Article Text

Abstract
Background Vitamin D deficiency has been associated or implicated with the pathophysiology of the gastrointestinal conditions inflammatory bowel disease and colorectal cancer, as well as with depression. No trials or epidemiology studies to date have investigated a link with irritable bowel syndrome (IBS). A single case report has suggested a benefit in IBS of vitamin D supplementation. We hypothesised that IBS participants with vitamin D insufficiency would benefit from repletion in terms of their IBS symptoms. We undertook a pilot trial to provide data to support a power calculation and to justify a full trial.
Methods This was a randomised, double blinded, three-arm parallel design trial of vitamin D, placebo or a combination of vitamin D and probiotics. Participants were further stratified according to whether they were vitamin D replete or insufficient. Vitamin D status was determined by blood test at baseline and exit; IBS symptoms were assessed by validated questionnaire; dietary intakes were assessed by food frequency questionnaire.
Results A significant proportion of the IBS population were vitamin D deficient, such that the replete stratum could not be adequately recruited. There was a significant association in the baseline data between circulating vitamin D level and quality of life (“How much has IBS affected your life?”). Supplementation significantly improved vitamin D level versus placebo. IBS symptoms were not significantly improved in this pilot, although a power calculation was enabled from the intervention data.
Conclusions The IBS population exhibits significant levels of vitamin D insufficiency and would benefit from screening and possible supplementation. The impact of IBS on quality of life may be reduced by vitamin D level. Future trials should have a sample size of over 97.
Trial registration number: ICTRN 6116003917.
- IRRITABLE BOWEL SYNDROME
- VITAMINS
- PROBIOTICS
- QUALITY OF LIFE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Irritable bowel syndrome (IBS) is a chronic functional gastrointestinal (GI) disorder that affects 10–15% of western populations, yet its pathogenesis and management are poorly characterised.
▸ Vitamin D supplementation has been associated with positive outcomes in other lower-GI conditions, including cancer prevention and colitis.
▸ Few studies to date have reported any relationship between vitamin D and IBS, although we recently reported a case study in this area.
What are the new findings?
▸ The IBS population exhibits low concentrations of serum 25OHD; these levels respond to supplementation.
▸ There is a significant positive association between quality of life and circulating 25OHD concentrations.
▸ We provide data on which to inform power calculations for a larger clinical trial of vitamin D supplementation in IBS patients.
How might it impact on clinical practice in the foreseeable future?
▸ The data provide evidence for widespread vitamin D insufficiency in people with IBS. There may be benefit to testing IBS patients’ vitamin D status and providing supplementation. There is a positive association between vitamin D status and quality of life measures, supporting a potential interaction between vitamin D and mental health and well-being. Clinicians may consider trialling vitamin D with patients with IBS as part of a nutritional management strategy. The results suggest a larger, adequately powered trial may be justified.
Introduction
Irritable bowel syndrome (IBS) is a chronic disorder which profoundly affects quality of life with a prevalence of 10–15% in the industrialised world.1 IBS is a relapsing condition that has a large social impact and is associated with significant direct and indirect healthcare costs.1 It is a heterogeneous disorder that can be subtyped depending on the bowel habits of patients; IBS with constipation (IBS-C), IBS with diarrhoea (IBS-D) or IBS with mixed bowel habits (IBS-M).2
IBS pathogenesis is poorly understood and it is generally regarded as a multifactorial disorder involving host and environmental factors, including diet. Most hypotheses involve altered intraluminal milieu, immune activation, enteric neuromuscular dysfunction and brain–gut axis dysregulation. It is thought that the intestinal microbiota might play an important role as bacterial infection, antibiotic use and chronic low-grade inflammation are associated with IBS onset.3 Several studies have implicated changes in the colon microbiota may be associated with IBS symptoms, including perturbation in bile acid metabolism and electrolyte absorption.4 This theory is further supported by generally beneficial effects of bacteriotherapeutic interventions (vide infra).
Therapy for IBS is primarily targeted at treating the symptoms experienced, and include loperamide for diarrhoea, methylcellulose for constipation and smooth-muscle relaxants for abdominal pain.2 Nonetheless, symptom treatment meets with limited success and may not be effective for long-term management of IBS.
