Article Text

Abstract
Objective A clinical diagnosis of bile acid malabsorption (BAM) can be confirmed using SeHCAT (tauroselcholic (75selenium) acid), a radiolabelled synthetic bile acid. However, while BAM can be the cause of chronic diarrhoea, it is often overlooked as a potential diagnosis. Therefore, we investigated the use of SeHCAT for diagnosis of BAM in UK hospitals.
Design A multicentre survey was conducted capturing centre and patient-level information detailing patient care-pathways, clinical history, SeHCAT results, treatment with bile acid sequestrants (BAS), and follow-up in clinics. Eligible data from 38 centres and 1036 patients were entered into a validated management system.
Results SeHCAT protocol varied between centres, with no standardised patient positioning, and differing referral systems. Surveyed patients had a mean age of 50 years and predominantly women (65%). The mean SeHCAT retention score for all patients was 19% (95% CI 17.8% to 20.3%). However, this differed with suspected BAM type: type 1: 9% (95% CI 6.3% to 11.4%), type 2: 21% (95% CI 19.2% to 23.0%) and type 3: 22% (95% CI 19.6% to 24.2%). Centre-defined ‘abnormal’ and ‘borderline’ results represented over 50% of the survey population. BAS treatment was prescribed to only 73% of patients with abnormal results.
Conclusions The study identified a lack of consistent cut-off/threshold values, with differing centre criteria for defining an ‘abnormal’ SeHCAT result. BAS prescription was not related in a simple way to the SeHCAT result, nor to the centre-defined result, highlighting a lack of clear patient care-pathways. There is a clear need for a future diagnostic accuracy study and a better understanding of optimal management pathways.
- BILE ACID
- MALABSORPTION
- IMAGING
- DIARRHOEA
- IRRITABLE BOWEL SYNDROME
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Summary box
What is already known about this subject?
▸ Bile acid malabsorption (BAM) is an established cause of chronic diarrhoea and results in significantly adverse quality of life for affected individuals.
▸ Diagnosis of BAM can be confirmed using SeHCAT (tauroselcholic (75selenium) acid), a radiolabelled synthetic bile acid. However, this diagnostic tool is not consistently applied in National Health Service (NHS) centres in the UK.
▸ Patients diagnosed with BAM can benefit from the prescription of bile acid sequestrants (BAS); however, there is known poor patient-reported adherence with BAS treatment.
What are the new findings?
▸ There was a high level of heterogeneity in practice, with no standardised protocol, and no consistently defined diagnostic threshold values of SeHCAT retention.
▸ Suspected BAM type 1 patients had the highest proportion of centre-defined abnormal results.
▸ Prescription of BAS was inconsistent across patient groups, with notable numbers of patients with low SeHCAT retention or centre-defined ‘abnormal’ results apparently not receiving BAS.
▸ The majority of patients who were prescribed BAS reported improvement in clinical symptoms of diarrhoea severity, pain, urgency or bloating, highlighting the importance of identifying patients who may benefit from BAS.
▸ Colesevelam is frequently prescribed as treatment for BAM, although not licensed for this purpose in the UK.
How might it impact on clinical practice in the foreseeable future?
▸ Participating centres varied in their interpretation of SeHCAT results with various cut-off/threshold values. As this impacts on subsequent patient treatment, we strongly recommend that a standardised threshold value be established for the UK.
▸ The survey brings attention to the variable prescription of BAS without clear patient care pathways, which needs to be addressed at a national level.
Introduction
Chronic diarrhoea is a commonly cited reason for referrals to secondary and tertiary care gastroenterology departments.1 ,2 Patients who present with chronic diarrhoea often undergo a multitude of investigations, which do not necessarily result in a diagnosis. As the prevalence of chronic diarrhoea is estimated to be 4–5% of adult Western populations, this places a significant cost burden on health systems such as the National Health Service (NHS), as well as impacting detrimentally on the quality of life of affected patients.3–5 Bile acid malabsorption (BAM) is a frequent cause of chronic diarrhoea.
Owing to lack of clinician awareness or access to appropriate investigations, BAM may be overlooked and patients left with incorrect diagnoses such as diarrhoea-predominant irritable bowel syndrome (IBS-D).4–9 Furthermore, robust data on the prevalence of primary and secondary BAM do not exist.
