Article Text

Abstract
Background Providing structured information for the understanding of hepatic encephalopathy (HE) might be relevant to the prevention and management of the syndrome. The aim of our study was to design a brief, structured educational intervention and evaluate its usefulness in preventing HE-related hospitalisation over time.
Methods Thirty-nine cirrhotic outpatients with a history of HE were enrolled and randomly assigned to an intervention (group A; n=20) or control group (group B; n=19). All of them underwent evaluation of HE (clinical and quantitative neuropsychiatric assessment) and completed the Questionnaire on the Awareness of Encephalopathy. A 15 min educational session was then provided to patients in group A, including basic information on the pathophysiology, hygienic and medical management of HE.
Results No demographic/clinical differences were observed at baseline between the two groups. Similarly, there were no significant differences in HE-related information available at baseline between the two groups; knowledge of HE was limited in both. The intervention was highly effective in increasing patients’ understanding of treatment of the condition (from 5% to 80%). The educational intervention also reduced the risk of developing an episode of HE over a period of 12 months.
Conclusion The educational intervention confirmed the poor knowledge of patients with previous HE about their condition, served as a tool to increase patients’ awareness, and minimised HE-related readmission rates over a period of 1 year.
- cirrhosis
- hepatic encephalopathy
- education
- re-admission
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Patients with a history of hepatic encephalopathy (HE) and their caregivers have limited understanding of HE and its management.
What are the new findings?
The HE educational procedure form (HEEPF), an educational intervention tool designed and tested in this study, increased patients’ awareness and minimised HE-related readmission rates over a follow-up period of 1 year.
How might impact on clinical practice in the foreseeable future?
This study provides pilot data to design and perform a definitive study on the usefulness of HEEPF.
Introduction
It has been estimated that the cumulative risk of recurrence after a first-ever episode of overt hepatic encephalopathy (HE) is nearly 40% over a period of 1 year.1 A retrospective analysis has reported that the readmission rate for HE-related reasons within 1 year is around 40%.2 The total healthcare cost for each HE hospitalisation has increased over the last decade, reaching $37 500 per each HE-related admission.3 Hence, preventing this complication of liver disease after discharge is challenging.4 The American Association for the Study of Liver Diseases/European Association for the Study of the Liver (AASLD/EASL) Practice Guideline4 has emphasised the importance of a multidisciplinary approach where patients, caregivers and practitioners should join to prevent/reduce the incidence of some precipitating factors of HE, such as infections, constipation or dehydration, and avoid subsequent hospitalisations.4 The alliance of both patients and caregivers in the healthcare process has been proved to be effective in the reduction of hospital admissions in other diseases.5 6
In a recent study, we have observed that both patients and their caregivers have limited understanding of the disease/its management, and we have suggested that this may be the consequence of insufficient provision of information.7 Therefore, providing structured information for the understanding of HE might be relevant to its prevention and management. Based on this hypothesis, the aims of this study were: (1) to test the awareness of HE in a group of patients who had had a previous episode of HE≥grade II; (2) to validate a short educational procedure for these patients; (3) to provide a preliminary assessment of the efficacy, if any, of an educational intervention to prevent HE-related hospitalisation (HE≥grade II) over time by a prospective randomised intervention study.
Patients and methods
Participants
A total of 39 consecutive outpatients referred to the Internal Medicine/Regional Centre for Liver Diseases of the Department of Medicine of Padova University Hospital were enrolled. The aetiology of cirrhosis was established based on clinical, laboratory, radiological, and histological indices. Its severity was determined using the Child-Pugh8 and Model for End-stage Liver Disease (MELD)9 scores. All patients had had at least one previous episode of overt HE (≥grade II).10
Patients were excluded if they were under 18 years of age, had misused alcohol in the preceding 6 months, had a history of head injury, cardiovascular/cerebrovascular disease, neurological/psychiatric comorbidity, were taking psychoactive drugs or were unable/unwilling to comply with the study procedures. A total of 12 outpatients declared they had habitual caregivers who were relatives.
