Article Text

Abstract
Objective Clostridium difficile is a major cause of nosocomial infectious diarrhoea. Treatment of C. difficile infection (CDI) depends on disease severity. A combination of vancomycin and metronidazole is often recommended in severe cases. The aim of this study was to examine, in a murine model of CDI, if mice treated with a combination of vancomycin and metronidazole had a better clinical outcome than mice treated with vancomycin or metronidazole alone.
Design C57BL/6J mice pretreated with an antimicrobial mixture were challenged with C. difficile VPI 10463 or phosphate-buffered saline by oral gavage. After the challenge, the mice were treated with placebo, vancomycin, metronidazole or a combination of vancomycin and metronidazole for 10 days. The mice were monitored for 20 days with weight and a clinical score. Stool samples were examined for C. difficile spore load and presence of C. difficile toxins.
Results None of the mice in the vancomycin-treated group died during the treatment phase compared to a mortality of 17%, 33% and 55% in the combination, metronidazole and infected control group, respectively. Mice treated with vancomycin alone or in combination with metronidazole recovered from CDI faster than mice treated with metronidazole alone. However, after discontinuation of treatment, vancomycin-treated and combination-treated mice succumbed to clinical and bacteriological relapse.
Conclusions Mice treated with vancomycin alone had a better clinical outcome in the treatment phase of CDI than mice treated with metronidazole alone. A combination of vancomycin and metronidazole did not improve the clinical outcome when compared to treatment with vancomycin alone.
Trial registration number The trial registration number from the Danish Experimental Animal Inspectorate is J number 2012-15-2934-00422.
- BACTERIAL INFECTION
- ANTIBIOTIC THERAPY
- COLONIC DISEASES
- COLONIC BACTERIA
- INFECTIOUS DIARRHOEA
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Clostridium difficile is the major cause of nosocomial infectious diarrhoea.
▸ The main antimicrobial agents for treatment of C. difficile infection (CDI) are metronidazole and vancomycin.
▸ A combination of vancomycin and metronidazole is often used in the treatment of severe, complicated CDI.
What are the new findings?
▸ Vancomycin is more effective than metronidazole in the treatment of a first episode of CDI in mice.
▸ A combination of vancomycin and metronidazole is less effective than vancomycin alone in the treatment of a first episode of CDI in mice.
▸ Vancomycin treatment is associated with relapse of CDI in mice.
How might it impact on clinical practice in the foreseeable future?
▸ If our findings could be reproduced in a clinical setting, this new knowledge could lead to a reduction in the use of a combination of vancomycin and metronidazole for the treatment of severe CDI in humans.
Introduction
Clostridium difficile is the major cause of nosocomial infectious diarrhoea.1 Treatment of C. difficile infection (CDI) is complicated and depends on several factors including disease severity. The main antimicrobial agents for treatment of CDI are metronidazole and vancomycin. Metronidazole has long been the first-line agent in treating CDI, as two randomised trials conducted in the 1980s and 1990s demonstrated equal efficacy of metronidazole and vancomycin in the treatment of CDI.2 ,3 Furthermore, metronidazole has a lower cost than vancomycin and a presumed lower potential for selection of vancomycin-resistant enterococci.4 However, a decreased response to metronidazole treatment of CDI has been reported,5–7 and a prospective, randomised study, stratified on disease severity, found vancomycin to be superior to metronidazole in treating severe CDI.8 Hence, the current guidelines for antimicrobial treatment of a first episode of CDI generally recommend metronidazole for treatment of mild to moderate or non-severe CDI and vancomycin for treatment of severe CDI.9 ,10 Despite the relevant treatment of a first episode of CDI with these agents, recurrence is common and occurs in up to 25% of cases.9 ,11 This has led to the introduction of new antimicrobial agents in the treatment of CDI, such as fidaxomicin,12 ,13 teicoplanin,14 rifaximin,15 tigecycline16 ,17 and nitazoxanide,18 ,19 but experience with these agents is still limited and only fidaxomicin has a licensed indication for the treatment of CDI.
In severe cases of CDI, a combination of oral metronidazole and oral vancomycin is sometimes recommended. This combination, given as intravenous metronidazole and oral vancomycin, or vancomycin retention enema, is also recommended in general guidelines for treating severe and complicated CDI.9 ,10 ,20 However, there is no evidence to support a combination of vancomycin and metronidazole.21–25 In fact, in a retrospective cohort study, it was noted that patients treated at once with a combination of metronidazole and vancomycin did worse than their counterparts treated with either drug by itself.22
Antimicrobial therapy is one of the most dominant risk factors for CDI, and treatment of CDI with metronidazole and vancomycin in combination may further disrupt the already abnormal intestinal flora. Hence, it is highly important to ensure only the necessary antimicrobial therapy for CDI. Therefore, using a murine model of CDI, we compared the effects of vancomycin and metronidazole alone and in combination in treated mice versus controls, with respect to clinical disease (weight and survival) and microbiological outcome (faecal C. difficile spore load and presence of C. difficile toxin). Furthermore, we evaluated the colonic pathology and inflammation with a histological score and myeloperoxidase (MPO), respectively.