BAM is categorised into three types: type 1 is defined as BAM resulting from ileal resection or ileal inflammation (eg, in Crohn's disease), type 2 is defined as primary or idiopathic and type 3 is defined as secondary to, or associated with, various gastrointestinal diseases or conditions such as IBS, postcholecystectomy, chronic pancreatitis, coeliac disease and diabetes mellitus.4 ,7 ,10 With recent key discoveries about the underlying pathophysiology, this condition is increasingly (and more accurately) also termed bile acid diarrhoea (BAD) as true malabsorption is not always present, especially in type 2.11
Confirmation of a clinical diagnosis of BAM can be made using SeHCAT (tauroselcholic (75selenium) acid), a radiolabelled synthetic bile acid.1 ,3 ,12 ,13 The SeHCAT test was introduced in the UK in 1981; however, it is underutilised in the UK owing to various factors, such as the lack of guidance on its role as a diagnostic tool, and the practice among some clinicians of diagnosing BAM (or BAD) by trial of bile acid sequestrant (BAS) treatment (without the use of SeHCAT) among those with chronic diarrhoea.3 ,11 However, there is no evidence base for this practice. Furthermore, SeHCAT is not licensed in many countries, for example the USA.14
The SeHCAT test involves measuring the retention of radioactivity in the patient following administration of a capsule containing SeHCAT.3 ,15 The patient is scanned 1–3 hours after taking the capsule, and this is repeated (ideally) after 7 days to measure retention of the radiolabelled bile acid. Low SeHCAT retention at day 7 represents an abnormal result and, therefore, a positive diagnosis of BAM. There is no set cut-off threshold established for the UK, although retention values of <5% (or up to <10% or <15%) are generally considered to be abnormal.3 ,4 SeHCAT results are occasionally used to grade the severity of BAM, for example <5% retention indicative of arbitrarily ‘severe’ BAM, between 5% and 10% retention as ‘moderate’ BAM and between 10% and 15% retention as ‘mild’ BAM.3 However, these severity grades, much like the cut-off thresholds, are not standardised or validated.
Patients with a confirmed or suspected clinical diagnosis of BAM may be offered treatment with BASs.2–4 ,7 ,12 ,13 ,16–18 BAS treatments such as colestyramine and colestipol may be empirically offered in the UK to patients with chronic diarrhoea as a trial of treatment for suspected BAM. These treatments are known to have poor adherence due to their unpleasant taste and texture,5 ,14 ,19 and response rates can vary depending on the patient population.4 Constipation and other gastrointestinal side effects are commonly reported.10 ,19 ,20 A newer BAS treatment, colesevalam, is available in tablet form, avoiding the unpleasant taste and texture, which may result in higher adherence in comparison to the other BAS that come in a granule formulation suspended as a resin in water.19 ,21 However, colesevalam, although promoted as an alternative BAS7 ,16 ,22–24 because it may be more effective in binding to bile acids, is not licensed in the UK for treatment of BAM.14 ,21
There is also evidence that response to BAS treatment is related to the result of the SeHCAT test,1 ,7 ,10 ,12 ,25 ,26 with authors suggesting that BAS prescription should be targeted to certain patient populations depending on their SeHCAT-informed BAM diagnosis.
The UK National Institute for Health and Care Excellence (NICE) published Diagnostic Guidance (DG7)3 on SeHCAT for the investigation of diarrhoea caused by BAM in people diagnosed with IBS-D or Crohn's disease without ileal resection. DG7 concluded that there were potential patient and system benefits from using SeHCAT for the diagnosis of BAM. However, the guidance went on to note that insufficient evidence existed to determine whether or not SeHCAT was a cost-effective diagnostic option, and, therefore, a programme of research was recommended.
Kings Technology Evaluation Centre (KiTEC), an External Assessment Centre funded by NICE, was commissioned to address the research questions in DG7 through a series of multidisciplinary studies: a retrospective audit, a prospective survey and a diagnostic accuracy study.13 ,27–29 The prospective survey is presented here (the second of the study series) and aimed to describe the day-to-day practice associated with the clinical indications for referring patients for a SeHCAT test in NHS centres. These data will inform future diagnostic and treatment pathways by providing the necessary background information for the design of the final study in this series, which will assess specifically the research questions posed in DG7.
More specifically, the service evaluation reported in this paper aimed to characterise the variability in centre practice and procedures, patient clinical history, SeHCAT test results and treatment including BAS prescriptions rates.
Methods
A prospective survey was designed to capture relevant data (including patient referral, symptom history, SeHCAT scan technique, results and clinical follow-up) related to the SeHCAT test performed on each eligible patient. A pilot phase ran during February and March 2014. The full prospective survey was launched in March 2014, and patient recruitment was open from March 2014 until August 2015. The survey was developed in consultation with members of a Clinical Advisory Board (CAB) (see appendix).
Inclusion criteria
NHS centres were recruited through a variety of methods, including direct emails to all centres listed on a SeHCAT database provided by the British Nuclear Medicine Society (BNMS), based on the work of Smith and Perkins,30 contact with members of the CAB and notices on the BNMS and British Society of Gastroenterology (BSG) websites.31 ,32 Formal commitments to participate were obtained from a consultant gastroenterologist and the Nuclear Medicine department at each centre. A total of 40 centres registered to participate in the survey (see Acknowledgments section for the participating centres).
