Article Text

Abstract
Background An estimated 170 million people worldwide are infected with hepatitis C virus (HCV). HCV genotype 4 (HCV-4)—the most prevalent hepatitis C strain in the Middle East and Africa—is difficult to treat, with an estimated sustained virological response (SVR) of 53% when using pegylated interferon and ribavirin (P/R) in treatment-naïve patients with HCV-4 infection. In regions where access to direct-acting antivirals is limited, re-treatment of patients who failed therapy with another course of P/R may be an option if the success rate is acceptable.
Objectives We aimed to determine the SVR from retreatment with P/R in treatment-experienced patients with HCV-4 infection.
Methods We performed a meta-analysis using MEDLINE and EMBASE searches, and by reviewing article bibliographies and abstracts from recent Liver Society Meetings. Original studies featuring at least 10 adult, treatment-experienced patients with HCV-4 infection failing prior interferon-based therapy and receiving subsequent re-treatment with P/R were included.
Results 3 studies were included. Overall pooled SVR was 32.7%, or 41/126 patients. No significant heterogeneity existed among the studies. One study reported higher SVR of 50% in previous relapsers, compared with 23% in previous non-responders.
Conclusions As expected, treatment-experienced patients achieved lower rate of SVR compared with previously reported SVR for treatment-naïve patients with HCV-4 infection. The abysmal rate of success from re-treatment with P/R supports the use of direct-acting antivirals whenever re-treatment is considered, even in resource-limited regions.
- HEPATITIS C
- GENOTYPE
- INTERFERON
- META-ANALYSIS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Hepatitis C virus (HCV) genotype 4 (HCV-4) infection is highly prevalent in Africa and the Middle East, accounting for over 80% of patients with chronic HCV infection in many areas of this region.1 Globally, HCV-4 is responsible for 20% of the estimated 130–150 million patients with HCV infection.2 Treatment success using pegylated interferon and ribavirin (P/R), defined by achieving sustained virological response (SVR), is estimated at 53% for treatment-naïve patients with HCV-4 infection.3 This means that approximately half of the patients who undergo such regimen experience failure due to null-response or relapse. While newer direct-acting antiviral (DAA) medications have demonstrated remarkable efficacy in patients with HCV-1 infection who had experienced prior failure with P/R,4 their cost and accessibility pose barriers to rapid worldwide adoption.5 Therefore, in areas where newer therapies are limited, another course of P/R may be the only option at the present.
To this effect, we conducted a meta-analysis and review of available literature to determine the SVR after re-treatment with P/R in treatment-experienced patients with HCV-4 infection. All published primary papers and abstracts regardless of study design were considered, and those fulfilling predetermined eligibility criteria were included. To the best of our knowledge, no such effort on this topic has been undertaken before. This meta-analysis adds to existing literature by providing a comprehensive evaluation of re-treatment efficacy using P/R in patients who have chronic HCV-4 infection and experienced prior failures with interferon (IFN)-based therapy.
Methods
We adhered to the PRISMA guidelines in the design, implementation, analysis and reporting of this meta-analysis.6 A review protocol was established during the design stage by the consensus of all authors involved, and was followed during the identification of eligible studies and data extraction (see online supplementary data).
supplementary data
Data identification
We conducted a comprehensive search in the literature databases MEDLINE and EMBASE, last accessed 18 January 2014, using the search term: (‘genotype 4’). We excluded articles that were not in English; no other search restrictions were imposed. We also completed a manual search of abstracts from annual scientific meetings by the American Association for the Study of Liver Diseases (AASLD), the European Association for the Study of the Liver (EASL), the Digestive Diseases Weeks (DDW), and the Asian Pacific Association for the Study of Liver (APASL) between the years 2012 and 2013 using the terms: (‘experienced’, ‘re’, ‘prior’, ‘before’, ‘previously’, and ‘failed’). We manually reviewed the bibliographies of published studies for additional studies eligible for inclusion. Two authors (BZ and BEY) independently conducted all searches. Search sources and search terms were predetermined by the agreement of all authors prior to execution. Only published data extracted from eligible studies were included in this meta-analysis.