Materials and methods
Murine model and ethics statement
The model used in this study was based on the model developed by Chen et al.26 Figure 1 illustrates the experimental scheme. The course of infection in C. difficile-infected mice can be divided into two phases: the treatment phase, with an acute course of disease within the first 3 days after challenge, and the post-treatment phase, in which some mice developed relapse of CDI. The Danish Experimental Animal Inspectorate approved the experimental protocol for this study (J number 2012-15-2934-00422). All applicable national guidelines for the care and use of animals were followed. Animals with a weight loss above 20% or judged to be in a moribund state based on a clinical score were euthanised (see online supplementary material).
supplementary data
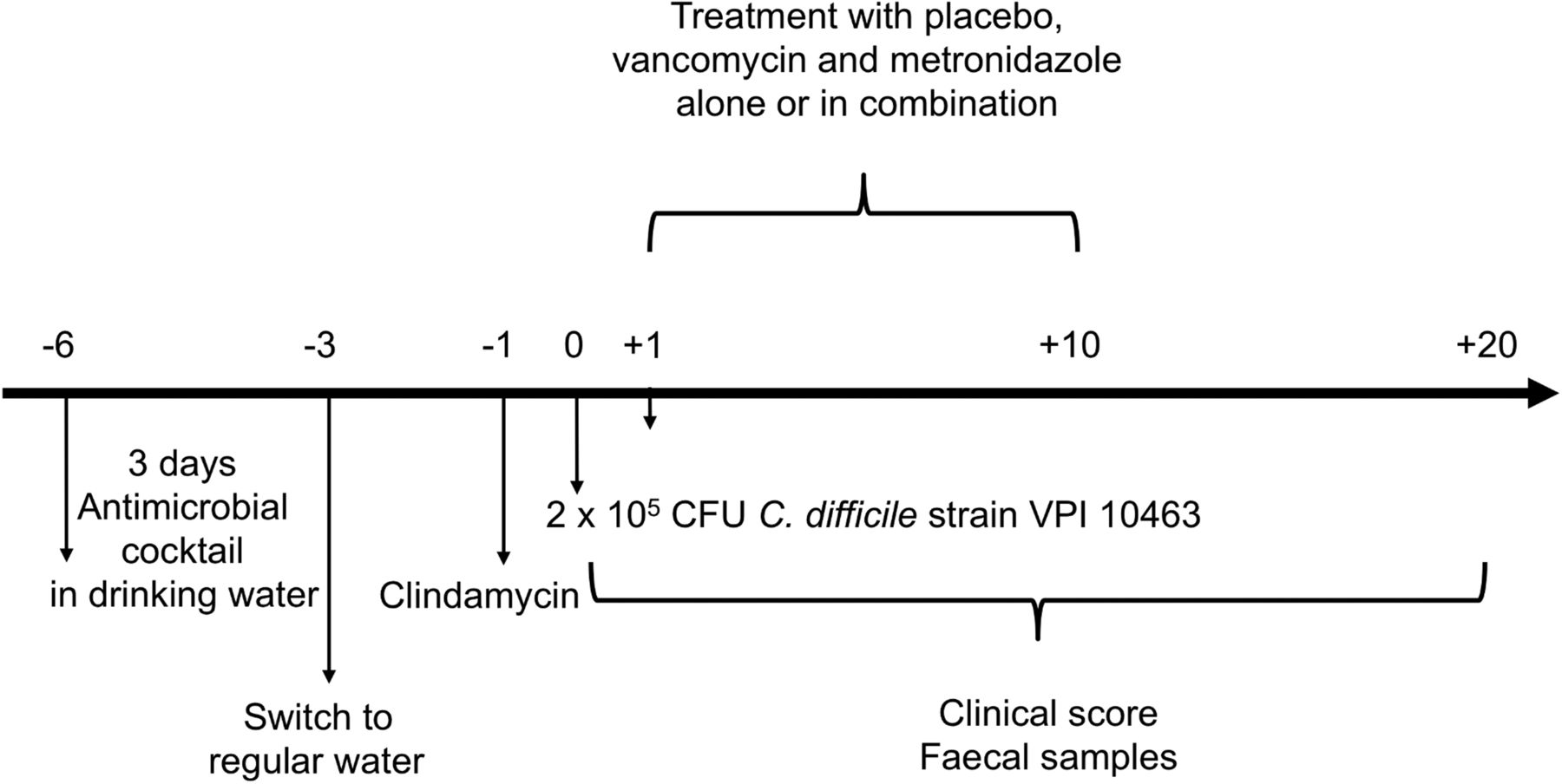
Experimental scheme of this study with key events marked on the timeline.
