Article Text

Abstract
Objectives The long-term goal for chronic hepatitis B patients is to maintain viral suppression in order to reduce disease progression risk. Because patients with previous treatment failure may have multiple viral resistance mutations, finding effective therapy is challenging. Because recent studies have shown that the combination of entecavir and tenofovir is effective in achieving virological response in many patients with prior treatment failure and multiple drug resistance mutations, we compared outcomes with this combination versus monotherapy.
Methods With a retrospective chart review we compared results in 35 patients with previous treatment failure treated with the entecavir-tenofovir combination to results in patients treated with entecavir monotherapy.
Results Although combination therapy resulted in significantly faster achievement of DNA negativity compared to entecavir monotherapy, the modest ten-week advantage is unlikely to be important for most patients since entecavir resistance develops extremely slowly. Significantly more patients on combination therapy experienced viral breakthroughs, most of which were attributed to non-adherence due to difficulties with the combination regimen.
Conclusions Our findings of reasonably comparable efficacy over time in the combination and monotherapy arms combined with the increased costs and compliance issues related to combination therapy weigh in favor of entecavir monotherapy in patients with previous treatment failure. However, because our study was a retrospective analysis of a small patient population, it will be important to confirm these findings with a randomised, controlled trial that compares these treatment approaches in treatment-experienced patients.
- HEPATITIS B
- ANTIVIRAL THERAPY
- ADVERSE DRUG REACTIONS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Finding effective therapy for patients with chronic hepatitis B virus (HBV) infection who have had previous treatment failure, many of whom have multiple viral resistance mutations, is a challenge.
▸ Several recent studies have shown that combination therapy with entecavir (ETV) and tenofovir (TDF) is effective in achieving virological response in the majority of patients with prior treatment failure and multiple drug resistance mutations.
▸ Studies comparing TDF monotherapy to combination therapy with ETV and TDF in patients with resistance mutations have had mixed results, with two studies reporting that combination therapy was superior to TDF monotherapy, and one reporting that results with TDF monotherapy were comparable to those seen with ETV-TDF combination therapy.
▸ Although one study has compared ETV monotherapy to ETV-TDF combination therapy only in ETV partial responders, finding that combination therapy was superior, no study has yet compared ETV monotherapy to ETV-TDF combination therapy in CHB patients with previous treatment failure to a variety of nucleos(t)ide analogues.
What are the new findings?
▸ Patients with previous treatment failure treated with ETV–TDF combination therapy achieved DNA negativity significantly faster than patients treated with ETV monotherapy; however, the modest 10-week advantage is unlikely to be important for most patients, since resistance to ETV develops extremely slowly.
▸ Significantly more patients on combination therapy experienced viral breakthroughs, most of which were attributed to non-adherence due to difficulties with the combination regimen.
▸ Our findings of reasonably comparable efficacy over time in the ETV–TDF combination and ETV monotherapy arms combined with the increased costs and compliance issues related to combination therapy weigh in favour of ETV monotherapy in patients with previous treatment failure.
How might our findings impact clinical practice in the foreseeable future?
▸ Our finding that the combination of ETV–TDF appears comparable with ETV monotherapy in patients with previous treatment failure, combined with the higher cost of the combination and the fact that it may lead to more adverse effects and non-compliance, may lead clinicians to consider ETV monotherapy in these patients. However, because our study was a retrospective analysis of a small patient population, it will be important to confirm these findings with a randomised, controlled trial that compares these treatment approaches in treatment-experienced patients.