Any patient referred for a SeHCAT test with a clinical suspicion of BAM because of chronic diarrhoea without a known cause was eligible for inclusion in the prospective survey. It was a requirement that the patient had at least one of their SeHCAT scans (day 1 or day 7) during the survey period, even if they were referred for the test prior to the start of the survey. Formal ethical approval and individual patient consent were not required for the survey, as it was an evaluation of practice and did not require any change to normal clinical practice.
Data collection and testing
Survey data were entered by NHS staff (such as gastroenterologist or nuclear medicine technicians) into a validated data management system, MedSciNet. Data were collected either during patient consultations (eg, patient symptoms) or from patient notes (eg, SeHCAT results). A pilot survey was conducted in five NHS centres (see Acknowledgments section) by collecting data for a sample of SeHCAT procedures. The feasibility, acceptability and availability of the tool to capture the relevant data were also tested. The pilot ran for 3 weeks (17 February to 7 March 2014). Feedback was collected, and this was used to optimise the proposed data collection strategy. Data collected in the pilot survey were deemed to be of sufficient quality to be added to the full prospective survey.
Statistical analysis
Data analysis was descriptive with appropriate summary statistics (means, medians, SDs, percentages, 95% CIs) and performed using SPSS (V.21) and Microsoft Excel (V.14).
Results
Centre overview
In total, 38 centres agreed to participate and contributed data to the SeHCAT survey (see online supplementary figure S1). The total number of SeHCAT investigations undertaken by the participating centres in the 6 months of the survey was 1070.
supplementary figures
Participating centres had been providing a routine SeHCAT service for a median of 13 years (range: 1–33 years). The majority of centres (68%, n=26/38) reported providing a service for 10+ years while 29% (n=11/38) of centres had been providing the service for 20+ years. Thirteen per cent of centres (n=5/38) reported providing a routine SeHCAT service for <5 years.
Centre-defined threshold values for the SeHCAT retention results were reported by 32 centres, and followed two main patterns, using either three categories (normal, borderline or abnormal, n=25) or four categories (normal, mild, moderate or severe/abnormal, n=7). Threshold values for ‘normal’ ranged from ≥10% to ≥20% retention. The majority of centres (69%, n=22/32) reported a ‘normal’ cut-off of ≥15%. Threshold values for ‘borderline’ ranged from a lower value of 5–15% to a higher value of 10–19%. Threshold values for ‘abnormal’ were all recorded from 0% retention with an upper limit between 4% and 14%. Centres (n=7/32), which reported across four categories (normal, mild, moderate and severe/abnormal), were very similar in cut-off values. All but one of these centres reported the following: normal (≥15%), mild (10–14.9%), moderate (5–9.9%) and severe/abnormal (0–4.9%).
Follow-up in clinics was not routinely conducted in 24% (n=9/38) of centres, with a common statement that the final report is usually sent back to the referrer (ie, internal consultant or external centre). The main source of SeHCAT test funding for centres was from outpatient appointments (74%, n=28/38), and 34% (n=13/38) of centres reported that the cost of SeHCAT was included in bundle of care.
In 42% of centres (n=16/38), the Se-75 high-energy peak (264 keV/279 keV approximately) window was used during the first scan, while 52% of centres (n=20/38) responded that they used a different approach. Of these, n=11/20 centres reported using the Se-75 high-energy peak (∼264 keV/279 keV) and the Se-75 low energy peak (∼137 keV) windows. Centres also elaborated on the use of SeHCAT equipment and patient positioning procedures (see table 1).
SeHCAT equipment and patient positioning procedures
Patient clinical information
A total of 1036 eligible patients (n=34 patients did not meet inclusion criteria) were entered into the SeHCAT survey database, each of whom had a SeHCAT scan during the period of the survey (see table 2 for their demographic characteristics and online supplementary figure 1 for patient recruitment). The suspected BAM type based on clinical indications was provided for 752 patients, prior to undertaking the SeHCAT test. Type 1 was the smallest group (14%, n=107/752), followed by type 3 (41%, n=310/752) and then type 2 (45%, n=335/752). The majority of patients had undergone multiple diagnostic tests since symptoms began, such as blood tests, stool tests and colonoscopies.
Demographics and background information
Details of patients' clinical symptoms were collected prior to the first SeHCAT scan (see online supplementary table S1). Patients across all suspected BAM types reported high levels of diarrhoea (three or more times per day), bloating and nocturnal diarrhoea. Using the Bristol Stool Chart as a guide, 92% of patients (n=555/603) reported that their main type of stool produced in a typical week was diarrhoeal in nature (stool types 5, 6 or 7).
supplementary tables
First and second SeHCAT scans
Each patient received an initial scan following administration of the SeHCAT capsule, and a follow-up scan usually scheduled for 1 week later. The time between the first and second scan was exactly 7 days for 99% of patients (n=1007/1021). The time between administration of the SeHCAT capsule and initial scan ranged from 8 to 339 min, with a mean of 187 min (SD: 50). For the majority of patients, there was no modification to food or drink prior to the scans (first scan: 66%, second scan: 81%). The next largest categories were fasting overnight (before first scan) and having a light breakfast (before second scan). For most patients (almost 90% for both scans), there was no modification of medication prior to the scans.