C. difficile strain and growth conditions
Infection of mice was performed with C. difficile VPI 10463 (ATCC 43255). This strain produces both C. difficile toxins, A and B, but not the binary toxin. The strain was stored in preservation broth (infusion broth with 10% glycerol) at −80°C and subcultured on 5% blood agar plates in an anaerobic atmosphere (10% H2, 10% CO2, 80% N2) at 37°C for 24 h. For C. difficile challenge a suspension of C. difficile was freshly prepared and bacterial enumeration was performed at the time of challenge to ensure that the correct dose of C. difficile cells was administered.
Antimicrobial agents
All antimicrobial agents were purchased from Sigma-Aldrich (Sigma-Aldrich, St Louis, Missouri, USA). Stock solutions of all antimicrobial agents were prepared in sterile water and stored at −80°C. The minimal inhibitory concentration (MIC) of vancomycin and metronidazole for VPI 10463 was determined using the broth microdilution method as described by the Clinical and Laboratory Standards Institute (CLSI).27
Animals and housing
Female C57BL/6J mice were obtained from M&B Taconic (Taconic Europe, Ry, Denmark). The mice were 6–8 weeks old, with an initial bodyweight of approximately 18–19 g. The mice were housed in groups of 3–4 in individually ventilated cages (Techniplast, Buguggiate, Varese, Italy) with a 12 h light/12 h dark schedule, and fed autoclaved standard chow (Altromin #1324, Lage, Germany) and water ad libitum throughout the experiment. The mice were given nesting material, shredded paper strips and wooden squares as environmental enrichment. The bedding in the cages was changed every day during the acute phase of CDI and relapse, and every second day during the rest of the experiment, in order to diminish the risk of cross-contamination. Two mice from the uninfected control group were excluded. One because it had C. difficile in faecal samples prior to the C. difficile challenge, and the other because it got hurt trying to escape from the cage.
Antimicrobial administration and infection with C. difficile
The mice were divided into five groups: an uninfected (n=7) and infected (n=9) control group treated with placebo (sterile water) and three infected groups treated with either vancomycin (n=6, 50 mg/kg/day), metronidazole (n=6, 50 mg/kg/day), or vancomycin and metronidazole in combination (n=6, 50+50 mg/kg/day), for 10 days. The group treated with vancomycin and metronidazole in combination will further on be referred to as the combination group. In order to establish CDI, the normal enteric flora was disrupted by pretreating the mice with an antimicrobial mixture containing kanamycin (40 mg/kg), gentamycin (3.5 mg/kg), colistin (4.2 mg/kg), metronidazole (21.5 mg/kg) and vancomycin (4.5 mg/kg). The concentration of the antimicrobial mixture was calculated based on the average weight of the mice and their expected water consumption. The antimicrobial mixture was administered for 3 days in the drinking water (figure 1). On day 3, the mice were switched back to regular drinking water. One day prior to infection, the mice received a single dose of clindamycin (10 mg/kg) intraperitoneal. On day 0, the mice were challenged with approximately 2×105 colony-forming units (CFU) C. difficile by oral gavage. The uninfected control group received phosphate-buffered saline (PBS). From 1 day post-infection, the mice were treated with placebo, vancomycin, metronidazole and the combination, for 10 days (figure 1). All antimicrobial agents and placebo were given by oral gavage. The mice were followed for a total of 20 days. A clinical scoring system based on weight loss, activity level and appearance of eyes and fur was used daily. Faecal samples were collected from each mouse at various time points throughout the experiment and immediately stored at −80°C. At the end of the 20-day observation period, the surviving mice were euthanised.
C. difficile spore load in faecal samples
Faecal samples were thawed, dissolved and incubated in 0.5 mL 70% alcohol. After 1 h, the samples were 10-fold diluted and plated on cycloserine-cefoxitin fructose agar. After incubation in an anaerobic atmosphere for 48 h, the colonies were counted. The detection limit was 100 CFU/g of faeces. To confirm C. difficile (VPI 10463), isolates were examined with PCR for toxin genes and in-frame deletions in tcdC (negative toxin regulator).28
Faecal cytotoxicity
Faecal cytotoxicity of toxin A and B was measured with a cell cytotoxicity assay.29 ,30 Each faecal sample was weighed and dissolved in PBS containing protease inhibitor (Roche Diagnostica, Mannheim, Germany). The amount of diluent per sample was normalised to provide the same stool mass-to-diluent ratio. Samples were vortexed and centrifuged at 3000 rpm (SX4750A in Allegra X-15R) for 10 min. Supernatants were filtered through a 0.22 μm membrane (Merck Millipore, Darmstadt, Germany) and stored at −80°C. To measure toxin-mediated cytotoxicity, filtrates were 10-fold diluted in PBS and added in duplicate to a confluent monolayer of Vero cells (CCL-81; American Type Culture Collection), grown in Dulbecco’s Modified Eagle Medium (DMEM) with 10% fetal bovine serum and gentamicin (0.1 mg/mL), and prepared in 96-well flat bottom microtitre plates (7.5×103 cells per well). These plates were incubated in a humidified incubator with 5% CO2 at 37°C. The cytotoxic effect of the filtrates was determined after 24 h by measuring cell rounding under a phase-contrast microscope. Toxin titres were defined as the highest dilution to cause 100% cell rounding. A control well for each sample was included, containing both the antitoxin and sample (TechLabs, Blacksburg, Virginia, USA).