Mounting data suggest that probiotics may be beneficial in the management of IBS. A recent systematic review of 35 trials investigating probiotic use in IBS showed that 25 of these studies reported a beneficial effect on the primary outcomes including global symptom severity.5 ,6 The effect on secondary outcomes varied between studies with improvements seen in flatulence and abdominal bloating following treatment with VSL#3.7 ,8 Other studies demonstrated a decrease in abdominal pain after 4 weeks of treatment with Lactobacillus plantarum 299V when compared to control.9 Our previous work has demonstrated an improvement in global symptom severity in people with IBS following 8 weeks of supplementation with LAB4 probiotic.10
We recently reported a case study of an IBS patient taking high dose (3000 IU daily) vitamin D. The participant reported remission of IBS symptoms following supplementation, with a recurrence of the symptoms on supplementation cessation. Additionally, analysis of social media (blogs/forums) reports from 37 IBS patients found that 70% described improvements in their symptoms with supplementation and the majority of these individuals reported being vitamin D deficient before supplementation.11 A role for vitamin D supplementation in gastrointestinal health is also supported by studies showing associations between vitamin D deficiency and inflammatory bowel disease (IBD).12 A recent systematic review suggested there may be benefits of vitamin D supplementation in IBD.13
On the basis of our previous case report,11 we hypothesised that patients with IBS who are vitamin D insufficient, would report improvement in symptoms following vitamin D supplementation. We further sought to test whether vitamin D supplementation in combination with a probiotic preparation would act synergistically.
There are no published randomised controlled trial of vitamin D supplementation in IBS and therefore no data on which to base a power calculation. A formal aim of this trial is to provide data to allow such calculations to be undertaken, enabling properly scaled clinical trials to be designed.
Materials and methods
Participants
Ethical approval for this study was granted by The University of Sheffield Research Ethics Committee (Ref: SMBRER278). Participants were recruited via poster advertisements at the University of Sheffield. All participants had a previous clinical diagnosis of IBS and met the Rome III criteria at baseline.14 Participants who reported any antibiotic use in the past 4 weeks prior to recruitment, recent changes in IBS medication, pregnancy, current use of vitamins or probiotic supplements, history of gastrointestinal surgery, diabetes or current use of antidepressants or antipsychotics were excluded. The study population was stratified by vitamin D status hypothesising that deficient or insufficient individuals would respond if deficiency were causal in IBS.