Although not all patients with chronic hepatitis B (CHB) suffer serious sequelae of infection, 15–40% develop cirrhosis or hepatocellular carcinoma (HCC),1 with the risk increased by higher serum hepatitis B virus (HBV) DNA and elevated alanine aminotransferase (ALT) levels.2–5 The long-term goal of antiviral therapy is to maintain viral suppression and normal ALT, thus lowering the risk of these complications.6–8 Owing to a high relapse rate, the majority of patients with CHB receive long-term antiviral therapy to achieve continuous suppression of HBV DNA replication and/or hepatitis B e antigen (HBeAg) seroconversion (in patients with wild-type virus), and ultimately hepatitis B surface antigen (HBsAg) seroconversion.9
Of the five oral nucleos(t)ide analogues currently approved for HBV treatment in the USA, tenofovir disoproxil fumarate (TDF) and entecavir (ETV) are currently the first-line therapies because of high potency, good efficacy and high genetic or functional barriers to resistance. In treatment-naïve patients, ETV resistance was seen in ∼1% after 5 years of therapy;10 ,11 no TDF resistance mutations have been clearly identified in the treatment-naïve through up to 240 weeks of treatment although there may be phenotypic resistance to treatment when adefovir dipivoxil (ADV) resistance mutations are present.12–15 However, the greater challenge is finding effective therapy for patients with previous treatment failure, many of whom have multiple viral resistance mutations. ETV monotherapy is effective in patients with ADV resistance,16 ,17 and in some patients with lamivudine (LAM) resistance.18 In 77 LAM-refractory patients (85% with documented LAM resistance mutations), it was shown that in the second year of ETV treatment, 40% achieved HBV DNA <300 copies/mL.18 A large-scale retrospective study showed that TDF efficacy was not influenced by the presence of mutations associated with LAM resistance, but was diminished in patients with ADV resistance (100% vs 52% probability of HBV DNA <400 copies/mL, respectively).15
The results from such studies combined with these drugs’ known high barriers to resistance led to a consideration that ETV–TDF combination therapy might have synergistic or additive antiviral effects that would create an effective regimen for patients with nucleos(t)ide analogue resistance mutations, previous treatment failure and/or inadequate viral suppression with monotherapy. Studies have now shown complete viral response in patients with CHB treated with ETV plus TDF in 80%,19 86%20 and 89%21 of patients with multiple resistance mutations, and 85%22 of patients with prior treatment failure. Studies have compared TDF monotherapy to combination therapy with ETV and TDF in patients with resistance mutations, with two studies finding combination therapy to be superior to TDF monotherapy,23 ,24 and one reporting similar results.25 A study of previously treatment-naïve patients who were only partial responders to ETV (with detectable HBV DNA after ≥12 months on ETV) found that more patients switched to ETV–TDF combination treatment achieved complete viral suppression compared with those who continued ETV monotherapy.26 However, to date, there are no studies comparing ETV monotherapy with combination therapy with ETV–TDF in patients with previous treatment failure and resistance.
Consideration of combination therapy requires taking into account possible undesirable aspects, including potentially higher rates of side effects, higher treatment costs, lower adherence rates due to pill number or regimen complexity, reduced efficacy due to drug competition, and creation of multidrug-resistant HBV if the combination is insufficient to prevent resistance.27 We performed a retrospective chart analysis in order to compare the outcomes, including viral suppression and adverse events, in patients with treatment failure and resistance to many different nucleos(t)ide analogues treated with ETV–TDF combination therapy versus ETV monotherapy in matched patients.
Methods
Study population
A retrospective chart review evaluated 35 patients with previous treatment failure who were treated with ETV–TDF combination therapy for a minimum of 6 months. Complete patient demographics are shown in table 1. Patients with CHB were defined as having previous treatment failure if while taking any oral nucleos(t)ide they exhibited persistent HBV DNA positivity or presented evidence of viral breakthrough, with or without evidence of resistance mutations. Persistent HBV DNA positivity was defined as a flat virological response (less than 1 log reduction over 3 months) or continuing DNA positivity after 2 years on oral therapy. Viral breakthrough was defined as viral rebound, 1 log greater than nadir, or 1 log greater than the lower limit of quantification, while being compliant with therapy. Patients were matched by gender and age (±10 years) to 35 patients on ETV monotherapy who had also been on treatment for a minimum of 6 months prior to enrolment. Sixteen of these patients were HBV treatment-naïve, while 19 had been switched to ETV monotherapy from alternative combinations or monotherapies (table 2) due to non-response; only 3 (8.6%) had documented drug resistance; the only resistance identified was to lamivudine; lamivudine resistance was defined as detection of the M204 mutation. This ETV treatment arm was used to compare safety and efficacy profiles of monotherapy versus combination therapy in terms of incidence of adverse events and time to HBV DNA negativity. Patients with a history of organ transplantation, with any other diagnosed concurrent liver disease, and/or with HIV, hepatitis C virus, hepatitis delta virus, or hepatitis E virus coinfection were excluded. Patients were also excluded if they were younger than 18 years of age and/or if they had an undetectable viral load at baseline.