Necropsy, histopathological analysis and MPO
The mice were euthanised by cervical dislocation. Caecum and the proximal 2/3 of colon were placed directly in liquid nitrogen and stored at −80°C. The remaining 1/3 of colonic tissue was fixed in neutral 10% buffered formalin and stored at room temperature until placed in 10% ethanol. Samples were coded and randomised. Tissue from each mouse was placed in separate tissue cassettes, then processed and paraffin embedded. Slides with two levels of sections from each paraffin block were routine-stained with H&E. The histological severity of enteritis was graded using a scoring system reported previously26 ,31 ,32 and adapted by Reeves et al.33 It was used to determine epithelial damage (score 0–4), oedema (score 0–4) and cellular infiltration (score 0–4), and assigned a total score between 0 and 12. An experienced histopathologist, blinded to treatment, evaluated all slides and all tissue on slides.
Colonic tissue from the proximal part of the colon adjacent to the caecum was used for examination of the presence of MPO. Tissue was homogenised with a tissuelyser II (Qiagen, Venlo, Limburg, The Netherlands). Samples were diluted (in a range from 1:4, 1:10, 1:20, 1:30, 1:60 to 1:100) and MPO levels in colonic tissue were tested in duplicate with a mouse MPO ELISA-kit (Hycolt Biotech, Uden, The Netherlands).
Statistical analysis
Results were analysed using STATA/IC 13 (Statacorp, College Station, Texas, USA). Results are presented as dot plots or mean values. For normally distributed data mean values are expressed as mean ±SE of mean (SEM). Differences between experimental groups at a given time point were analysed with one-way analysis of variance. Differences between two groups at a given time point were analysed with Student t test or Mann-Whitney U test. Mortality between the different treatment groups was compared with the log-rank test for equality of survivor functions and presented as Kaplan-Meier survival curves.
Results
Treatment phase of CDI in mice
After the C. difficile challenge, the infected mice showed signs of clinical illness with weight loss, hunched posture, loose stools or diarrhoea. Some mice developed severe illness and were euthanised. At day 10, we found a significantly higher survival in the uninfected control group compared with the infected control group (the log-rank test, p=0.023). The vancomycin and combination-treated mice were clinically least affected in the treatment phase of CDI. None of the mice in the vancomycin-treated group died during their treatment for CDI compared to a mortality of 17%, 33% and 55% at day 10 in the combination, metronidazole and infected control group, respectively (figure 2 and table 1).
Per cent survival in each group tabulated at days 2, 3, 4 and 20 post-infection

Kaplan–Meier survival plots for the uninfected control and the four groups challenged with Clostridium difficile VPI 10463 on day 0. Treatment or placebo was given from day 1 to day 10.
The only treatment group with significantly better survival than the infected control was the vancomycin group (p=0.034); however, there was only a tendency towards better survival in the vancomycin group when compared to the metronidazole group (p=0.138).
Figure 3 illustrates the mean relative weight for all the surviving mice (until time of death) in the five groups. Infected mice showed maximum weight loss at days 2–3, and all the infected groups had significant weight loss at days 2–3 when compared to the uninfected control (Student t test, infected control: p<0.001, mean difference: 20.88%, SEM: ±2.66; vancomycin: p=0.024, 10.82% ±3.77; metronidazole: p=0.004; 16.49% ±3.85; combination: p<0.001, 11.0% ±1.07) (figure 3). The metronidazole group had the most pronounced weight loss; however, there was no significant difference in weight loss between the three treatment groups on days 2–3. After days 3 and 4, the surviving mice began to gain weight. Mice in the vancomycin, infected control and combination groups returned to normal weight by days 5–8. However, mice in the metronidazole group did not return to their normal weight until approximately day 16. In the treatment phase, from day 4 and through 10, we found significantly lower mean relative weights in the metronidazole group than in the vancomycin group (p=0.004). We found no significant difference between the relative weights in the vancomycin and the combination group (p=0.584).

Mean relative weight (%) for all the surviving mice until time of death in the five groups. Treatment or placebo was given from day 1 to day 10.
