Article Text

Abstract
Objective It has been established that use of proton pump inhibitors (PPIs) is associated with an increased risk of acquiring Clostridium difficile-associated diarrhoea (CDAD). However, it is not known whether the use of PPIs or histamine-2 receptor antagonists (H2RAs) concurrently with CDAD-targeted antibiotic treatment affects clinical response or recurrence rates.
Design In two phase 3 trials, patients with toxin-positive CDAD were randomised to receive fidaxomicin 200 mg twice daily or vancomycin 125 mg four times daily for 10 days. Only inpatients with CDAD (due to complete medication record availability) were included in this post hoc analysis: 701 patients, of whom 446 (64%) used PPIs or H2RAs during study drug treatment or follow-up. Baseline factors that were statistically significant in univariate analyses were analysed in multivariate analyses of effects on clinical response and recurrence.
Results Multivariate analysis showed that leukocytosis, elevated creatinine and hypoalbuminemia, but not PPI or H2RA use, were significant factors associated with poor clinical responses. Treatment group was the single significant predictor of recurrence; the probability of recurrence after fidaxomicin therapy was half that following vancomycin therapy.
Conclusions Acid-suppressing drugs, used by nearly two-thirds of inpatients with CDAD, did not worsen clinical response or recurrence when used concurrently with fidaxomicin or vancomycin. Therefore, development of CDAD does not require discontinuation of anti-acid treatment in patients who have an indication for continuing PPI or H2RA therapy, such as gastro-oesophageal reflux disease and risk of gastrointestinal bleed.
- BACTERIAL OVERGROWTH
- PROTON PUMP INHIBITION
- DIARRHOEA
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Proton pump inhibitor (PPI)/histamine-2 receptor antagonist (H2RA) use is common in patients with Clostridium difficile-associated diarrhoea (CDAD) and often is not founded on evidence-based medicine.
▸ It is unknown whether concurrent use of PPI/H2RA with CDAD-targeted antibiotics damages clinical response.
▸ Some studies have reported that PPI/H2RA use increased the risk of recurrence, but the studies had small sample sizes and were not carefully controlled.
What are the new findings?
▸ PPI/H2RA used concurrently with fidaxomicin or vancomycin had no adverse effects on clinical response among inpatients with CDAD.
▸ In a multivariate analysis, recurrence rates were influenced by numerous other factors, but not by PPI/H2RA use.
▸ Treatment with fidaxomicin was the single significant predictor of CDAD recurrence.
How might it impact on clinical practice in the foreseeable future?
▸ Our results show that development of CDAD does not require discontinuation of PPI or H2RA treatment in patients who have an indication for continuing such therapy.
Introduction
The use of proton pump inhibitors (PPIs) and histamine-2 receptor antagonists (H2RAs) is among modifiable factors that may increase the risk of acquiring Clostridium difficile-associated diarrhoea (CDAD). Recent publications indicate that PPI exposure may increase the risk of community-acquired CDAD and that the risk of nosocomial CDAD increases along with the frequency of PPI or H2RA use.1–3 An explanation for the association of PPI use with CDAD risk may be the ability of PPIs to reduce gastric acidity, thereby disabling a natural defence against ingested C. difficile spores.4
However, the matter remains controversial.2–6 PPI use may increase the risk of community-acquired CDAD, but the supporting studies are heterogeneous and considered inconclusive by some observers.1 ,7 Recent reports also indicate that PPI use during and after metronidazole or vancomycin therapy may increase recurrence rates by 40–60%.1 ,8–12
PPIs and H2RAs are used to treat dyspepsia, gastroduodenal ulcers, gastro-oesophageal reflux disease, and to reduce the risk of medication-induced or stress-induced gastrointestinal haemorrhage. They are frequently administered prophylactically to critically ill hospital patients and their use often continues after hospital discharge.13 Both PPIs and H2RAs are accessible without prescriptions.14 PPIs are one of the most commonly used medicines worldwide.15 It has been alleged that virtually 70% of PPI use either cannot be attributed to evidence-based medical reasoning or is associated with unsuitable indications.14 ,16–21 The US Food and Drug Administration (FDA) recently issued a safety communication to the public indicating an association between PPI use and increased risk of CDAD. The announcement recommended that a CDAD diagnosis be considered in cases where patients who use PPIs experience persistent diarrhoea.22 The agency is currently evaluating similar risks among patients using H2RAs. In hospitalised patients, by extension, it can be hypothesised that concurrent use of PPIs and H2RAs may adversely affect response to CDAD treatment, and that anti-acid therapy should be discontinued.