The distance between the patient's stomach or back and the detector was highly variable for both scans. This is likely to reflect the difference in position of the patient during the scan (eg, prone vs sitting). The mean estimated time required to perform each scan was 9.3 min (SD: 5.3), and the duration ranged from 1.7 to 30 min.
SeHCAT results
SeHCAT retention scores were provided for 824 patients of the 1036 eligible patients. The retention scores were positively skewed with a peak towards lower retention and an overall mean retention score of 19% (95% CI 17.8% to 20.3%, median=15%). The percentage SeHCAT retention differed with suspected BAM type: type 1 had a mean retention of 9% (95% CI 6.3% to 11.4%), the mean for type 2 was 21% (95% CI 19.2% to 23.0%), and the mean for type 3 was 22% (95% CI 19.6% to 24.2%) (figure 1).

SeHCAT retention by suspected BAM types: box and whisker plots. Circles represent outliers. BAM, bile acid malabsorption; SeHCAT, tauroselcholic (75selenium) acid.
Fifty per cent of patients (n=412/824) had a SeHCAT retention score of <15%, and 24% (n=196/824) had a score of <5%. The breakdown of SeHCAT retention scores in 5% bands by the BAM type is shown in table 3. Around 60% of suspected BAM type 1 patients had a SeHCAT retention of <5%, while a similar percentage of suspected BAM types 2 and 3 had retentions of 15% or more.
SeHCAT results and centre-defined results by suspected BAM type
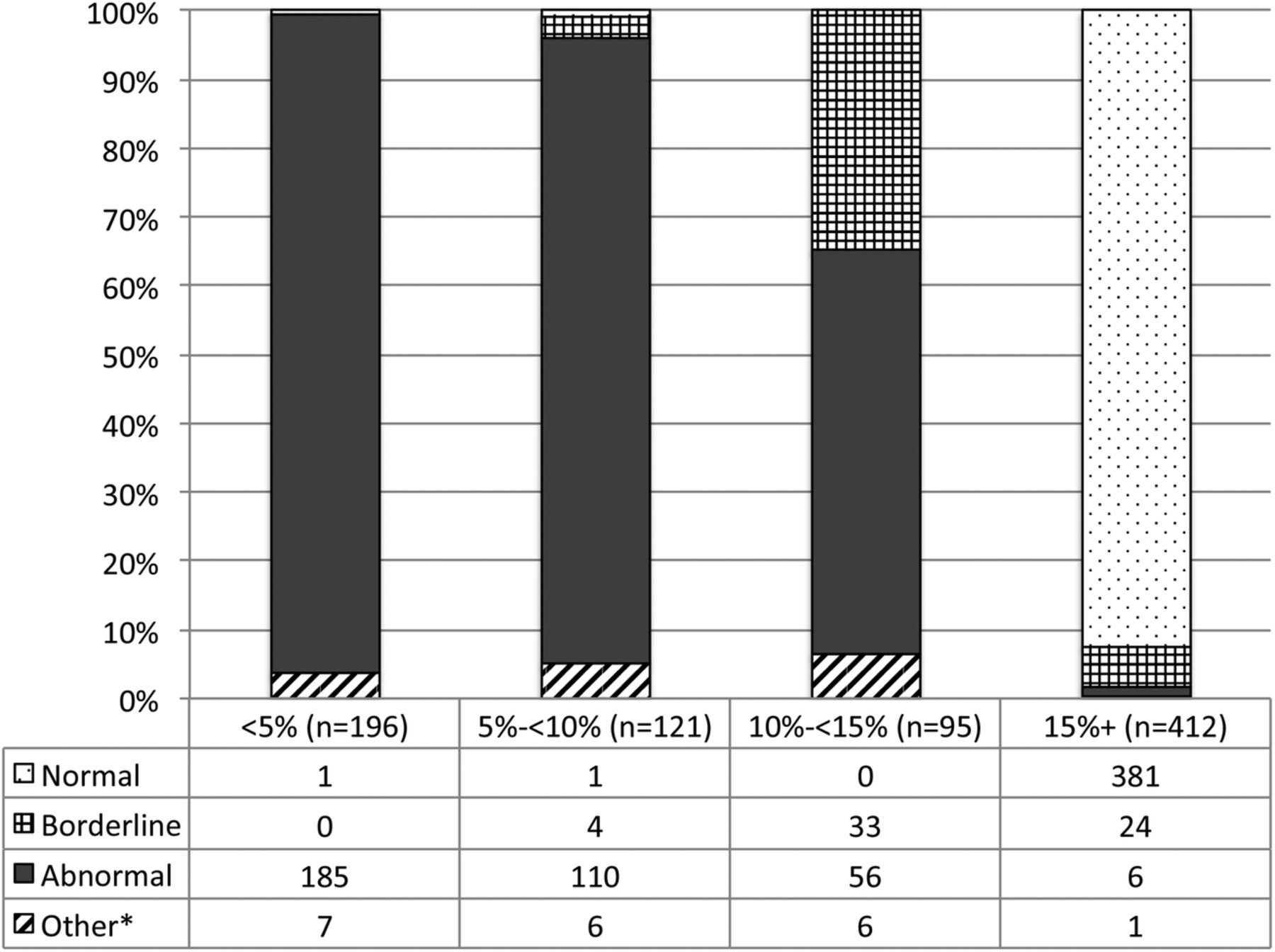
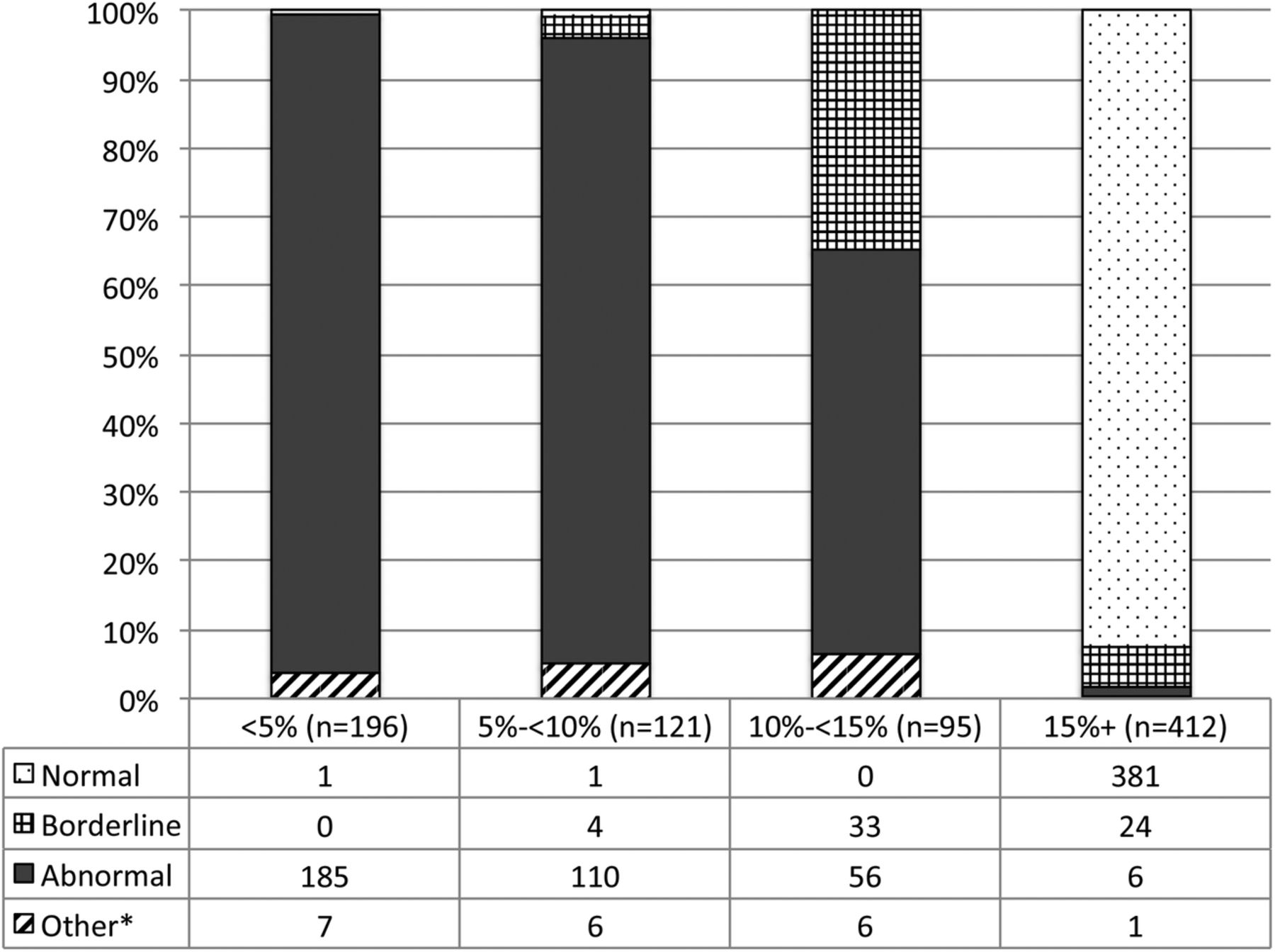
Forty-three per cent (n=358/828) of patients had a centre-defined ‘abnormal’ result, with 7.5% (n=62/828) defined as ‘borderline’ and 47% (n=388/828) defined as ‘normal’. Suspected BAM type 1 had the lowest overall ‘normal’ result of 21% (n=22/107), whereas suspected BAM types 2 and 3 had a higher proportion of ‘normal’ results, with 54% and 53%, respectively (n=177/329 and n=162/308). Of patients with <5% SeHCAT retention, 96% (n=185/193) had a centre-defined ‘abnormal’ result, as did 91% (n=110/121) of those with a SeHCAT retention of 5% to <10% (figure 2). For patients with a SeHCAT retention of 15% or more, 92% (n=381/412) had a centre-defined ‘normal’ result (figure 2). Those patients whose SeHCAT retention score lay in the range 10% to <15% were divided between the ‘abnormal’ (59%, n=56/95) and ‘borderline’ (35%, n=33/95) centre-defined categories.