Patient demographics
Patient treatment histories and documented drug resistance mutation testing results
Patients were followed for up to approximately 18 months after the initiation of combination therapy. For patients without an 18-month follow-up date, the next closest HBV DNA lab value, within 1 year of what would be their 18-month follow-up, was used. Eight patients in the combination therapy arm and 10 patients in the ETV monotherapy arm were lost to follow-up prior to 18 months. HBV DNA was measured using real-time PCR (COBAS AmpliPrep/COBAS TaqMan HBV Test, V.2.0, Roche, Basel, Switzerland). For our analysis, we used baseline HBV DNA levels taken either at the initiation of combination therapy or ETV monotherapy, or at the closest date before initiation of treatment. All subsequent HBV DNA levels available in each patient's chart were also recorded. When HBV DNA laboratory values were measured in ‘copies,’ a conversion factor of 0.179 was used to convert to IU/mL. HBV drug resistance mutations reported were determined using either Inno-LiPA or direct sequencing assays.
Statistical analyses
Continuous data are summarised as means with SD, or median with range. Categorical data are summarised as frequency and percentages. Continuous data are compared between groups using the Student t test or the Mann-Whitney test. Categorical variables were analysed using Fisher's exact test. Time until first detection of DNA negativity was compared between groups using the log-rank test. Cox proportional hazard model was used to adjust for covariates that are not balanced between the two groups, or of interest otherwise. A p value of <0.05 was considered to be statistically significant for all tests. Analyses were performed using the open source statistical programming language R.
Results
Patient characteristics
Twenty-two men and 13 women were enrolled in each arm of this study. The mean age of patients in the ETV–TDF combination therapy arm was 50.3 years (range 26.7–75.2 years old), and of patients in the ETV monotherapy arm 49.6 years (range 20.8–75.1 years). Previous treatment profiles for patients in both arms are summarised in table 2.
Efficacy analysis
ETV only versus ETV–TDF combination arms