Experimental design and structured educational intervention
The study was planned to be completed in 2 years and had a prospective randomised intervention design. Over this period of time, we were able to enrol 39 outpatients with cirrhosis, who were randomly assigned to one of two groups (by random numbers generated from a computer): group A, undergoing the educational intervention (n=20), and group B, not undergoing the educational intervention and serving as controls (n=19).
Before starting the intervention, all participants underwent a neuropsychological and neurophysiological assessment (vide infra) and filled in the Questionnaire on the Awareness of Encephalopathy (QAE), which was designed by our research group in 2012 and is fully described elsewhere.7
The educational intervention was based on commenting three cartoons (HE educational procedure form (HEEPF)) including: (1) basic information on the pathophysiology of HE; (2) education on how to ensure/maintain regular bowel emptying; and (3) drugs used to treat HE with a simple explanation of their mechanism of action, pharmacological and commercial names (figure 1). The educational intervention was planned to be completed in approximately 15 min. The intervention was designed with a view to inform/educate the patient on manoeuvres and decisions that can be made without the intervention of a doctor, thus changes in the dose of diuretics and introduction/tapering of psychoactive drugs were not covered.

Hepatic encephalopathy educational procedure form.
Within 1 hour of the educational intervention, patients completed a questionnaire designed to check if they were satisfied with the information received and if they had acquired novel information (Novel Information Questionnaire (NIQ)) (table 1).
Novel Information Questionnaire
Both the HEEPF and the NIQ were designed for purposes of this specific study, and they are presented and described in table 1 and figure 1, respectively.
Baseline neuropsychiatric assessment
At the moment of recruitment, all the patients underwent a clinical assessment, including full neurological examination and a clinical grading of the neuropsychiatric abnormalities, if any, according to the West Haven criteria.10
Neuropsychological evaluation
Paper and pencil psychometry
Psychometric performance was assessed, under standardised conditions, using Number Connection Tests A and B, the Digit Symbol subtest of the Wechsler Adult Intelligence Scale, and the Line Tracing and Serial Dotting tests.11 Individual test results were scored in relation to age-adjusted and education-adjusted Italian norms.12 Performance was classified as impaired if the rounded sum of the adjusted SD from the norms for the individual tests, known as the Psychometric Hepatic Encephalopathy Score (PHES), was ≤−4.12
Sternberg task
A computerised version of the Sternberg paradigm test was also administered.13 Thirty-six consecutive pairs of numbers, with or without common digits, were presented on a computer screen, and subjects were asked to press 1 on the keyboard if there were common digits (ie, 5632 and 694) and press 3 if there were no common digits (ie, 41 and 75). Both accuracy (% correct responses) and reaction times (ms, adjusted for accuracy) were obtained. Finally, an overall age-adjusted and education-adjusted z score was obtained, with reference to local normative values.
Neurophysiological evaluation
Electroencephalograms (EEG) were recorded for 10 min, eyes closed, in a condition of relaxed wakefulness, using a 21-electrode EEG cap (ground: Fpz; reference: Oz; impedance <5 kΩ). Each channel had its own analogue-to-digital converter; the resolution was 0.19 μV/bit (Brainquick 3200, Micromed, Mogliano Veneto, Italy). One continuous 80–100 s period of artefact-free EEG tracing was selected for spectral analysis; the following parameters were obtained: mean dominant frequency (MDF, expressed in Hz), which is an estimate of the background frequency of the EEG, and relative power of the spectral bands delta, theta, alpha and beta, expressed as percentages (%). EEGs were classified according to Amodio et al. 14
On the day of study, patients were qualified as being neuropsychiatrically unimpaired (normal on clinical assessment, normal PHES and normal EEG) or as having covert HE (≤grade I on clinical assessment,10 abnormal PHES and/or EEG) or overt HE (>grade I on clinical assessment).10
Follow-up
Patients were telephoned monthly for 12 months, and they were asked if they had had HE-related admissions. Information was verified, where possible, on clinical notes and hospital records.