Post-treatment phase of CDI—relapse
All the infected mice that survived the acute phase of CDI regained their normal weight at approximately the end of the first week except for the mice in the metronidazole group, which displayed a slow clinical recovery with respect to the mean relative weight (figure 3). However, five of six mice in the vancomycin-treated group and five of five mice in the combination group developed clinical symptoms of CDI, with weight loss and diarrhoea at around day 15, 5 days after the treatment was discontinued. The mean relative weight of the two groups treated with vancomycin was significantly lower than that of the surviving mice in the infected control group at day 16 (vancomycin: p=0.009; combination: p=0.018) and the metronidazole group at day 16 (vancomycin: p=0.024; combination: p=0.055, border significant). Three mice in the vancomycin group and one mouse in the combination group died during relapse (figure 2). None of the mice in the vancomycin-treated group died during the acute CDI, but after relapse there was a mortality of 50% in this group and, when compared to the infected control group at day 20 post-infection with the log-rank test, there was no longer a significant difference between the two groups (p=0.42). No additional deaths occurred in the infected control or metronidazole groups after the treatment was discontinued; furthermore, they did not have any clinical symptoms of CDI.
Presence of C. difficile spores and toxins in faecal samples
To determine if the clinical symptoms of CDI were associated with increased C. difficile presence, faecal samples were examined. Figure 4 shows the amount of C. difficile spores from all the surviving mice (until time of death) in the four infected groups. In the acute course of CDI, there was a high amount of C. difficile spores among all infected groups. However, at day 2 post C. difficile challenge, the spore load in the vancomycin-treated group was significantly lower when compared to the infected control group (p=0.018). At day 3 post-infection, all treated groups had significantly lower spore counts when compared to the infected control (vancomycin: p=0.008, metronidazole: p=0.046 and combination: p=0.011). At the acute course of CDI, there was no significant difference between the three treatment groups (day 1: p=0.536, day 2: p=0.185). However, the groups treated with vancomycin and the combination showed almost undetectable to completely undetectable spore