{kind=link}
{kind=link}
SeHCAT retention result by centre-defined result. *Other often described as ‘severe BAM’ or ‘moderate BAM’. BAM, bile acid malabsorption; SeHCAT, tauroselcholic (75selenium) acid.
Treatment and follow-up
Overall, BAS was reported as being prescribed to 37% of patients post-SeHCAT (n=265/717). Prescription of BAS was most frequent among suspected BAM type 1 patients (56%, n=55/98) compared to BAM types 2 and 3 (34% and 33%, respectively). Patients with a SeHCAT retention of <5% or between 5% and 10% were prescribed BAS in 72% (n=123/172) and 76% (n=78/102) of cases, respectively. BAS was prescribed to 73% (n=117/161) of patients with a centre-defined abnormal result.
The SeHCAT survey captured additional outpatient follow-up information for two patient groups: 140 patients who were prescribed BAS treatment, and 200 patients who were not prescribed BAS, regardless of their SeHCAT result.
Among patients followed-up, colestyramine was the main type of BAS prescribed (70%, n=96/138), and this was the favoured treatment regardless of suspected BAM type or SeHCAT retention result (see online supplementary table S2). A second line of BAS treatment was prescribed for 18% (n=22/119) of patients. Patient-reported adherence to BAS prescription was 76% (n=77/101) for all patients followed-up. Among those prescribed BAS, 21 reported side effects from the BAS treatment.
A reduction in the severity of diarrhoea symptoms (moderate to complete cessation) was reported by 71% (n=63/89) of patients, since beginning BAS treatment (see online supplementary table S3). Reduction (moderate to complete cessation) in the severity of several symptoms was reported by patients after the start of BAS treatment: reduced pain associated with symptoms by 42% (n=28/53); reduced frequency of urgency associated with symptoms for 69% (n=50/73); and reduced severity of bloating for 46% (n=23/49).
Patients described their experience with BAS, with some reporting further gastrointestinal symptoms:a lot of improvement but not total cure
very good, a vast improvement
feeling bloating and windy
not nice to take due to taste and bloating
difficult to take granules
did not like Colestyramine at all. Tolerated Colesevalam better.
Among followed-up patients not prescribed BAS (n=200), the majority reported no change post-SeHCAT in the severity of diarrhoea symptoms (69%, n=108/157), severity of pain (82%, n=104/127), frequency of urgency (81%, n=102/124) and severity of bloating (87%, 107/123) (supplementary table 3).
Adverse events
Adverse events were only reported by one centre in the survey. Twenty-eight patients had a single adverse event, and five patients had two adverse events, resulting in 38 adverse events in total. Some of the adverse events were recorded as being a result (n=5/38) or likely/possibly result (n=20/38) from the SeHCAT test itself. For the eight patients who reported severe side effects, these were described in free text fields as:Bloated, rough back of throat, sweaty/sick
Bloating (but after a meal)
Diarrhoea, sickness & stomach cramps
Vomiting, bad stomach pain.
Discussion
The main aim of this prospective survey was to describe the day-to-day practice associated with the clinical indications for referring patients for a SeHCAT test, and their subsequent management, in order to inform future diagnostic and treatment pathways. Recruitment exceeded expectations for the number of centres (38 centres contributed data) and eligible patients (n=1036). Centres described their procedures for referrals, funding and equipment related to SeHCAT.
This study was designed as a service evaluation, and so it was not possible to undertake additional patient follow-up where this was not normal clinical practice. Hence, there were no follow-up data for 24% of centres that did not routinely follow-up patients themselves.
