coeliac disease at the baseline and after 1 year of gluten-free diet
A high proportion of patients (63%) displayed lactose malabsorption; however, it was not considered to be the sole cause of intestinal injury. Autoimmune disorders were associated with seronegative CD only in few cases (type I diabetes in one patient, Hashimoto's thyroiditis in five patients). In six patients, a non-herpetiformis dermatitis was observed. Use of angiotensin II inhibitors, nowadays known to be harmful for intestinal mucosa,16 was not recorded in any of the 48 studied patients with the exception of one 67-year-old female patient, who was taking enalapril.
Histology
According to the Marsh classification, the most observed lesion in the duodenal mucosa of patients with seronegative CD was Marsh I (20/48; 42%). Surprisingly, 15 patients displayed Marsh III (table 1).
Seronegative and seropositive patients
Patients with seronegative CD were compared with 85 patients with seropositive CD (table 1). Median age and gender ratio (F/M 5:1 vs F/M 4:1) between the two CD groups were similar. Reported abdominal symptoms were more frequent in seronegative CD (92% vs 76%, p=0.029), whereas family history of CD was more frequent among patients with seropositive CD (37% vs 17%, p=0.011). Overall, patients with seronegative CD did not display a specific laboratory profile, moreover alterations of biochemical tests were, in general, less common than in patients with seropositive CD. In addition, severe duodenal mucosal damage (Marsh II–III) was observed less frequently in patients with seronegative CD compared with patients with seropositive CD (58% vs 78%, p=0.019) (table 1). This may explain the lower frequency of lactose malabsorption in patients with seronegative CD compared with patients with seropositive CD (63% vs 91%, p=0.0001). Autoimmune diseases such as diabetes type 1 and Hashimoto's thyroiditis and an established mild anxiety-depression syndrome as well as non-herpetiformis dermatitis were more often associated with patients with seronegative CD. Instead, osteopenia and/or osteoporosis were more frequent in patients with seronegative CD than in patients with seropositive CD. Additional analyses were performed in order to compare Marsh II and III stages of seronegative CD patients with seropositive CD patients (see online supplementary material).
supplementary data
Genotyping
Class II HLA haplotypes were assessed in 32 patients with seronegative CD and in 62 patients with seropositive CD. Findings were also compared with the Sardinian general population.17 The frequency of HLA–DR and DQ haplotypes is presented in table 2. As expected, almost half of seropositive patients were homozygous for HLA-DR3-DQB1*02 and HLA-DR4-DQB1*0302 haplotypes which are strongly predisposing for CD. On the contrary, among seronegative patients, the frequency did not differ significantly from that of the general population. Moreover, the frequency of homozygotes DQB1*02, usually associated with a more severe disease, was twofold higher in patients with seropositive CD (38.1% vs 15.2%) compared with seronegative CD (data not shown). Notably, none of the seronegative patients was negative for alleles predisposing to CD.
Distribution of HLA-DR and DQ haplotypes in patients with seropositive and seronegative coeliac disease and in a population of 631 controls from Sardinia17
Second step
After 1 year of GFD, patients were interviewed for diet compliance and symptoms. A straight adherence to GFD was recorded for 44 patients (92%). Four patients reported difficulties to completely adhere to the GFD. All patients were invited to repeat the esophago–gastro–duodenoscopy (EGDS) with duodenal biopsy and laboratory testing (figure 1). Among the 48, 40 patients agreed, 34 were females; median age 36 years (range 22–69) (table 1). There was a dramatic improvement of abdominal symptoms that was statistically significant among patients with seronegative CD that completely adhere to GFD. In addition, haemoglobin levels gained normalisation in all five patients and folate was in the reference range in six patients out of seven (86%) (table 1). More interesting, Marsh III mucosal duodenal injury resolved in 14 patients out of 15 (93%), out of 40 undergoing EGDS, and a complete restitutio ad integrum was observed in 13 patients (table 1). Bone mineral density significantly increased in the lumbar spine and femoral neck compared with previous examination (table 1).
Third step
Patients with seronegative CD on GFD for up to 12 months and re-evaluated for duodenal mucosa features were invited to undergo a gluten challenge (figure 1). Among 40 patients, 19 agreed to follow a gluten-rich diet trial. However, eight patients avoided food containing gluten after few weeks because of the occurrence of abdominal symptoms. All 11 patients underwent a third EGDS with duodenal biopsies after 6 months of free diet. Examination of duodenal specimens according to Marsh classification showed no patient with Marsh 0, three patients with Marsh I, eight patients with Marsh II and no one with Marsh 3, respectively (table 3). All patients reported recurrence of gastrointestinal symptoms.
Comparison of duodenal mucosa findings according to Marsh classification in patients with seronegative coeliac disease after 1 year of gluten-free diet followed by a gluten challenge
Follow-up
Twenty patients were available for the follow-up after a median of 133 months (range 72–192 months) (table 4). The majority (90%) were female patients. Three of them developed autoimmune thyroiditis, and inflammatory bowel disease, ulcerative colitis and Crohn disease, respectively, occurred in two patients.