counts from day 6 through day 13, whereas the metronidazole group demonstrated spore counts well above the detection limit throughout the 20-day observation period. Hence, when the mean spore load from day 6 through day 13 (after the acute course of CDI and before relapse) was calculated for each mouse, and in comparison between the three treatment groups, we found a higher spore load in the metronidazole group compared to the vancomycin (p=0.006) and combination (p=0.011) groups, respectively. However, after relapse in the vancomycin and combination groups, the mean spore load in both groups increased, and the mean spore load from each mouse from day 16 through 20 was higher when compared to the metronidazole group (vancomycin: p=0.031 and combination: p=0.046).

Mean Clostridium difficile spore load and toxin titre for all the surviving mice until time of death in the four infected groups. Black bars represent the mean log10 C. difficile spores as colony forming units (CFU) per gram faeces and light grey bars represent the mean log10 C. difficile toxin titre. The dashed lines represent the detection limits.
The faecal samples collected were also examined for the presence of C. difficile toxins. The toxin titres for all surviving mice in the four infected groups are illustrated in figure 4. The peak toxin titres were found on days 1–3, which corresponds with the weight loss of the mice and the spore load. At day 3 post-infection, all of the treated groups had significantly lower toxin titres when compared to the infected control group (vancomycin: p=0.008, metronidazole: p=0.030 and combination: p=0.009). Furthermore, when the mean toxin titre from day 6 through day 13 was calculated for each mouse, and in comparison between the three treatment groups, we found a higher toxin titre in the metronidazole group compared to the vancomycin (p=0.009) and combination (p=0.023) groups, respectively. There was a very strong positive association between the C. difficile spore load and the toxin titres (p<0.001; R2=0.83).
Histopathological changes and MPO level in colonic tissue
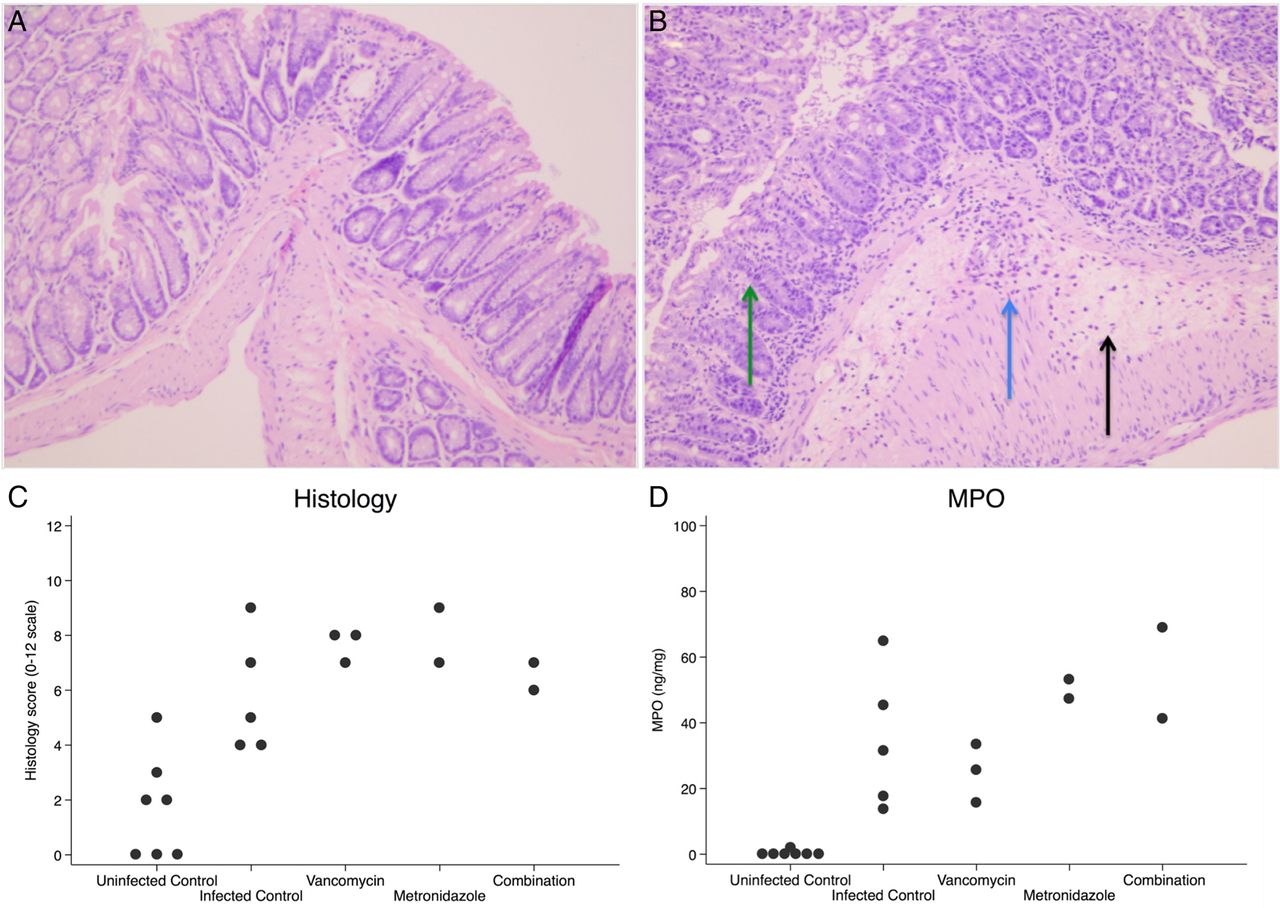
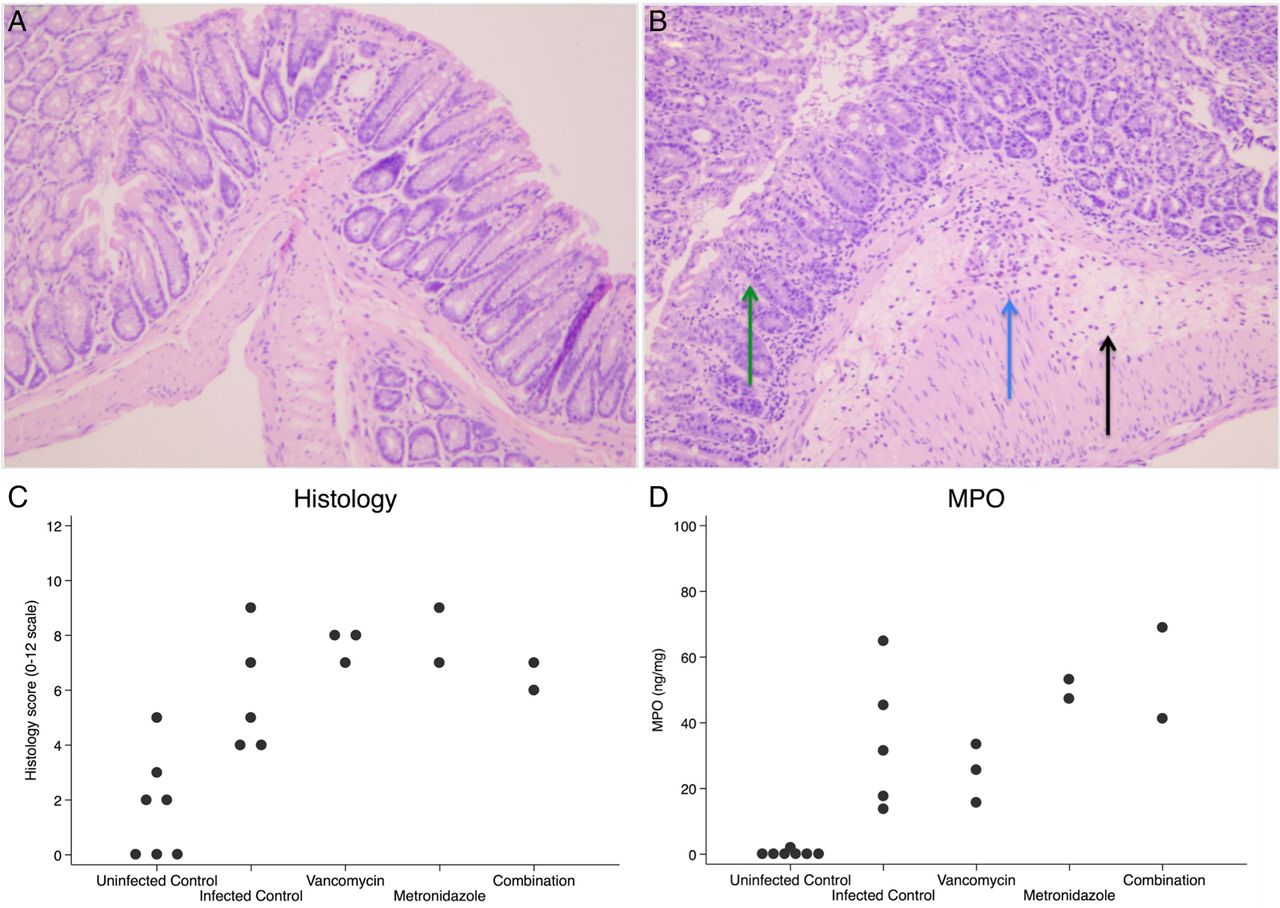