Ethics
The study was approved by the Padova University Hospital Ethics Committee, and all participants provided written, informed consent. The study was conducted according to the Declaration of Helsinki (Hong Kong Amendment) and Good Clinical Practice (European) guidelines.
Statistical analysis
Demographic, clinical and neuropsychiatric variables distributions were tested for normality using the Shapiro-Wilk’s test. Differences between groups were performed by the Student’s t-test/Mann-Whitney U test, as appropriate. Analysis of the effectiveness of the educational intervention was performed using the Fisher’s exact test for proportions. Survival analysis was performed using both monovariate (Kaplan-Meier) and multivariate models (Cox’s regression). Incidence was expressed as the number of events per year per 100 patients. The sum of the follow-up for each event to occur was computed. Then, the sum of the events and the sum of the observation time for the events to occur was computed. This value was normalised for 1 year and for 100 patients.
Results
Demographic and baseline assessment parameters are presented in table 2. There were no significant differences between groups A and B in any of the demographic, hepatic failure, neuropsychological and neurophysiological variables. Similarly, there were no significant differences between groups A and B in QAE results. In detail, 30 of the 39 patients (77%, 95% CI 62 to 87) were aware of previous HE, 16 in group A (80%, 95% CI 58 to 92) and 14 in group B (74%, 95% CI 51 to 88). However, only three patients in group A (15%, 95% CI 5 to 36) and two in group B (11%, 95% CI 3 to 31) were able to correctly identify the medication used to treat/prevent HE. Furthermore, only one patient in group A (5%, 95% CI 1 to 24) and two in group B (11%, 95% CI 3 to 31) had adequate understanding of the expected treatment effects.
Demographic, clinical, neuropsychological and EEG variables by group. No significant differences were observed between groups A and B in any of these variables
Twelve (60%, 95% CI 39 to 78) patients in group A declared they were satisfied with the HEEPF and 11 (55%, 95% CI 34 to 74) had actually acquired novel information on the pathophysiology of HE. Of the eight (40%, 95% CI 22 to 61) patients who declared that the intervention had not been useful to them, one (5%, 95% CI 1 to 24) already had adequate information at baseline, five (25%, 95% CI 11 to 47) had not actually acquired new knowledge on their condition, and 2 (10%, 95% CI 3 to 30) had acquired new knowledge on their condition despite declaring the opposite. Thus, in 13 (65%, 95% CI 43 to 82) patients the intervention provided novel information and 14 (70%, 95% CI 48 to 85) had adequate knowledge at the end of the educational procedure.
In relation to prevention/treatment of HE, 16 patients (80%, 95% CI 58 to 92) belonging to group A declared they had received novel information, and 4 (20%, 95% CI 8 to 42) declared they had not. Out of these four, one (5%, 95% CI 1 to 24) already had the information at baseline, and 3 (15%, 95% CI 5 to 36) had not actually acquired new information on prevention/treatment of HE, despite the HEEPF. Thus, the intervention was highly effective in increasing expertise on HE management, improving knowledge from 5% (95% CI 1 to 24) preintervention to 80% (95% CI 58 to 92; p<0.001, Fisher’s exact test) postintervention in group A.