Patient measures
Throughout the study participants were assessed using a number of outcomes. To assess vitamin D status participants provided a blood sample from which baseline and exit 25OHD was measured in serum. Participants were given a food frequency questionnaire (FFQ) from which dietary intake was derived using FETA opensource software.i Baseline IBS symptom questionnaires were completed.15 The questionnaire assessed abdominal pain (pain severity and number of days with pain), bloating, bowel habits (minimum and maximum bowel movement per day and satisfaction with bowel habit) and quality of life over each 2-week period.
Study design
This was a 12-week double-blind, placebo-controlled, stratified study.
Participants attended the Clinical Research Facility, Royal Hallamshire Hospital, Sheffield for three visits (figure 1). At the first visit, baseline 25OHD was measured in serum, participants completed FFQ and baseline IBS symptom questionnaires were completed.15
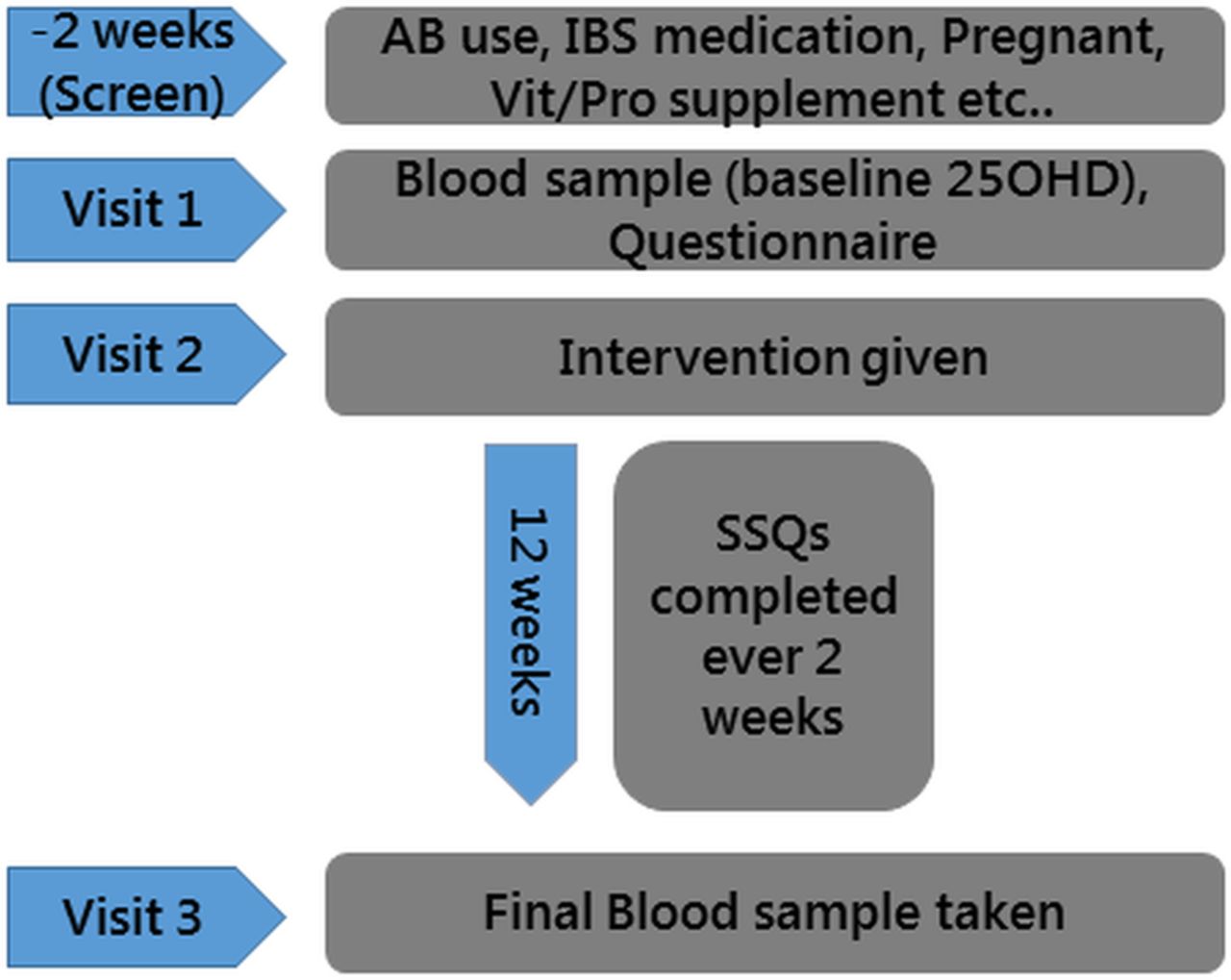
Flow diagram of study protocol. IBS, irritable bowel syndrome; SSQ, Symptom Severity Questionnaires.
The second visit took place approximately 2 weeks following visit 1. Participants were issued with a 12-week supply of supplement and were given IBS symptom questionnaires to be completed biweekly from the date of visit 2.
At the final visit participants provided a second blood sample from which serum 25OHD was measured. Of the 51 patients issued with supplements 9 failed to return questionnaires for the full period (4 in the placebo group, 3 vitamin D alone and 2 combined intervention).
Sample size and randomisation
Based on our previous study10 we aimed to recruit approximately 150 participants. By the end of the study 51 participants were recruited. Recruitment was between January 2014 and April 2014. Participants were stratified by baseline vitamin D statusii (‘Vitamin D deficient’ (25OHD <20 ng/mL) and ‘Vitamin D replete’ (25OHD >20 ng/mL)) and randomised. Participants were randomised to receive either double placebo (n=17), vitamin D supplementation and probiotic placebo (n=16) or probiotic and vitamin D supplementation (n=18). Participants were allocated in a 1:1:1 ratio to the three arms of the study according to a computer-generated random sequence using block randomisation with a block-size of six. The randomisation was performed by an independent statistician. Participants were enrolled and assigned sequentially to placebo or active products. The allocation sequence was not available to any member of the research team until databases had been completed and locked.