One key finding was that centres varied widely in their interpretation of SeHCAT results with differing cut-off/threshold values. This is consistent with previous findings.3–5 For example out of 32 centres, 25 reported using three categories of ‘normal’, ‘borderline’ and ‘abnormal’ while seven used four categories of ‘normal’, ‘mild’, ‘moderate’ and ‘severe/abnormal’. Among the former, over 90% of SeHCAT results showing <10% retention had been graded as ‘abnormal’ by centres, and similarly over 90% of SeHCAT results of 15% of more were graded as ‘normal’. Notably, patients with a retention score between 10% and 15% were classified differently by different centres, with 59% defined as abnormal and 35% defined as borderline. These inconsistent threshold values may be impacting on subsequent patient treatment and, in common with previous authors,4 we therefore recommend that a standardised threshold value be established for the UK. This will require a prospective diagnostic accuracy study, including consistent and standardised methodologies between participating centres collected alongside prospective data about therapeutic responses to BAS in order to set a validated and clinically useful threshold value or range. Parallel evaluation of other markers of bile acid handling such as faecal bile acids would also be valuable. Such a study has already been designed with a detailed protocol available.13
The mean overall SeHCAT retention score for patients was 19%, and this differed depending on the suspected BAM type, with suspected type 1 having the lowest mean retention of 9%. Similarly, 79% of patients with suspected BAM type 1 had SeHCAT retention of <15%, compared with 42% and 45% for patients with types 2 and 3, respectively. This is consistent with expectations, as lower retention scores should certainly be seen in patients who have terminal ileal disease or resection, as per previous studies.1 ,17 The fact that 21% of type 1 patients have SeHCAT scores of over 15% suggests that empirical trials of therapy in this group, bypassing the SeHCAT test altogether, would be a suboptimal approach. For the other BAM types (2 and 3), where the majority of the SeHCAT results are over 15%, the test has potential utility in targeting treatment or further investigation.
Aspects of the SeHCAT scans themselves were captured at an individual patient level. A consistent finding was that almost all patients underwent their second SeHCAT scan 7 days after the first. Prior to the SeHCAT scans, 16% of patients (n=117/732) reported taking medication that might have influenced the SeHCAT test. A further study would need to address this potentially confounding factor. Current guidelines suggest that in patients over 45 years of age, colonoscopies are undertaken before undergoing a SeHCAT test.2 ,3 However, this survey found that among 45+ year olds, 29% (n=101/351) reported no colonoscopy (since symptoms began) prior to SeHCAT, suggesting that the guidelines are not closely followed in the UK gastroenterology community, at least in centres with access to SeHCAT.
Overall, BAS was reported as being prescribed to just over a third of patients, with the majority (70%) initially prescribed colestyramine, reflecting the findings of a similar study where colestryamine represented the most commonly prescribed BAS treatment.18 Although colesevelam is not licensed for use in the UK for BAM treatment, 28% of patients prescribed BAS were specifically prescribed colesevelam. Notably, BAS was not prescribed for 27% of patients with a centre-defined ‘abnormal’ result, nor to 24% of patients with a SeHCAT score of <15%, highlighting an apparent inconsistency in how the SeHCAT information is used within patient care pathways across these NHS centres. It is not clear how the SeHCAT retention score influences the decision to prescribe BAS, or if this is determined by other clinical factors or centre-specific guidelines.
A fundamental aim of the survey was to capture follow-up information on patients who were either prescribed BAS or not, regardless of the result of the SeHCAT test. In total, 340 patients had follow-up information entered into the database during the survey period. Among 140 patients prescribed BAS, a majority reported reduced clinical symptoms of diarrhoea severity, pain, urgency or bloating. The majority of the 200 patients who were not prescribed BAS reported no change post-SeHCAT in clinical symptoms. A limitation of the study is the high level of missing symptomatology data among the followed-up patients. The numbers are too small to fully interpret the relationship between symptom improvement and SeHCAT retention or suspected BAM type. Furthermore, the length of time for which BAS prescriptions were continued could not be ascertained.
One of the findings of this survey is the high level of heterogeneity, both in centre practices and among the patient population. Centres reported differing procedures for carrying out SeHCAT scans and adopted different SeHCAT retention cut-offs for determining an abnormal result. The prescription of BAS seemed highly variable and not simply linked to either the SeHCAT retention value or the centre-defined result. There was also considerable variation in the use of a range of other treatments post-SeHCAT, regardless of whether a patient received a BAS prescription or not. The patient population is heterogeneous by the nature of the three different BAM types, particularly the range of secondary conditions included within BAM type 3, and in their presenting symptoms. Hence while the survey is large and contains rich data, the ability to make meaningful comparisons between patient sub-groups is restricted by the large number of confounding factors inherent in such heterogeneity. This would support the case for a future prospective, placebo-controlled trial of BAS, with clear inclusion criteria and standardised protocols.
Another key finding was that many patients undergo SeHCAT without prior colonoscopy, indicating that the current BSG guidelines for investigating chronic diarrhoea3 are not adhered to, at least in centres with access to SeHCAT. The guidelines, which would always place colonoscopy before SeHCAT, may need reconsideration as to the positioning of SeHCAT in the pathway, but better primary evidence is required to underpin this.
In summary, the survey has identified wide variations in clinical practice in the interpretation of SeHCAT results, and in management and follow-up, and limited adherence to BSG guidelines. Coupled to variable access to SeHCAT testing across the UK, these findings already have significant implications for the consistency and equity with which patients with chronic unexplained diarrhoea are assessed and managed in the UK NHS.