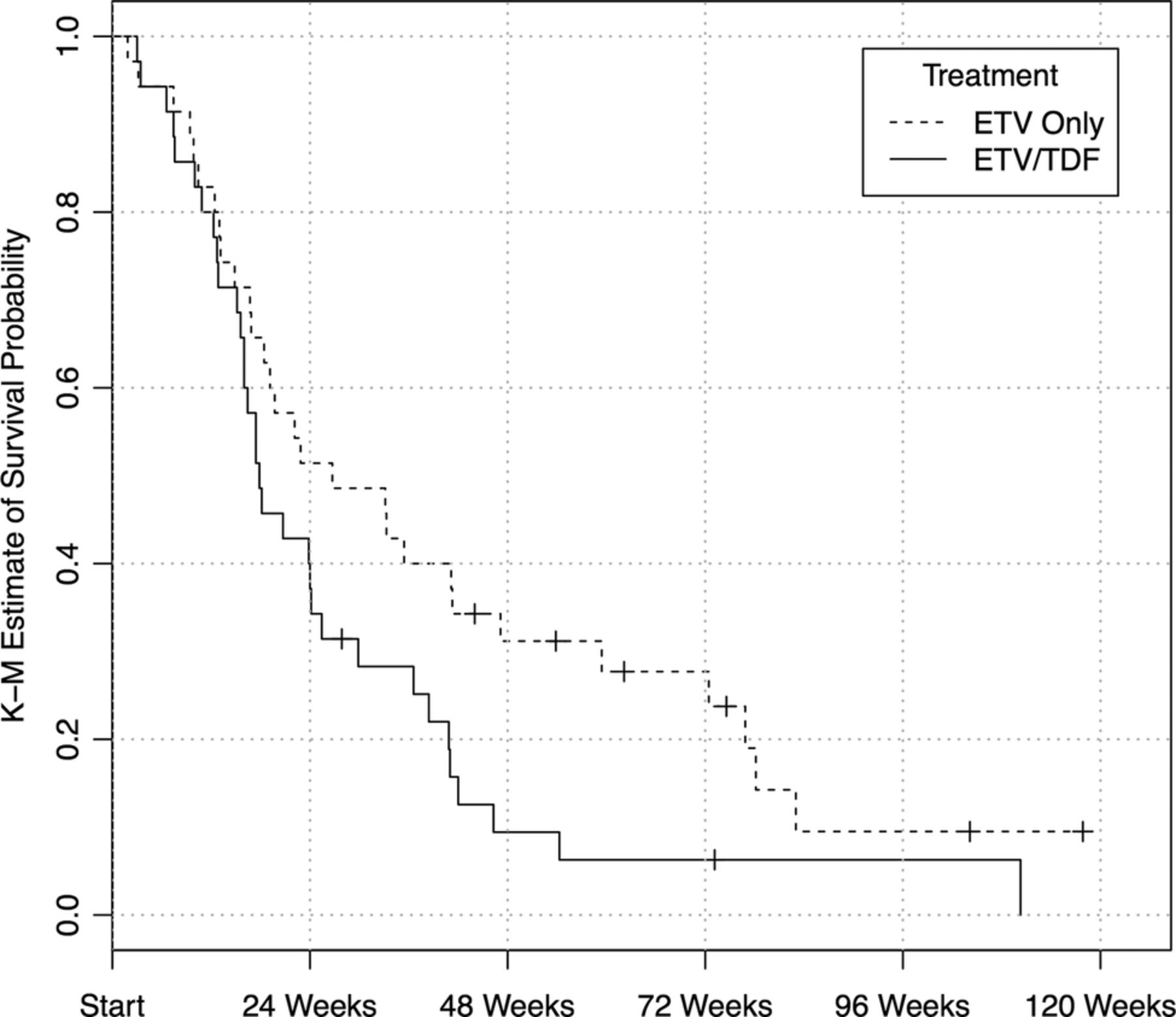
The difference in the distribution of time to first detection of DNA negativity between patients in the ETV-only group (median 27 weeks) and the ETV–TDF combination group (median 18 weeks) was found to be significantly different (p=0.049, log-rank test), as shown in figure 1. When controlling for baseline HBV DNA level, HBeAg status and prior exposure to ADV in a Cox proportional hazards model, the difference between the ETV-only group and the ETV–TDF combination group remained significant (p=0.004, table 3). HBeAg-positive patients were shown to take significantly longer to achieve HBV DNA negativity compared with HBeAg-negative patients (p<0.001). There were two and six participants with censored time to HBV DNA negativity in the ETV–TDF and ETV-only groups, respectively.
{kind=link}
Kaplan–Meier estimates of time until first detection of HBV DNA negativity. Hash marks indicating censored values. The distribution of days until first detection of HBV DNA negativity was found to be significantly different between patients in the ETV only and ETV–TDF combination group, via the log-rank test (p=0.049). (ETV, entecavir; HBV, hepatitis B virus; TDF, tenofovir disoproxil fumarate)
Output for the Cox proportional hazard model for time until the first detection of DNA negativity
ETV–TDF combination arm
The median baseline HBV DNA level for the ETV–TDF combination therapy arm was 6510 IU/mL with a range from 396 to 2×107 IU/mL. Times until first detection of HBV DNA negativity in this arm are presented in figure 1. Median time to DNA negativity was 18 weeks (range 3–110+ weeks). Among the patients treated with ETV–TDF, the difference in the distribution of days until first detection of DNA negativity in patients with previous resistance to LAM (median time 16 weeks, n=7) and without LAM resistance (median time 19 weeks, n=28) was not statistically significant (p=0.392 via log-rank test). The difference in the distribution of days until first detection of DNA negativity was also found not to be statistically significant between patients with previous exposure to ADV (median time 24 weeks, n=15) and without previous exposure to ADV (17 weeks, n=20, p=0.540 via log-rank test).