Intervention
The probiotic, vitamin D3 and corresponding placebos were provided by Cultech Ltd, Port Talbot, UK. Vitamin D3 and the corresponding placebo were provided as 15 mL liquid sublingual sprays. Both contained identical buffers with placebo lacking the active vitamin D3. Each spray of vitamin D3 gave a dose containing 3000 IU vitamin D3.
The probiotic preparation contained two strains of Lactobacillus acidophilus, CUL60 (NCIMB 30157), CUL21 (NCIMB 30156), Bifidobacterium bifidum CUL20 (NCIMB 30153) and Bifidobacterium animalis subsp. lactis CUL34 (NCIMB 30172) at a total of 2.5×1010 colony forming units (cfu) per capsule. Volunteers were instructed to ingest one capsule per day with water and one spray orally per day for 12 weeks. Compliance was assessed by counting the number of capsules remaining and weighing sprays at the end of the intervention—98% compliance was achieved.
Adverse events
There were no adverse events. One participant on the placebo arm reported feeling unwell after starting the trial with acute indigestion, heartburn and pain in the back which subsided after 2 weeks. The participant halted supplements for 4 weeks and then returned to the study under the initial time frame.
Biochemical assay
Serum 25OHD was measured using the Cobas e411 automated immunoassay from Roche Diagnostics (Germany). The inter assay coefficient of variation (CV) was 4.6%.
Statistical analysis
Number of days with pain were expressed as a percentage of each 14-day period. All other variables were assessed using a visual analogue scale and scored of 100. Individual scores were then combined to give a total symptom severity score of 500.15 χ2 Test was used to assess the distribution of participants by vitamin D stratification. Associations between baseline 25OHD stratification (deficient: <12.5 ng/mL; insufficient: 12.5–20 ng/mL; replete 20–50 ng/mL; toxic: >50 ng/mL, no recordings were made at or near the toxic range) and baseline symptom scores, follow-up 25OHD and change in symptom score were determined by analysis of variance(ANOVA) with Bonferroni correction. Pearson's correlations for vitamin D intake and baseline serum 25OHD were undertaken. Change in symptom score over 7 time points were analysed by repeated measures ANOVA, missing data were not imputed and were assumed to be missing at random in the ANOVA model. Comparisons of deficient and replete symptom scores were assessed by independent t tests. All tests were two sided with a significance value of <0.05. Analysis was carried out using SPSS V.22 (IBM, Armonk, New York, USA).
Results