Conclusions
In this study, the current provision of SeHCAT to a referred patient population with suspected BAM has been characterised across 38 UK centres. The study has provided valuable information on the distribution of SeHCAT test results, on BAS prescription rates, and on symptom improvement following treatment. The study has confirmed that a range of different criteria are used by centres when defining an ‘abnormal’ SeHCAT result. BAS prescription was not simply related to the SeHCAT result, nor to the centre-defined result, but appears to be influenced by other factors. The majority of patients receiving BAS treatment showed an improvement in symptoms.
The results of this survey have provided key information to help optimise the design of a future diagnostic accuracy study,13 to clarify the optimal classification of SeHCAT retention scores, and to enable the specific research questions set out in the NICE DG7 guidance to be addressed. Further research is also warranted to investigate the efficacy of BAS according to BAM type, SeHCAT retention and other clinical characteristics.
Acknowledgments
The authors thank the members of the KiTEC SeHCAT Studies Clinical Advisory Board for their clinical advice (see appendix). The authors thank Dr Gill Vivian and Professor Roy Sherwood from King's College Hospital NHS Foundation Trust for their advice on the design and implementation of the survey. The research was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy's and St Thomas' NHS Foundation Trust and King's College London. The views expressed are those of the authors and not necessarily those of NICE, the NHS, the NIHR or the Department of Health. The authors thank all participating centres for their contribution to the survey. The UK NHS participating centres are as follows (centres marked with an asterisk piloted the survey): Ashford & St. Peter's Hospitals NHSFT; Brighton & Sussex University Hospitals Trust; Cambridge University Hospitals NHSFT*; Chelsea & Westminster Hospital; County Durham & Darlington NHSFT; Imperial College Healthcare, London, NHSFT; Kent and Canterbury Hospital; King's College Hospital, London, NHSFT*; Lewisham & Greenwich NHSFT; Mid Staffordshire NHSFT; New Cross Hospitals, Wolverhampton, NHSFT*; Norfolk & Norwich University Hospital, NHSFT; North Bristol NHSFT; North Cumbria University Hospitals NHSFT; North Tees & Hartlepool NHSFT; North West London NHSFT; Nottingham University Hospitals NHSFT*; Oxford University Hospitals, NHSFT; Parkside Hospital, London; Poole Hospital NHSFT and The Royal Bournemouth and Christchurch NHSFT; Portsmouth Hospitals NHSFT; Queen Elizabeth Hospital, Birmingham; Queen Elizabeth Hospital, Gateshead; Rotherham NHSFT; Royal Bolton NHSFT; Royal Cornwall Hospital; Royal Derby Hospital; Royal Liverpool & Broadgreen University Hospitals Trust; Royal United Hospital NHSFT; Royal Victoria Hospital, Belfast; Salford Royal NHSFT*; Sandwell & West Birmingham NHSFT; Sheffield Teaching Hospitals NHSFT; St George's Hospital, Tooting, London; United Bristol Hospitals NHSFT; University Hospital Coventry and Warwickshire NHSFT; University Hospital North Staffordshire; Western Sussex Hospitals NHSFT.
References
Footnotes
JMcL and FR are joint last authors.
Contributors The study concept and design of study was undertaken by JAS, JP, BC, VM, CL, SK, RL, JMcL and FR. Analysis and interpretation of data were undertaken by JAS, JP, BC, MO, JMcL and FR. Drafting of the manuscript was completed by JAS, JP, CL, SK, RL, JMcL and FR. All authors contributed to the preparation of this manuscript. CL and SK are guarantors for the overall content.
Funding King's Technology Evaluation Centre (KiTEC) is funded by the National Institute for Health and Care Excellence (NICE) to act as an External Assessment Centre for the Medical Technologies Evaluation Programme.
Competing interests Several of the authors (JAS, JP, BC, VM, MO, CL, SK and FR) were employed/funded by King's Technology Evaluation Centre (KiTEC). As per above funding description, KiTEC was funded by NICE. NICE reviewed this manuscript but played no part it its composition. Three of the authors (CL, SK and RL) are NHS employees. JM was Chair of the British Society of Gastroenterology research committee at the time of the study.
Ethics approval Guidance from the UK National Research Ethics Service (NRES) indicated that structured data collection for the SeHCAT survey fulfilled the criteria for service evaluation and did not require UK NHS Research Ethics Committee (REC) review.33 Furthermore, the ‘Department of Health governance arrangements for research ethics committees: a harmonized edition 2011’34 indicates characteristics of studies where an NHS REC review is required (section 2.3.12) and these did not apply to this survey. The same document states “RECs are not expected to consider applications in respect of activities that are not research such as clinical audit, service evaluation and public health surveillance” (section 2.3.12).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement KiTEC will retain the data set and perform all analyses. Data will not be shared with other parties for further research in keeping with the remit of the service evaluation.