To confirm that all the mice that died from CDI also had evidence of colonic infection characteristic of CDI, we examined colonic tissue for histopathological changes (figure 5). In all the infected mice that died from CDI and the uninfected control we found a median histological score of 7 (range: 4–9) and 2 (range: 0–5), respectively. When compared to the uninfected control group, all infected groups had a significantly higher score (p<0.05) (figure 5C). To assess the neutrophil infiltration of the gut, we examined the MPO levels. For all the infected mice that died from CDI and the uninfected control mice, we found a mean MPO level of 1906 ng/mL (SEM: ±267) and 32 ng/mL (SEM: ±4.8), respectively. When compared to the uninfected control group, all infected groups had a significantly higher MPO level (p<0.05) (figure 5D). These results support the notion that the mice died from an infection characteristic of CDI. However, they do not allow us to determine the severity of infection between the different treatment groups, as the mice did not die on the same time during the course of infection.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Colonic pathology. The top panels showing representative H&E-stained slides (×200) of (A) normal colonic tissue and (B) colonic tissue from a mouse that died from Clostridium difficile infection (CDI), illustrating epithelial damage (green/left arrow), cellular infiltration (blue/middle arrow) and oedema (black/right arrow). (C) The histology score of infected mice that died from CDI in each of the treatment groups. When compared to the uninfected control, all infected groups had a significantly higher score (infected control: p=0.014, vancomycin: p=0.015, metronidazole: p=0.036 and combination: p=0.036). (D) The myeloperoxidase (MPO) level in the proximal colonic tissue. When compared to the uninfected control, all infected groups had a significantly higher MPO-level (infected control: p=0.005, vancomycin: p=0.017, metronidazole: p=0.040 and combination: p=0.040).
Discussion
Treatment of CDI and recurrent disease is complicated and has posed a significant challenge to clinicians. Using a mouse model of CDI, we have demonstrated that mice treated with oral vancomycin had a better clinical outcome, in relation to mean relative weight, and a better microbiological outcome, in relation to the faecal bacterial load and toxin titre, in the treatment phase of CDI after the acute course of disease than mice treated with oral metronidazole. A combination of metronidazole and vancomycin did not improve the clinical or microbiological outcome. However, mice that received vancomycin or a combination of vancomycin and metronidazole succumbed to clinical and bacteriological relapse after discontinuation of treatment for CDI.