Baseline vitamin D status shows a significant association with quality of life
Demographics of the population are shown in table 1. The three arms were similar in terms of number, gender, age, IBS subtype and serum 25OHD. Overall IBS symptom severity at baseline (week -2) was similar between groups (243±67 placebo, 244±92 vitamin D and 237±67 vitamin D with probiotic, p=0.241) and between IBS subtype (figure 2A) as was the baseline serum 25OHD (15±8.4, 16±8.0, 14±8.3 ng/mL, p=0.295).
Baseline characteristics of participants
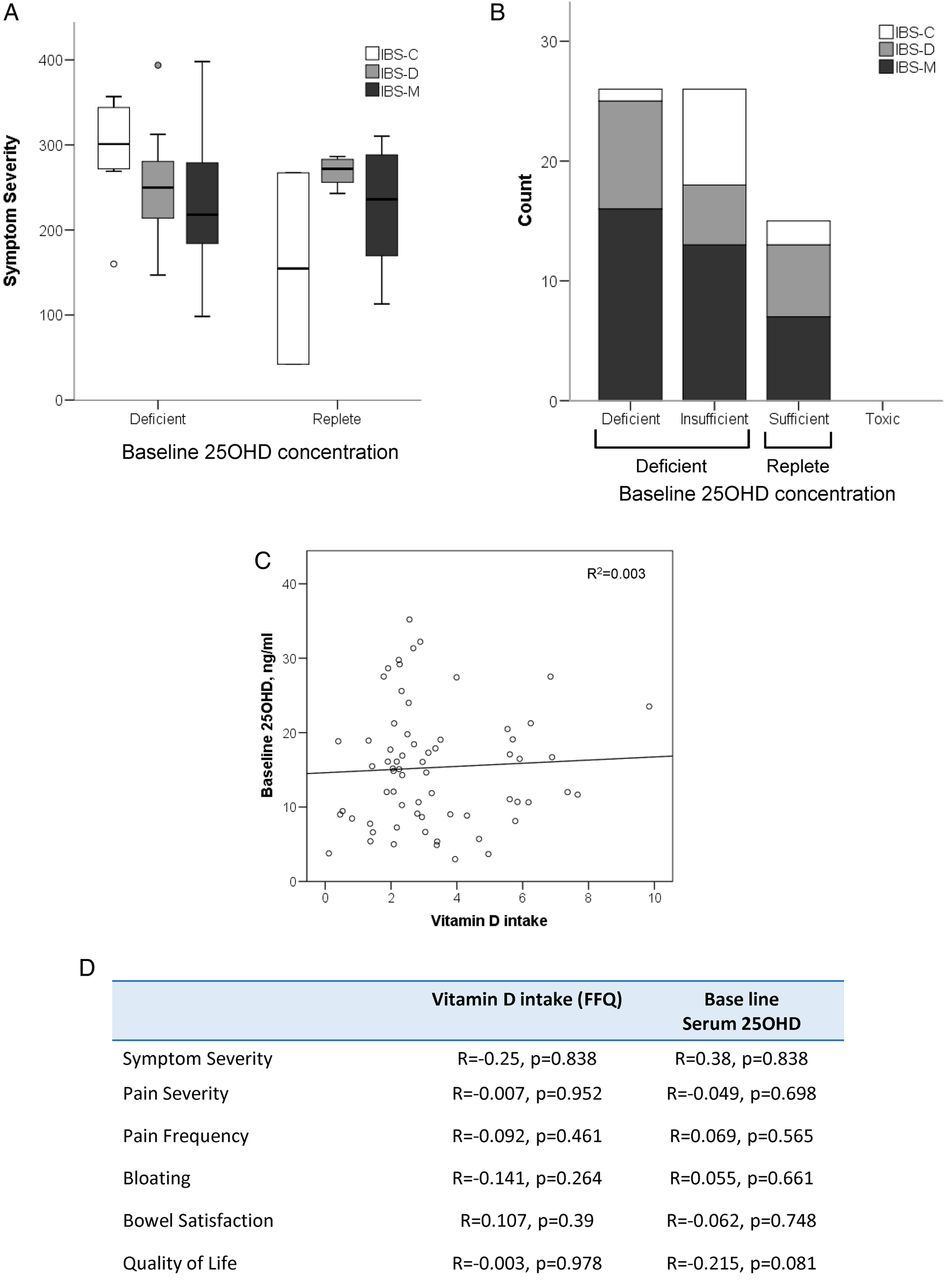
Baseline characteristics of participants (A). Distribution of IBS-subtype across serum 25OHD levels at baseline shows no significant association of IBS subtype with vitamin D status (B). Mean score for symptom severity at baseline in IBS-C, D and M participants stratified by vitamin D status at baseline (C). Correlation of baseline 25OHD with vitamin D intake (D). Table summarising IBS symptom score with vitamin D intake and baseline serum 25OHD. No correlations were detected with in response to vitamin D intake, however, serum 25OHD showed a negative correlation between quality of life and serum 25OHD. IBS, irritable bowel syndrome; FFQ, food frequency questionnaire.
The majority of participants had baseline 25OHD levels that are considered insufficient/severely deficient16 with an overall sample mean 25OHD of 15.3±7.9 ng/mL and 81.8% of IBS-C (n=7), 70% of IBS-D (n=9) and 81.6% of IBS-M (n=24) with <20 ng/mL circulating 25OHD levels. This level of deficiency was similar to that seen in a BMI-matched cohort in Sheffield at this time of year (S. Bowles personal communication, 2014). There was no association between IBS-subtype and 25OHD status at baseline (figure 2B). However, participants with low 25OHD at baseline reported a greater impact on quality of life (on the basis of the IBS questionnaire) than their replete counterparts (p=0.034) (table 2). There was no difference in other symptom scores between 25OHD deficient and replete individuals (table 2). Data exploration suggested, a trend for lower affected quality of life scores in each IBS subtype in vitamin D replete participants against the non-replete cohort (see online supplementary, figure S1c).
supplementary data
Baseline symptoms by vitamin D status*
We sought to determine whether potential benefits of replete vitamin D status may be attributed to associations between systemic effects of 25OHD or the potential mucosal action of ingested dietary vitamin D. There was no association between vitamin D intake and symptom severity, suggesting the effect may be systemically mediated (figure 2C, D).