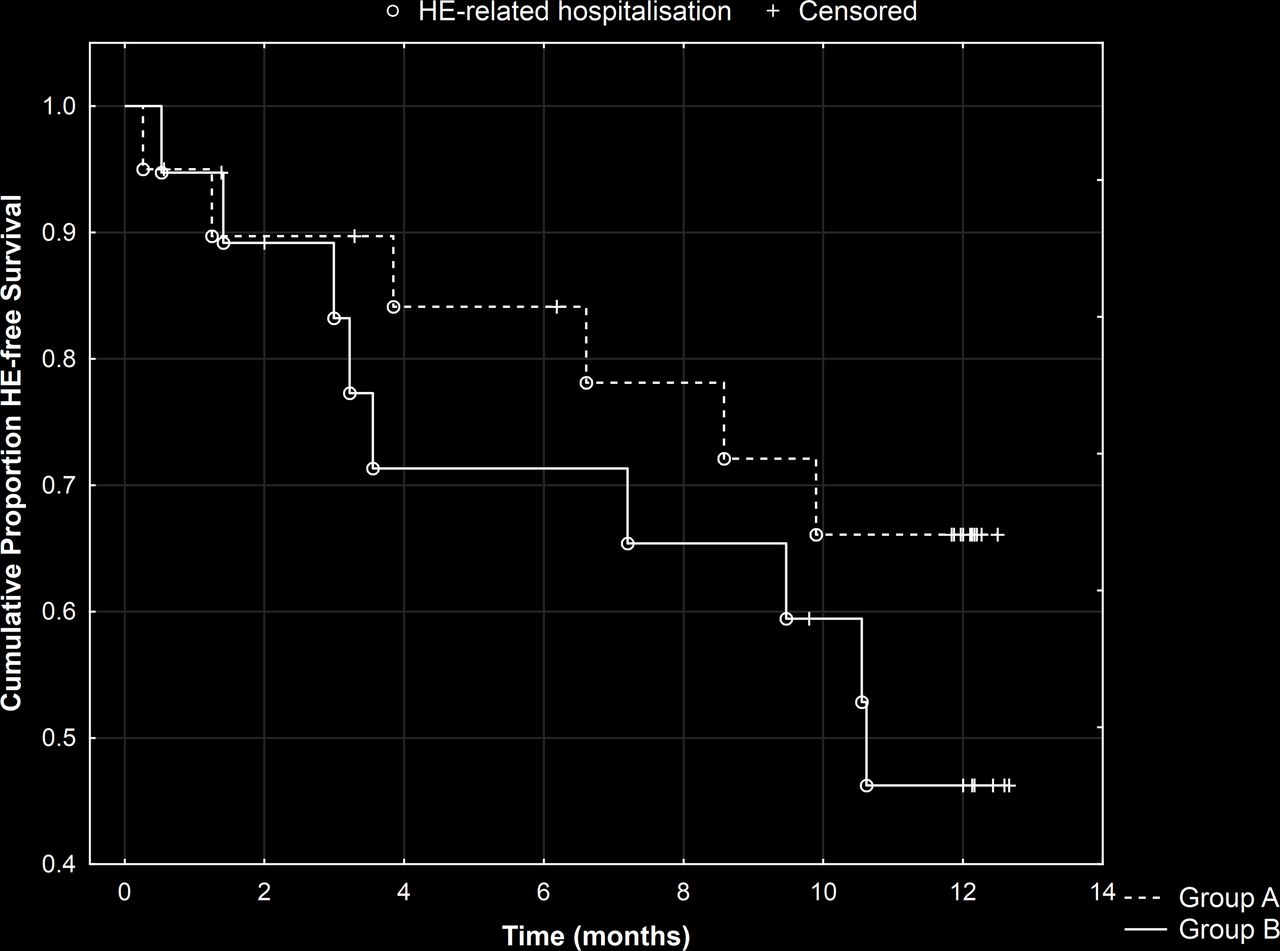
During the 12-month follow-up period, patients in groups A and B suffered a total of 6 and 9 episodes of HE≥grade II requiring hospitalisation, respectively. The precipitating causes of HE were infection (n=2), dehydration (1), constipation (1) and unknown (2) in group A, and infection (3), constipation (2), and unknown (4) in group B.
The incidence of events was 20.8×100 patients × year versus 48.8×100 patients × year in groups A and B, respectively (figure 2). These results allow us to estimate that about 80 subjects would have been required to reach 80% power.
{kind=link}
{kind=link}
Cumulative proportion of HE-free patients over time by group (A=intervention; B=no intervention). The risk of HE-related hospitalisation in group A was HR=0.58 (95% CI 0.21 to 1.62; p=0.29). HE, hepatic encephalopathy.