The current guidelines recommend metronidazole for the treatment of mild-to-moderate CDI and vancomycin for the treatment of severe CDI,9 ,10 based on reports of a decreased response to metronidazole treatment for CDI.5–8 In this study, we found that mice in the metronidazole group had a higher mortality of 33% vs 0% and a significantly slower clinical and bacteriological recovery, compared to vancomycin, indicating that metronidazole is less effective than vancomycin in the treatment of CDI in mice. The reason for this is not clear, but could be associated with the pharmacokinetics of metronidazole and vancomycin. When given orally, metronidazole is highly absorbed and faecal concentrations of metronidazole have been found to be undetectable in patients without diarrhoea, only reaching modest to therapeutic levels in patients with diarrhoea.34 ,35 Whereas, when administered orally, vancomycin does not get readily absorbed and vancomycin levels in faecal samples from patients with high stool frequency have been reported to be consistently 100–1000 times higher than the MIC90.36 In our study, loose stools and diarrhoea among all the infected mice stopped at around days 3–4, presumably causing suboptimal intraluminal concentrations of metronidazole and thereby possibly slow clinical recovery and lack of bacteriological cure. This theory is supported in a recent prospective study of patients with CDI, where most vancomycin-treated patients were found to maintain inhibitory concentrations of vancomycin in stool for 4–5 days after therapy, whereas metronidazole was only detectable during therapy.37 Furthermore, a retrospective study by Wilcox and Howe38 showed that symptomatic response time was significantly shorter in patients treated with vancomycin compared to those treated with metronidazole (3.0 vs 4.6 days, p<0.01). Furthermore, findings similar to ours, in relation to weight loss and mortality, of the response to metronidazole and vancomycin treatment of C. difficile-infected mice, has been reported.26 ,39 Despite the fact that vancomycin was effective in controlling CDI in the treatment phase, vancomycin-treated mice (both vancomycin alone and in combination with metronidazole) experienced a relapse at around day 15. The disease severity of relapse was severe and resulted in a mortality rate in the vancomycin group similar to the mortality rate seen in the infected control during acute CDI. The reason for the relapse of CDI is not clear but, of course, it requires the presence of vegetative C. difficile or C. difficile spores. Furthermore, relapse of CDI in vancomycin-treated mice has been reported elsewhere26 ,39–41 and it has also been reported in mice after treatment with fidaxomicin.39 Fidaxomicin, similarly to vancomycin, is not readily absorbed in the gut and therefore generates high intraluminal concentrations in the colon. On the basis of this and on histopathological findings, Warren et al39 suggested that the relapse seen in mice after both vancomycin and fidaxomicin treatment could be due to a tissue injury and may not have the same mechanism as that underlying relapse or recurrence in humans. Furthermore, reducing the dosage and length of treatment with vancomycin reduces the risk of relapse.39
A combination of metronidazole and vancomycin is sometimes recommended in severe cases of CDI. When the antimicrobial interaction of metronidazole and vancomycin against C. difficile is investigated in vitro, the results indicate no difference between the two agents.21 However, in theory, a combination therapy of CDI with vancomycin and metronidazole could be beneficial given the differences in the pharmacokinetics of these two agents. We found that mice treated with a combination of vancomycin and metronidazole had a fast clinical and microbiological recovery similar to the mice treated with vancomycin alone. However, we did not find an improved clinical outcome with the combination when compared to vancomycin. In fact, there was a mortality of 17% in the combination group compared to 0% in the vancomycin group during the treatment phase, indicating that the combination was less effective than vancomycin. Some clinical studies have reported results similar to ours. In a study by Pépin et al,22 patients treated with the combination fared worse than their counterparts treated with either drug, however, this was true only for a small number of patients, and with the risk of severity as a confounding factor. Additionally, in a retrospective review of CDI in patients with haematological malignancies, response rates to metronidazole, vancomycin and the combination were 53.7%, 50% and 38.5%, respectively, though not significant.23 Hence, if treatment with the combination is not better than treatment with vancomycin alone, a combinational therapy might not be an advantage in the treatment of CDI, as this can cause further disruption of the normal enteric microflora and subsequently facilitate the growth of any C. difficile organisms still present in the colon or acquired from an exogenous source.
A limitation to our study was the relatively small number of mice. Hence, at relapse, several mice had died during the initial course of infection and this resulted in low power for the comparison of groups at relapse. Furthermore, we were not able to examine the concentration of metronidazole and vancomycin in the faecal samples, as the collected samples were used for the measurement of faecal spore load and cytotoxicity. Also, this study uses the mouse model of CDI developed by Chen et al26 and, because treatment is started at day 1 after the C. difficile challenge, one may argue that this was a prevention of infection/death model as opposed to treatment of infection, and all mice within the respective groups were treated equally despite the fact that not all mice became equally ill. Overall, the limitation of data from a mouse model means that our study alone cannot influence clinical decision-making, but supports further investigation in humans.
In conclusion, using an in vivo mouse model, we found that treatment of CDI with vancomycin alone is as effective as treatment with vancomycin and metronidazole in combination. We believe that this is an important finding and, if possible, it should be tested in a clinical setting. Antimicrobial therapy is one of the most dominant risk factors for CDI, and if there is no advantage in using combinational therapy, patients with severe CDI may benefit from alternative options instead of additional antimicrobial therapy. If our findings could be reproduced in a clinical setting, this new knowledge could lead to a reduction in the use of a combination of vancomycin and metronidazole for the treatment of severe CDI in humans.
Acknowledgments
The authors would like to thank Pfizer R&D's Investigator-Initiated Research programme and the Scandinavian Society for Antimicrobial Chemotherapy for supporting this work. Preliminary results were presented as poster P-027 at NSCMID 2013 in Aarhus, Denmark.
References
Footnotes
Contributors LTE, FD-H, BK, KEPO and KF were responsible for conception, design and overall supervision of the study. LTE, MA, RH-M and KEPO were involved in collection and analysis of samples. LTE, BK, KEPO and KF participated in analysis and interpretation of data and drafting of manuscript. LTE, FD-H, RH-M, KEPO and KF were responsible for provision of materials and services. All the authors were involved in critical revision of manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.