Six patients had their TDF doses reduced and three patients had their ETV doses reduced due to adverse events or changes in renal function. Of the 25 HBeAg-positive patients, 2 achieved HBeAg seroconversion while on therapy (one at 24 weeks and one at 46 weeks). Seven patients experienced viral breakthrough while on combination therapy; 6 of these patients experienced viral breakthrough attributed to non-compliance; after becoming compliant, 5 of these patients achieved undetectable levels of HBV DNA by the end of follow-up.
One patient experienced breakthrough at 16 months after their TDF dose was decreased from 300 mg daily to 300 mg every other day due to a serum creatinine increase of 0.3; after normalisation of the creatinine, they were returned to the full dose of 300 mg daily which resulted in a return to HBV DNA negativity by their next follow-up appointment (29 months).
ETV monotherapy arm
Median baseline HBV DNA level was 5.8×105 IU/mL (range 417–>5×108 IU/mL). Times until first detection of HBV DNA negativity in this arm are presented in figure 1. Median time to HBV DNA negativity was 27 weeks (range 2–83 weeks). The difference in the distribution of time to first detection of HBV DNA negativity in patients with and without documented lamivudine resistance (median time 33 weeks in 3 patients vs 23 weeks in 32 patients, respectively) was not statistically significant (p=0.669 via log-rank test). The difference in the distribution of days until first detection of DNA negativity was also found not to be statistically significant between patients with previous exposure to ADV (median time 33 weeks, n=15) and without previous exposure to ADV (24 weeks, n=20, p=0.462 via log-rank test). Two additional patients (3 in total) experienced viral breakthrough while on ETV monotherapy. Both these patients did achieve undetectable levels of HBV DNA (at 2.5 and 14 months of therapy, respectively). One of these patients experienced a minor breakthrough at their final follow-up and ended the study with a viral load of 36 IU/mL. The other experienced a 4-log breakthrough at 5 months, most likely due to non-compliance, and was HBV DNA negative less than a month later. Of the three patients that experienced breakthrough on treatment, one was nucleos(t)ide-naive and two were exposed to ADV prior to treatment with ETV but without documented resistance.
Safety analysis
ETV–TDF combination arm
Six patients had their TDF doses reduced. One patient had their dose decreased due to flatulence; three due to renal events; one due to a pre-existing renal condition with a subsequent dose increase after glomerular filtration rate (GFR) stabilisation; and one after achieving an undetectable HBV viral load. Six patients had changes in their ETV dosing on treatment. Three patients had their doses increased from 0.5 to 1 mg daily by their provider in order to potentially enhance their treatment response. Based on provider discretion, two patients had their dose reduced once they achieved undetectable HBV DNA levels. One patient was changed from ETV–TDF combination therapy to TDF monotherapy after becoming HBV DNA negative, but was promptly restarted on ETV when TDF monotherapy resulted in viral breakthrough.
One patient developed a rash after initiation of ETV–TDF combination therapy, but it was unclear if this was medication related since the rash resolved on treatment. One patient experienced right flank pain, headaches and blurry vision which may be attributed to therapy; however, no dose change was recommended. There were no incidences of lactic acidosis or other serious adverse effects reported.
ETV monotherapy arm
One patient had a dose change while on therapy. This patient started therapy at 0.25 mg daily due to a pretreatment renal condition and, for financial reasons, briefly went off therapy. When this resulted in viral relapse, the provider increased the dosage to 0.5 mg daily. Only one patient in the ETV monotherapy arm reported an adverse event, a mild rash which may or may not have been attributed to ETV. ETV was not associated with increases in serum creatinine. No cases of lactic acidosis or other serious adverse effects were reported. Table 4 details medication dose adjustments.