Fidaxomicin is the first antimicrobial treatment for CDAD to be approved by the FDA in more than 25 years.23 Fidaxomicin targets bacterial RNA polymerase.24 ,25 Recent data from two phase 3 clinical trials showed that fidaxomicin is non-inferior to oral vancomycin in achieving clinical response and is superior to oral vancomycin in maintaining a sustained clinical response, which is an initial response with no relapse or death during the subsequent 25 days of follow-up.26–28 Using data from these phase 3 trials, we analysed whether the use of PPIs or H2RAs during a course of CDAD-specific antibiotic therapy with fidaxomicin or vancomycin might affect clinical response or recurrence rates in hospitalised patients.
Methods
Data from two identical, independent, randomised, controlled, phase 3 trials comparing the safety and efficacy of fidaxomicin versus vancomycin were pooled for this study of the effect of PPIs and H2RAs on the clinical response of hospitalised patients with CDAD to fidaxomicin or vancomycin therapy. Study NCT00314951 was conducted in the USA and Canada from May 2006 through August 2008, and study NCT00468728 was conducted in the USA, Canada and Europe from April 2007 through December 2009.26 ,28 Primary and secondary end points were clinical response and recurrence rate, respectively.
Patients were ≥16 years of age, had >3 unformed bowel movements (UBM) during the 24 h preceding randomisation, had CDAD confirmed by the presence of toxin A and/or B in the 48 h period preceding randomisation, and had ≤1 episode of CDAD in the preceding 3 months. Patients were randomised to receive 10 days of treatment with oral fidaxomicin 200 mg twice daily and intervening placebo capsules twice daily (n=539) or oral vancomycin 125 mg four times daily (n=566). Treatment with other potentially effective CDAD therapies was prohibited.
The modified intent to treat (mITT) population comprised patients who were randomised to receive daily therapy of fidaxomicin 400 mg or vancomycin 500 mg, had CDAD confirmed by clinical observation and a positive C. difficile toxin assay, and received at least one dose of study drug. Only inpatients were included in this post hoc analysis because it was important to verify by study records the use of the drugs of interest, PPIs and H2RAs. Data on PPI or H2RA use during the two phase 3 studies were derived from medication records compiled in case report forms at each clinical study site. PPIs of interest were esomeprazole, lansoprazole, omeprazole, pantoprazole and rabeprazole. H2RAs of interest were famotidine, ranitidine and cimetidine.
Diarrhoea was defined as a change in bowel habits, with >3 UBM (or >200 mL unformed stool for patients with rectal collection devices) during the 24 h before randomisation, and the presence of C. difficile toxin A and/or B in the stool within 48 h before randomisation. Clinical response was defined as the resolution of diarrhoea (≤3 UBM for 2 consecutive days) through the end of therapy and subsequently for 2 days, after which patients were followed for 4 weeks for recurrence. Treatment failure was defined as persistent diarrhoea, the need for additional CDAD treatment, or both. Recurrence was defined as the reappearance of CDAD symptoms during follow-up; C. difficile toxin A, B or both in stool; and the need for additional therapy. Sustained clinical response was defined as clinical response with no recurrence or death. Concomitant antibiotic use was defined as taking one or more intravenous or oral doses of an antibiotic during the treatment or follow-up periods.