Study eligibility
Studies were considered for inclusion in our analysis if they were – original studies (i) featuring at least 10 adult (ii) treatment-experienced patients (iii) with chronic HCV-4 infection (iv) who have failed prior interferon-based therapy (either due to non-response or relapse) (v) and were subsequently retreated with another course of P/R combination therapy (vi). Studies were excluded if they included children or adolescents (i) or otherwise failed to satisfy the inclusion criteria (ii). Two authors (BZ and BEY) independently reviewed the titles and abstracts of relevant studies for eligibility. Duplicate publications were identified independently by cross-referencing the first and the last authors, collaboration groups, and the number of participants featured in each study. Any discrepancy was reviewed by a third review author (NHN) and resolved by consensus. Unless specifically stated by the included studies’ authors, patients were assumed to not be co-infected with hepatitis B virus (HBV)/HIV, or have any other liver-related diseases.
Data extraction and statistical analysis
We designed a data extraction form to record both the total number of patients and those who achieved SVR. We also recorded each study's design (prospective vs retrospective), study type (randomised controlled trial vs observational), intention-to-treat (ITT) analysis (yes or no), and country of origin. Baseline patient characteristics, treatment protocol, and treatment responses of each study were recorded, including age, sex, prior relapser versus non-responder, treatment duration, rapid virological response (RVR), early virological response (EVR), and SVR. The extraction form initially contained a number of possible prognosticators of treatment success, as discussed by Yee et al,3 but were removed after their omission from most articles we reviewed in-depth. Data extractions were performed by two authors (BZ and BEY).
Statistical analysis
Our prespecified primary outcome is the probability of successfully re-treating chronic HCV-4 infection with a second course of P/R for the patients who had experienced failure with prior IFN-based therapy. Secondary outcomes included estimates of achieving SVR in prior relapsers versus non-responders, and the probability of achieving SVR in patients who achieve RVR or EVR. We obtained pooled event rates with corresponding 95% CIs using random-effects model (DerSimonian and Laird method), and inverse variance method.7 Study heterogeneity was determined with χ2-based Cochrane Q-statistic (p value set at ≤0.05) and I2 set at ≥50%, in accordance to the standard of quality for reporting meta-analysis from the Cochrane handbook.7 To assess for bias introduced by varying study characteristics in the primary analysis, we attempted univariate and multivariate random-effects meta-regression to identify heterogeneity in primary outcome. All statistical tests were two-sided. All analyses were performed using Comprehensive Meta-Analysis, V.2 (Biostat, Englewood, New Jersey, USA), and STATA 11 (StataCorp, College Station, Texas, USA).8–11
Results
Literature search results
Our literature search identified 1798 studies (729 from MEDLINE and 1069 from EMBASE), and 14 648 abstracts from major liver society meetings (4327 from AASLD, 4204 from DDW, 3260 from APASL and 2857 from EASL) held between 2012 and 2013. One hundred and forty-eight studies (see online supplementary data) were selected for closer evaluation of eligibility and extractable data. Of these studies, 145 were excluded—121 for naïve or unknown prior treatment status, 15 for redundancy, 4 for non-extractable data, 3 for number of total patients less than 10, and 2 for including children and adolescents. After exclusion of aforementioned studies, two full-length articles and one abstract were included in the meta-analysis12–14 (figure 1).