Older age, poor liver function and poor psychometric performance (abnormal PHES) were associated with increased risk of HE-related hospitalisation, while fast EEG activity was associated with reduced risk of HE-related hospitalisation (table 3).
Monovariate analysis showing the association between age, liver function (MELD), abnormal PHES and EEG mean frequency (MDF) with the risk of developing HE-related hospitalisation
By using multivariate backward Cox’s model to adjust for these variables, which reflect the severity of the patients’ clinical condition and may have acted as confounders, the educational intervention was shown to reduce the risk of HE-related hospitalisation over the follow-up period (HR=0.14, 95% CI 0.02 to 0.77, p=0.02).
Discussion
A structured educational session (HEEPF) providing information on HE pathophysiology, prevention and medical treatment was designed, with a view to help preventing HE-related hospitalisations. The usefulness of such programme was immediately evaluated by means of NIQ, and over the subsequent 12 months by a monthly telephone interview, to check for the occurrence of HE-related hospitalisations.
After the intervention, 70% of patients had acquired new information about the pathophysiology of HE, and 80% of them had improved their knowledge about HE prevention/treatment. These findings highlight two issues: (1) the limited awareness of these patients about their condition, which is in line with a previous report7 and (2) the need to strengthen the communication between patients and physicians, at least within the context of the Italian healthcare system. In other diseases, educational approaches have been shown to enhance patients’ personal understanding, to improve long-term control of the disease, and also to improve evidence of the usefulness of pharmacological treatment.15–18
Importantly, when the results were corrected for the severity of the clinical condition, HEEPF was shown to reduce the risk of HE recurrence over time. This was despite the high absolute number of HE events over the follow-up period. Although well-informed patients in group A could have avoided precipitant factors such as constipation or dehydration, factors such as infection or bleeding are obviously more difficult to prevent/control. Nonetheless, the number of ‘avoidable’ precipitants in both groups was similar. The fact that the AASLD/EASL Practice Guideline on HE4 strongly encourages definition and recording of HE precipitants may help with similar studies in future, by way of clearer and better information in this respect in notes/medical records.
In addition, the AASLD/EASL Practice Guideline4 highlights the importance of the education of both patients and their relatives/caregivers. Caregivers have a crucial role in the healthcare process once the patient is discharged,4 hence new tools are being designed to help them detect episodes of HE.19 Similarly, the HEEPF could have been administered to both patients and their caregivers, or even only to caregivers. Indeed, one of the initial aims of the present study was to involve caregivers. However, very few patients were accompanied on the day of study, making enrolment impossible.
Altogether, the improved awareness/understanding of HE by use of a single, quick (15 min) educational intervention (HEEPF) constitutes preliminary evidence of its usefulness. The tool is cheap, user-friendly, and can be administered by trained nursing staff to improve patients’ self-management (and possibly pharmacological treatment) so that HE-related readmission rates can be reduced. This has considerable consequences, as poor understanding of HE/its management among patients may also impinge on the likelihood of demonstrating the efficacy of treatments in future. In conclusion, the present study:
confirms limited disease awareness in patients with a history of HE
proposes a simple and short educational procedure (HEEPF) that is effective in increasing awareness, and most likely also in reducing readmission rates
provides pilot data to design and perform a definitive study on the usefulness of HEEPF. Future research is also needed to characterise the features (ie, precipitants and others) of the HE with the highest likelihood of benefiting from the educational approach in terms of prevention.
References
Footnotes
Contributors MT, CF, MC, MDR and SM assessed the patients and performed the study. MG, CF, SM and PA analysed the data and drafted the manuscript. SM and PA designed and planned the study. SM is responsible for the overall content as guarantor.
Funding The work was partly funded by a grant from the Italian Ministry of Health to SM (Giovani Ricercatori 2009-1604309); MG was funded by a research postdoctoral fellowship from Gobierno de Extremadura (jointly financed by the European Regional Development Fund (ERDF); ref. PO14013).
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Padova University Hospital Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.