Patients were evaluated daily during treatment for clinical response or failure. Patients who responded to treatment were assessed for signs of recurrence during weekly phone contact through the fourth week of follow-up after the end of therapy visit. Foecal samples were collected before the first dose of study drug was administered, again at the end of therapy, and on recurrence of symptoms. These samples were assayed for C. difficile toxins A and B.
Univariate analyses were performed to determine the effect of PPI or H2RA use on clinical response and recurrence among inpatients who used or did not use PPIs or H2RAs during the treatment phase (study days 1–10), during the follow-up period (study days 11–40), and at any time (study days 1–40) during the two phase 3 studies. Baseline factors that were statistically significant in univariate analyses of categorical variables were included in multivariate analyses.
Multivariate analysis of clinical response and recurrence rates among inpatients was performed using six categorical variables: age (in decades), serum albumin (<2.5 vs ≥2.5 g/dL), serum creatinine (≥1.5 vs <1.5 mg/dL), white cell count (≥15×109 vs <15×109/L), treatment group (fidaxomicin vs vancomycin) and PPI or H2RA use (PPI vs H2RA vs PPI and/or H2RA).
The phase 3 studies were consistent with good clinical practices and were conducted in accordance with ethical principles originating in the Declaration of Helsinki, the International Conference on Harmonization and relevant regulatory requirements. Patients provided informed consent before participating in either study.
Results
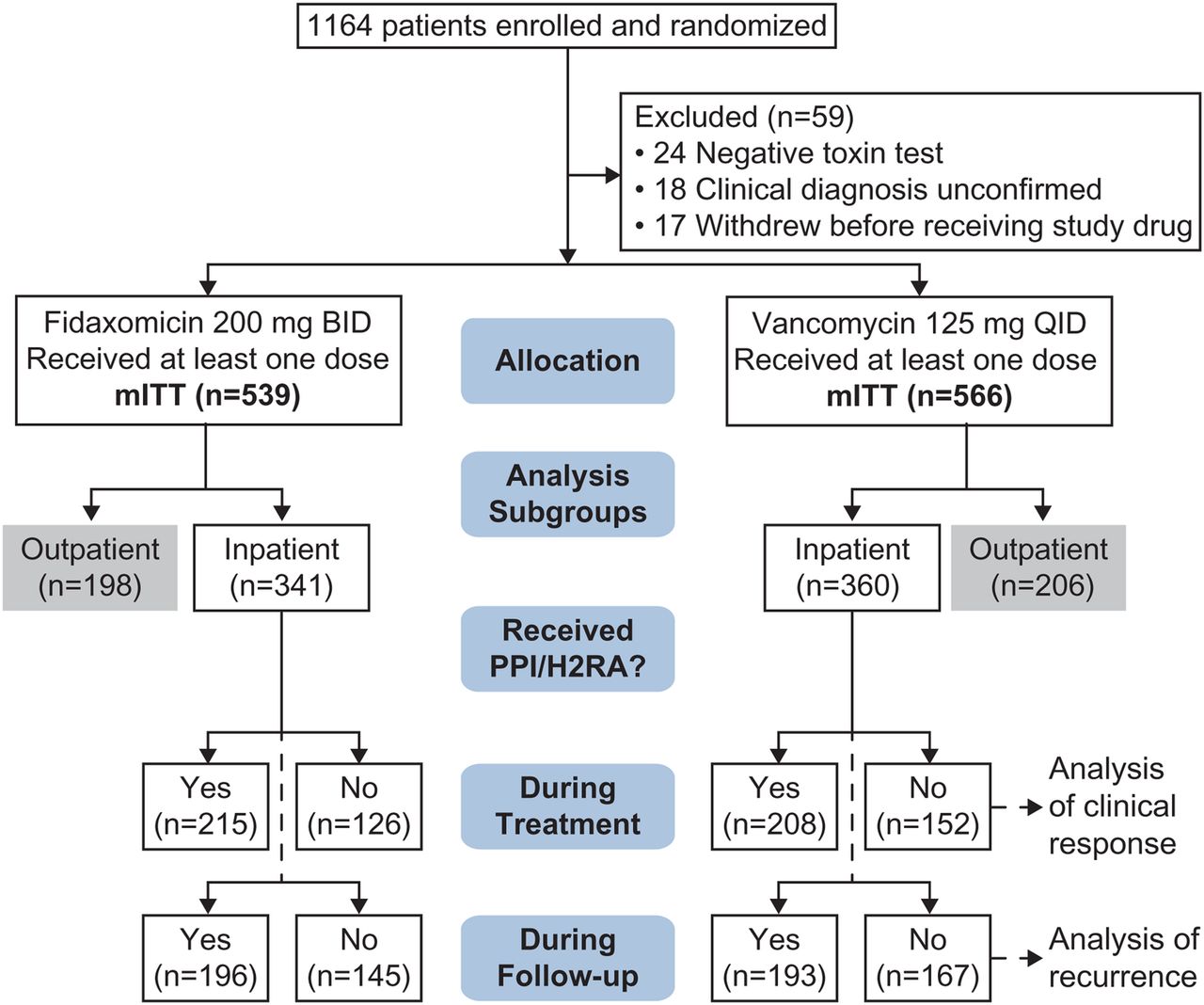
Among the 1105 mITT patients, 49% were randomised to receive fidaxomicin (n=539) and 51% were randomised to receive vancomycin (n=566). Of the 1105 mITT patients, 701 (63%) were hospitalised at the time of study enrolment and treated for CDAD as inpatients (figure 1). The analyses are based on these 701 inpatients. Baseline and disease characteristics for the inpatient study population are provided in table 1.
Baseline and disease characteristics (mITT inpatients, n=701)
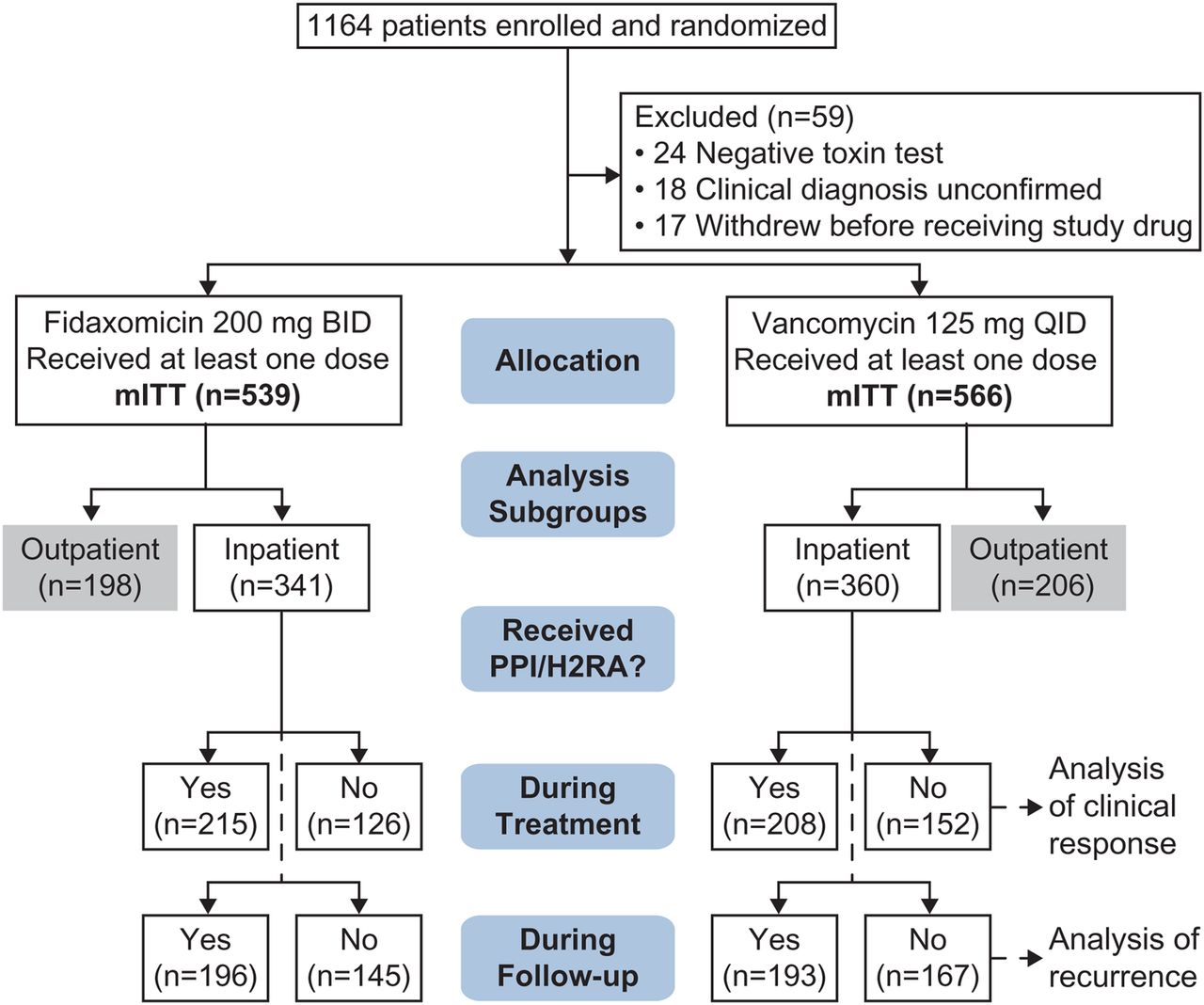
Patient disposition. In two phase 3 trials, 1164 patients with CDAD were enrolled and randomised. The mITT population used for this analysis comprised 539 patients who received at least one dose of fidaxomicin and 566 patients who received at least one dose of vancomycin. BID, twice a day; CDAD, Clostridium difficile-associated diarrhoea; H2RA, histamine-2 receptor antagonist; mITT, modified intent to treat; PPI, proton pump inhibitor; QID, four times a day.
Of the 701 hospitalised patients, 482 (69%) used PPIs or H2RAs at some time during the periods of interest (ie, during the pretreatment, treatment or follow-up periods). Overall, PPI use by inpatients was more common than H2RA use, and use of either type of drug by inpatients was highest in the 10-day treatment phase, during which 423 (60%) of inpatients used PPIs and/or H2RAs (table 2). Among the inpatients who used PPIs or H2RAs concomitantly with C. difficile-targeted antibiotics during the treatment phase, 380 (54%) used a PPI, 55 (8%) used an H2RA, and 12 (2%) used both. During the follow-up period, 389 (55%) of inpatients used PPIs and/or H2RAs. Among inpatients who used these drugs during the follow-up period, 353 (50%) used a PPI, 54 (8%) used an H2RA and 18 (3%) used both.
PPI and H2RA use during phase 3 studies (mITT inpatients, n=701)
Univariate analysis showed that achievement of clinical response by inpatients was not affected by concurrent use of PPI or H2RA with fidaxomicin or vancomycin therapy; 344/423 (81%) of inpatients who used PPIs and/or H2RAs achieved clinical response, while 231/278 (83%) of non-users similarly achieved clinical response.