Effect of vitamin D intervention
The distribution of participants by vitamin D status in each treatment arm was compared at baseline and exit. An equal distribution was seen at baseline (table 3) and the distribution was altered by 12 weeks of vitamin D supplementation. Of participants receiving supplementation in combination or alone the percentage of participants who were replete improved from 22.2% and 25.0% to 87.5% and 92.3%, respectively. Participants on placebo also had higher 25OHD levels with 60% of participants replete at exit compared to only 18.5% at baseline (figure 3A).
Vitamin D status at baseline and exit

{kind=link}
{kind=link}
{kind=link}
Effect of intervention on participant serum 25OHD concentration and total symptom severity (A). Box plot serum 25OHD concentrations (ng/mL) before and after intervention with placebo, vitamin D3 or vitamin D3+Probiotic (all participants), a significantly greater increase with vitamin D supplementation alone or with probiotic was seen over placebo group (B). Repeated measure of total symptom severity against time point (all participants) (C). Box plot serum 25OHD concentrations (ng/mL) before and after intervention with placebo, vitamin D3 or vitamin D3+Probiotic. (deplete participants only), a significant increase in serum 25OHD was seen in all groups with a greater response associated with vitamin D supplementation alone or with probiotic when compared to placebo group (D). Repeated measure of total symptom severity against time point (deplete participants only).
Participants who received vitamin D alone or in combination with probiotic had significantly higher 25OHD at follow-up compared to baseline (15.8±8.0 to 37.2±9.3 ng/mL and 14.9±8.4 to 37.1±11.7 ng/mL, respectively, p<0.001). These two groups also had higher levels of 25OHD compared to the placebo group at exit with mean 25OHD levels of 37 ng/mL while the placebo group mean was 25.3±8.0 ng/mL (p=0.008 vitamin D, p=0.005 vitamin D+Probiotic, respectively) (figure 3A). While it appeared that there were improved scores in all reported symptoms from baseline to exit irrespective of the intervention arm, this was not statistically significant for any symptom tested. Additionally, treatment arm did not interact with any of the symptom scores at any of the time point (figure 3B and online supplementary figure S2). The analysis was repeated limited to participants who were deficient at baseline. A significant increase was seen between baseline and exit 25OHD in all arms (figure 3C) with no significant relationship of intervention arm on total symptom severity (figure 3D) or individual IBS scores (data not shown).
Discussion
We have presented evidence of high-vitamin D insufficiency in a population with IBS, We have previously reported anecdotal evidence suggesting a benefit of vitamin D in management of IBS.11 Baseline data from our population would support a need for monitoring vitamin D status and suggests that the impact of vitamin D deficiency is most acute on perceived quality of life.
A correlation indicated a potential relationship between 25OHD and quality of life scores; however, this did not reach significance. Reported quality of life will be influenced by the depression status of participants, a common comorbidity in IBS.17 Numerous studies have reported that vitamin D levels are correlated with depression. In one such study vitamin D deficiency in young healthy individuals predicted clinical depression across a 4-week period, noting that as vitamin D levels increased due to seasonal difference in sunlight exposure volunteers showed lower levels of depression.18 A similar pattern was seen in patients suffering post-stroke depression: lower serum vitamin D correlated with depression.19 The exact mechanism through which vitamin D improves depression is not fully understood. However, vitamin D status has been implicated in neurological development,14 the vitamin D receptor (VDR) is expressed throughout the nervous system where its activation is linked to neurotransmitter levels and serotonin synthesis.20 Additionally binding of 25OHD-VDR complex results in expression of 1-α-hydroxylase which converts 25OHD to 1,25-dihydroxyvitamin D.21 This 25OHD metabolite has been shown to upregulate neurotrophins which in turn promote survival and differentiation of nerve cells.22 VDR is also expressed in the gut and regulates epithelial barrier function and bowel inflammation23 suggesting that a vitamin D deficient diet may directly impact bowel function and hence IBS symptomology. Our attempt to distinguish the effects of circulating and ingested vitamin D did not support either model, likely due to underpowering.