Comorbidity developed by 20 patients with seronegative coeliac disease during the follow-up period (median=133 months; range 72–192 months)
Discussion
In clinical practice, CD negative for serological markers is a problem for the physician and the patient. First of all, to differentiate between seronegative CD and other causes of duodenal mucosal injury needs an extensive work-up; second, treatment and follow-up of patients with seronegative CD pose a clinical dilemma.19
Over a 4-year period, among patients with gastrointestinal symptoms seen at our single tertiary-care referral centre, a definitive diagnosis of seronegative CD was established in 48. An interesting finding in our cohort was the high number of patients who improved their symptoms after a period of GFD and, more importantly, the restitutio ad integrum of intestinal mucosa observed in the majority of patients in the duodenal specimens obtained at the second upper endoscopy. Notably, patients with seronegative CD with stigmata of malabsorption experienced normalisation of laboratory parameters, especially haemoglobin and folate serum levels, according to restoration of the intestinal villi following GFD. These findings support our initial choice to recommend a GFD trial in patients with seronegative CD, although the benefit of a lifelong GFD in order to prevent autoimmune diseases, usually associated with CD, is not so obvious according to our findings. In fact, in our patients with seronegative CD followed up for several months (133), the occurrence of autoimmune diseases was observed in 25% who were given the GFD. However, these results can be partially explained by the fact that genes predisposing to CD are also involved in other autoimmune diseases such as thyroiditis and diabetes, both diseases in Sardinia have one of the highest prevalence in Europe.20 ,21
At the moment, we do not have an explanation for negative serum markers in CD. Usually, TTG IgA and endomysial IgA are highly sensitive and specific for CD, whereas anti-gliadin antibody testing is not.21–23 Some authors explain seronegativity as the inability of anti-TTG passage into the bloodstream.24–26 For example, in seronegative CD children with Marsh I stage, Tosco et al25 found deposits of TTG bound with IgA in the duodenal mucosa by immunofluorescence. An additional study observed a clinical improvement following a GFD in patients with increased presence of IELs in the duodenal mucosa and in ten of them deposits of immunocomplexes.26
The newer DGP assay is also highly sensitive and specific for CD and has been shown to detect patients who were seronegative by TTG testing;27 ,28 however, at the time of patient enrolment antibodies to DGP were not yet available. In addition, it has been reported that CD markers may be negative in the presence of partial villus atrophy such as in subclinical or silent CD.29 This could justify negative CD markers in the 20 patients with mild intestinal mucosa damage (Marsh I), but is inexplicable for the 28 patients with Marsh II and III. We may also cautiously suppose that in seronegative CD patients autoantibodies might have disappeared in adulthood, similarly to other autoimmune diseases such as type 1 diabetes.30 An additional issue may be that until 2012, the antihypertensive drug olmesartan was not recognised as a potential factor of severe villus atrophy;16 however, in our cohort of young patients, hypertension was not recorded among comorbidities except for one 47-year-old woman taking enalapril.
The existence of seronegative CD was previously reported in several studies,31–35 although its prevalence is still a matter of debate and available information on the clinical phenotype of this subset of patients with CD is currently discordant. For example, Rostami et al31 reported a high prevalence of seronegative CD in 1999. In this study, patients had mild intestinal alterations and moderate gastrointestinal symptoms. Abrams and colleagues reported a prevalence of patients negative for all CD-related serological tests in 15% of their patients with villus atrophy.32 The most striking finding of their study was that clinical features and associated disease in patients with seronegative CD were similar to those with seropositive CD and improved following a GFD.32 In contrast, in a more recent study of adult patients with seronegative CD, on the basis of negative TTG, DGP and EMA tests, positive genetic tests and histological findings consistent with a diagnosis of CD, only two patients out of eight showed an initial improvement of symptoms after a GFD.34 In our study, the majority of seronegative patients experienced a reduction of symptoms on GFD. The long-lasting effect of GFD observed in our cohort on gastrointestinal symptoms tend to exclude a mere placebo effect.13 In patients with malabsorption, duodenal biopsy is needed in order to analyse the intestinal mucosa for villus atrophy.32 Although malabsorption was not detected in the 100% of our patients with seronegative CD, all had some degree of mucosal duodenal injury and, more importantly, symptoms improvement was associated with normalisation of duodenal mucosa.
Overall, differences in clinical phenotype and genotype between patients with seronegative and seropositive CD were minimal, insufficient to draw a specific profile. However, the frequency of DRB1*02 homozygosis, which entails a more severe underlying autoimmune process, was significantly reduced in seronegative patients, a possible indication that patients with seronegative CD have a relatively milder genetic profile.
There are limitations of our study. First of all, the long follow-up period and the invasive procedures in the different steps of the study determined a high number of dropouts. Moreover, patients were seen by different physicians over a 13-year follow-up period and some loss of data cannot be ruled out. Finally, a gluten challenge test was refused by several patients and for those who agreed, we were not able to guarantee for an adequate introduction of gluten per day.
Conclusions
Our study identified a subgroup of patients with clinical and genetic features associated with histological lesions peculiar of CD and negative serology that benefits from GFD. We failed to trace a specific phenotype and/or genotype in our cohort of patients with seronegative CD compared with patients with seropositive CD. Waiting for more sensitive serological markers, small-bowel biopsy remains the ‘gold standard’ for the diagnosis of gluten intolerance in patients with malabsorption and unexplained abdominal symptoms. A strict, lifelong gluten avoidance appears the most reasonable treatment for these patients.
References
Footnotes
Contributors MPD, GMP and GR were involved in acquisition of data, analysis and interpretation of data, drafting of the manuscript, study concept and design, and critical revision of the manuscript for important intellectual content. ID contributed to acquisition of data. VV and AM carried out analysis of biopsies and critically revised the manuscript for important intellectual content.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The protocol was approved by the local ethics committee, Azienda Unità Sanitaria Locale N 1, Sassari, Italy.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.