After adjusting for the effects of PPI and/or H2RA use on clinical response, multivariate analysis of the effects of potential predictors of clinical response showed that hypoalbuminemia (OR 0.497, 95% CI 0.320 to 0.774, p=0.0020), elevated serum creatinine (OR 0.547, 95% CI 0.339 to 0.883, p=0.0135) and leukocytosis (OR 0.605, 95% CI 0.373 to 0.980, p=0.0411) were independent predictors of poor clinical response among inpatients who used PPIs and/or H2RAs (table 3). Similar effects on clinical response were observed among inpatients who used PPIs and, separately, among inpatients who used H2RAs.
Multivariate analysis: effect on clinical response of acid suppressants taken concurrently with CDAD-targeted antibiotics (mITT inpatients, n=701)
Univariate analysis showed that PPI or H2RA use during the treatment phase (study days 1–10) had no effect on recurrence rates. A similar proportion of inpatients who used PPIs or H2RAs during the treatment phase experienced recurrence as compared with patients who did not (75/344, 22% vs 44/231, 19%, respectively). Conversely, although not observed subsequently in multivariate analysis, PPI or H2RA use during the follow-up period (study days 11–40) had a significant effect on recurrence rates. Inpatients who used PPIs or H2RAs during the follow-up period experienced significantly higher recurrence than inpatients who did not (76/315, 24% vs 43/260, 17%, p=0.025).
After adjusting for age, high serum creatinine, hypoalbuminemia, leukocytosis, and PPI or H2RA use, multivariate analysis of recurrence showed that treatment (fidaxomicin vs vancomycin) was a significant predictor of recurrence. Fidaxomicin reduced the probability of recurrence by half, compared with vancomycin, among inpatients who used PPIs and/or H2RAs at any time (OR 0.498, 95% CI 0.313 to 0.793, p=0.003). Similar effects on recurrence were observed among inpatients who used PPIs and, separately, among inpatients who used H2RAs (table 4). In addition, high serum creatinine levels were associated with a statistically significant increased risk of recurrence among inpatients when adjusted for H2RA use (OR 1.776, 95% CI 1.018 to 3.101, p=0.043), but not when adjusted for PPI use (OR 1.657, 95% CI 0.948 to 2.896, p=0.076).
Multivariate analysis: effect on recurrence of acid suppressants taken at any time during phase 3 studies (mITT inpatients, n=701)
PPI or H2RA use during CDAD-targeted antibiotic treatment by inpatients did not significantly influence time to resolution of diarrhoea (TTROD). The median TTROD was 77 h (95% CI 63 to 101) and 67 h (95% CI 53 to 79) among inpatients who used PPIs and/or H2RAs and did not use them, respectively (figure 2). The difference in TTROD between the two groups was not statistically significant by Kaplan-Meier analysis (p=0.07, log rank test).

{kind=link}
{kind=link}
TTROD among inpatients who did or did not use PPIs or H2RAs concurrently with CDAD-targeted antibiotics. The time from the first dose of study drug to the last dose before resolution of diarrhoea was determined for inpatients who used PPIs or H2RAs (n=423) and those who did not (n=278). Median TTROD was 77 h and 67 h, respectively, for the two groups. Multivariate analysis showed that use of these acid-suppressing drugs did not significantly influence TTROD (p=0.0738, log rank test). CDAD, Clostridium difficile-associated diarrhoea; H2RA, histamine-2 receptor antagonist; mITT, modified intent to treat; PPI, proton pump inhibitor; TTROD, time to resolution of diarrhoea; UBM, unformed bowel movements.
Discussion
Treatment with acid-suppressing drugs such as PPIs and H2RAs has been brought to prominence by the recent safety announcement from the FDA warning the public of an association between PPI use and increased risk of CDAD.22 The FDA Adverse Event Reporting Service (FAERS) and the medical literature provided the basis of this report. In addition to the increased risk of acquiring CDAD, could antacids adversely affect treatment of CDAD or increase risk of recurrences? Our study found that PPI or H2RA use had no effect on clinical response or recurrence; however, fidaxomicin therapy was associated with a 50% reduction in recurrence versus vancomycin. Thus, the concomitant use of PPIs or H2RAs by hospitalised patients treated for CDAD with fidaxomicin or oral vancomycin need not be contraindicated.