Dose changes on treatment for ETV–TDF combination therapy and ETV monotherapy arms
Discussion
Our study showed that combination therapy with ETV and TDF in patients with previous treatment failure who had few or no mutations resulted in significantly faster achievement of DNA negativity compared with ETV monotherapy. With antivirals in which resistance develops quickly in the setting of incomplete viral suppression, this could be important. However, although the difference in the time to reach HBV undetectability was significant, the 10-week advantage seen with the combination therapy arm is unlikely to be of importance for most patients since resistance develops extremely slowly with ETV. Although the faster achievement of negativity might theoretically be considered more important in patients with lamivudine resistance, since in patients without such resistance the development of resistance to ETV is very unlikely, in our comparison, the difference in the distribution of time to first detection of HBV DNA negativity was not statistically significant in patients with and without documented lamivudine resistance in either the combination therapy group or the ETV monotherapy group. However, our analysis of the effect of lamivudine resistance may be underpowered, as there were only seven and three individuals with documented lamivudine resistance in the ETV–TDF and ETV-only groups, respectively, and the follow-up was short; thus, we cannot confirm the efficacy of ETV monotherapy in patients with lamivudine resistance.
Treatment adherence was shown to be an issue with the combination therapy. Patients are told to take ETV on an empty stomach, and TDF after a meal, making the combination regimen potentially difficult and confusing for some patients. Significantly more patients in the combination arm experienced a viral breakthrough compared to the ETV monotherapy arm (seven and three, respectively); viral breakthrough in six of seven patients in the ETV–TDF combination arm and in one of three patients in the ETV monotherapy arm were attributed to non-adherence, as endorsed by the patients to their treating physicians; most of them achieved virological response once they became compliant with the medications. Non-compliance leading to viral breakthrough in the short term and to drug resistance in the long term can result in difficult-to-treat chronic HBV and in progressive disease and its related complications. Thus, monotherapy with ETV (as suggested by our results), or monotherapy with TDF as suggested by the study by Lim et al,28 could be considered as an alternative to a multidrug regimen. Treatment costs were, obviously, higher in the combination therapy arm with an estimated annual cost of approximately US$2900 for ETV monotherapy compared with approximately US$4700 for the ETV–TDF combination. Despite the fact that no serious adverse events occurred in either arm of this study, seven patients in the combination arm compared with one patient in the ETV monotherapy arm experienced adverse events; four patients in the combination therapy arm experienced small changes in creatinine and/or GFR requiring dose modification but not therapy discontinuation (table 4); one patient in this arm experienced gassy symptoms, one patient rash and one patient right flank pain, blurry vision and headache. The only adverse event reported in the ETV monotherapy arm was a rash that did not require dose modification or discontinuation. In our study, there was no difference between the ETV–TDF combination arm and the ETV monotherapy arm in patients who were either non-responders or partial responders to nucleos(t)ide analogues, including some patients with genotypic resistance to nucleoside or nucleotide medications. These findings in combination with the increased costs and the compliance issues that in some patients resulted in viral breakthrough in the combination therapy arm weigh in favour of the use of monotherapy with a first-line therapy (currently, ETV or TDF) in patients with previous treatment failure, followed by a transition to combination therapy in patients who fail either ETV or TDF monotherapy. However, because our study was a retrospective analysis of only a small patient population, it will be important to confirm these findings with a randomised, controlled trial that compares these treatment approaches in treatment-experienced patients.
References
Footnotes
Contributors SB made substantial contributions to the study concept and research design; acquisition of the data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; approval of the submitted and final versions. JP and RX made substantial contributions to analysis and interpretation of the data; statistical analysis; critical revision of the manuscript; approval of the submitted and final versions. SK and MC made substantial contributions to acquisition of the data; drafting of the manuscript; approval of the submitted and final versions. RG made substantial contributions to the study concept and research design; acquisition of the data; analysis and interpretation of the data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; approval of the submitted and final versions.
Funding This project was supported by the California Pacific Research Institute where the research was carried out. There was no grant support for this project. Initial data analyses were undertaken only by authors. Writing assistance was provided by Dr Lark Lands (self-employed medical editor) and funded by RG Consultants, L.L.C.
Competing interests RG was on the advisory, scientific and speakers bureaus for both Bristol-Myers Squibb and Gilead at the time of this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.