Supplementation with vitamin D increased serum 25OHD concentrations from baseline with a significantly greater improvement seen compared to participants receiving placebo. Nonetheless the group receiving placebo showed an improvement in 25OHD levels. This may have prevented us from detecting a significant difference in symptom scores between the placebo and supplemented groups at exit. This general increase in serum 25OHD across intervention arms was likely due to seasonal differences in sun exposure. It has been found in previous studies that the percentage of individuals in the UK deficient for vitamin D ranges from 30–40% (January–March) to 2–13% (July–September).16 Study participants were recruited in the early months of 2014 (January–April) with most follow-up visits taking place from May to August, most likely explaining the rise in 25OHD in all groups.
An exploratory analysis of participants by IBS subtype showed that there was a marked improvement in response to vitamin D supplementation across nearly all IBS symptoms in participants with IBS-C (see online supplementary figure S3). Interestingly the proportion of these participants that were considered severely deficient was low in comparison to the other IBS subtypes (figure 2B). A clear limitation is the very small numbers in groups when the data is split but the observation suggests a future study into vitamin D supplementation in this subgroup may be justified.
Throughout this study we failed to observe a significant interaction with intervention with either vitamin D alone or in combination with probiotic. This is likely explained by a number of limitations in the study. First, we observed an effect of the placebo on symptom scores: IBS symptoms have a highly variable course (compare week-2 and 0 in figures 3B, D for example). It is recommended that active intervention in IBS last a minimum of 4 weeks and potentially up to 6 months for long-term analysis.24 Furthermore, as a pilot study the current trial is inherently underpowered. In order to detect a statistically significant response in total symptom severity scores we would need larger sample sizes. With the data generated in this study it was calculated that a sample size of 74 per arm would be needed. This was calculated based on change in total symptom severity at exit with a placebo mean of −16, a mean of −54 for vitamin D intervention, a combined SD of 82 and assuming a desired power of 80% with an α error of 0.05.
It is possible that seasonal variations in vitamin D levels may impact IBS in the current study. Our data show a general improvement in symptom score and improved 25OHD over the duration of this study is tempting to speculate that increased sunlight exposure increases vitamin D levels which in turn improved IBS symptoms. Such effects have been previously shown for IBS and IBD symptoms.25 ,26 However, there was a significantly greater effect of vitamin D intervention than placebo on circulating vitamin D. Taken together, these data suggestion that seasonal variation should also be taken into account in the design of trials to assess the potential application of vitamin D in IBS.
In summary we have shown that IBS sufferers deficient in vitamin D experience poorer quality of lives than their replete counterparts. Our data demonstrate the need for additional studies of more than 8 weeks in duration with recruitment of a larger cohort of IBS patients.
Acknowledgments
The authors thank the staff at Sheffield Clinical Research Facility for support phlebotomy and use of their research environment; Ms Fatma Gossiel undertook clinical biochemical assays for vitamin D; Ms Dolappo Owoeye and Ms Farhana ab Hadi entered diet data.
References
Footnotes
Contributors ST completed exit analyses, entered all data, undertook all statistical analyses, wrote the first draft of the paper. NR and ART recruited and consented participants and undertook day-to-day running of the trial in its inception and initial phases and reviewed drafts of the paper. ALE contributed to exit analyses, undertook first-pass data analysis and reviewed drafts of the paper. VAG co-conceived the study and undertook qualitative exit interviews with participants and reviewed drafts of the paper. IG; SFP co-designed the study, advised on dosing and delivery of probiotics and vitamin D, contributed to the analysis and interpretation of the data and reviewed drafts of the paper. EAW co-designed the study and contributed to its direction, supervised and interpreted the nutritional analyses and reviewed drafts of the paper. BMC conceived the study, assumes overall responsibility for the project, is its chief investigator, finalised each draft of the manuscript and produced the final version.
Funding This work was funded by Cultech Ltd.
Competing interests IG and SFP are employees of Cultech Ltd, a manufacturer of supplements and probiotics.
Patient consent Obtained.
Ethics approval University of Sheffield.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
↵ii https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/