Although, in univariate analysis, 24% of inpatients who used PPIs or H2RAs during the follow-up period experienced recurrence, compared with 17% of inpatients who did not use PPIs or H2RAs, multivariate analysis did not detect a significant impact of PPI or H2RA use on recurrence. Instead, other factors dominated. Our data confirm that hypoalbuminemia, elevated serum creatinine and leukocytosis are independent predictors of reduced responses to treatment, regardless of whether or not PPIs or H2RAs are used concurrently with C. difficile-targeted antibiotics. All three conditions have been associated with increased severity of illness in previous studies, so it seems reasonable that they would be related to lower response rates and higher recurrence rates.29–31
The strengths of our study include the large database of patients with CDAD, within which there is a significant inpatient contingent (n=701) that was followed prospectively during the treatment period and 30 days thereafter. Since the analysis only included inpatients, we could confirm that the study drugs were administered as ordered. Other strengths include consistent definitions of clinical response and recurrence, complete collections of safety and efficacy data, and follow-up for 28 days after initial therapy for evidence of recurrence. A weakness is that data are not available for use of acid-suppressing drugs before onset of CDAD, so this study cannot inform the ongoing debate regarding whether these drugs do indeed increase the risk of acquiring the disease. Some studies have found an association between acid-suppressive therapy and recurrence.8–12 While we saw this effect in the univariate analysis when PPIs or H2RAs were used in the follow-up period, this association vanished when the multivariate analysis brought into consideration other confounding factors.
The polemic over the association of PPIs and H2RAs with risk of acquiring CDAD has been controversial in part because of the heterogeneity of studies, some of which have concluded that the association of PPIs and H2RAs with CDAD is epidemiologically based,7 ,32 and others of which have attributed the association to disease severity and lengthy hospital stays.33 ,34 Although it is not our intention to encourage use of PPIs or H2RAs, we have found that such concurrent treatment did not adversely affect CDAD treatment outcomes among inpatients with CDAD. In conclusion, these data support a position that acid suppression therapy, when indicated, can be maintained during treatment of CDAD.
Acknowledgments
This study was presented at the American College of Gastroenterology Annual Scientific Meeting, 28 October–2 November 2011, in Washington DC. Yin Kean (Optimer Pharmaceuticals) provided the statistical analyses. Sally Altman (Optimer Pharmaceuticals), a medical writer, assisted in writing the article. StemScientific (Lyndhurst, New Jersey, USA) provided medical writing and editorial support, sponsored by Cubist Pharmaceuticals.
References
Footnotes
Contributors KW, TL, MAM, KM, and SLG were involved in planning and conducting the study. KW, TL, MAM, KM, DWC, and SLG were involved in collecting and interpreting data, drafting and reviewing the manuscript, and approving of final draft submission.
Funding This study was funded by Cubist Pharmaceuticals, Lexington, Massachusetts, USA (formerly Optimer Pharmaceuticals, San Diego, California, USA).
Competing interests KW has served on an advisory board for and has received research funding as an investigator from Optimer Pharmaceuticals. TL has served on an advisory board sponsored by Cubist Pharmaceuticals. MAM has been an employee of bioMerieux since 1 October 2012. He has also served on an advisory board for and has received research funding as an investigator from Optimer Pharmaceuticals. KM has served on an advisory committee for the protocols and publications involving phase 2 and 3 studies of fidaxomicin. The University of Chicago, where KM is employed, was reimbursed for the cost of conduct of the phase 2 and 3 trials. DWC is supported by the NIHR Oxford Biomedical Research Centre. SLG was an employee of Cubist Pharmaceuticals at the time this manuscript was originally drafted.
Patient consent Obtained.
Ethics approval Both phase 3 trials were approved by independent ethics committees or institutional review boards.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.