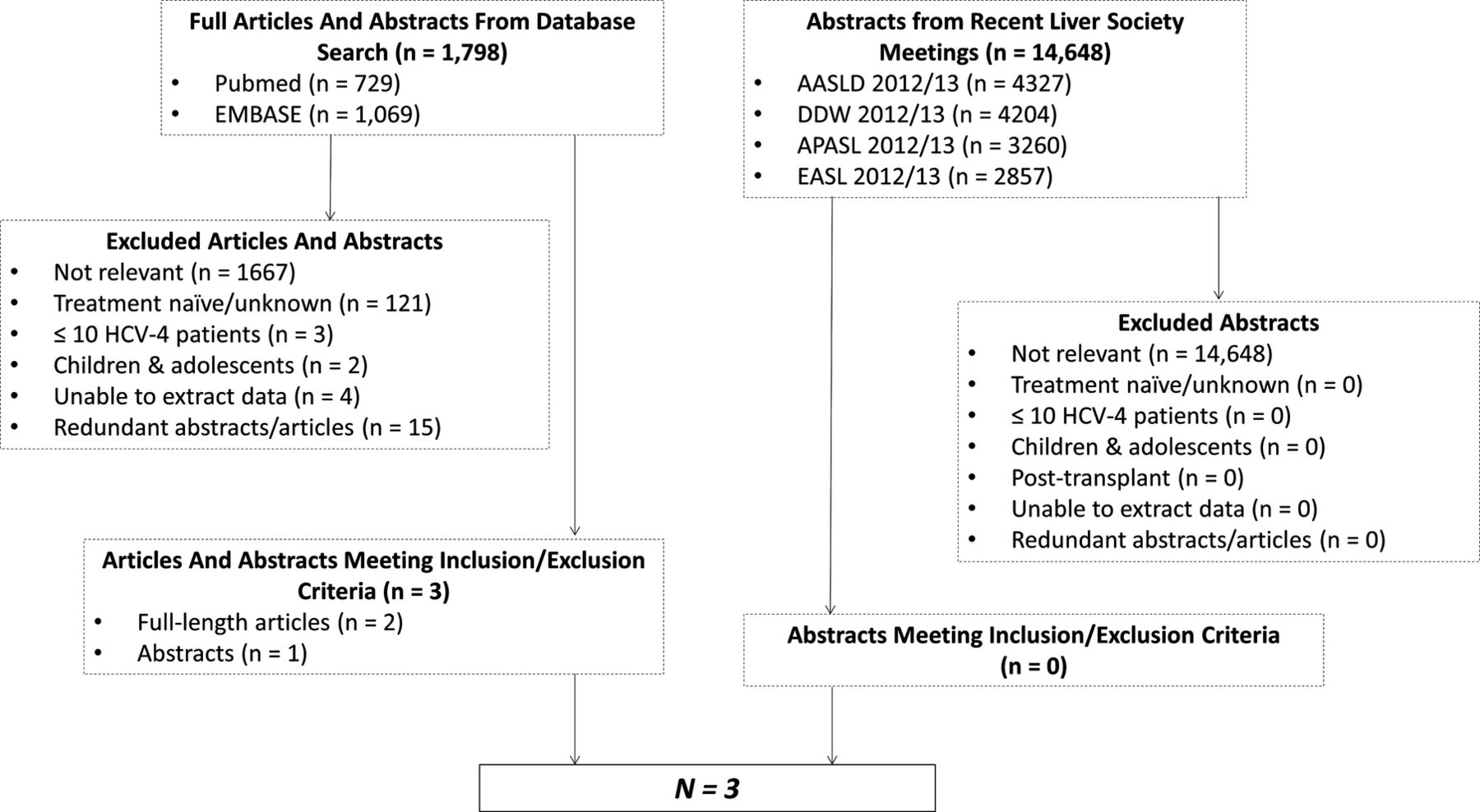
Flow chart of studies from initial search, and those meeting or failing to meet inclusion criteria for meta-analysis (AASLD, American Association for the Study of Liver Diseases; APASL, Asian Pacific Association for the Study of Liver; DDW, Digestive Diseases Weeks; EASL, European Association for the Study of the Liver; HCV-4, hepatitis C virus genotype 4).
Study characteristics
Three studies with a total of 126 individuals were included in our pooled analysis (figure 1). Two studies originated from Saudi Arabia12 ,13 and another from Portugal.14 All three studies were retrospective in design. One study13 provided analysis based on ITT, with 37 of 56 (66%) patients actually completing treatment. Of the other two studies, 51 of 59 patients (86.4%) completed treatment in one,12 while the other14 did not disclose the rate of treatment completion. One study14 reported that all re-treated patients had previously failed regimens of standard IFN with or without ribavirin (RBV). Only one study12 provided baseline characteristics for treatment-experienced patients, including age (52.2±10.7; mean±SD), gender (male=36/59, or 61%), HBV/HIV co-infection (10/59, or 16.9%), and previous organ transplant (7/59, or 11.9%). Intended length of treatment was a minimum of 48 weeks in all three studies.
Sustained viral response
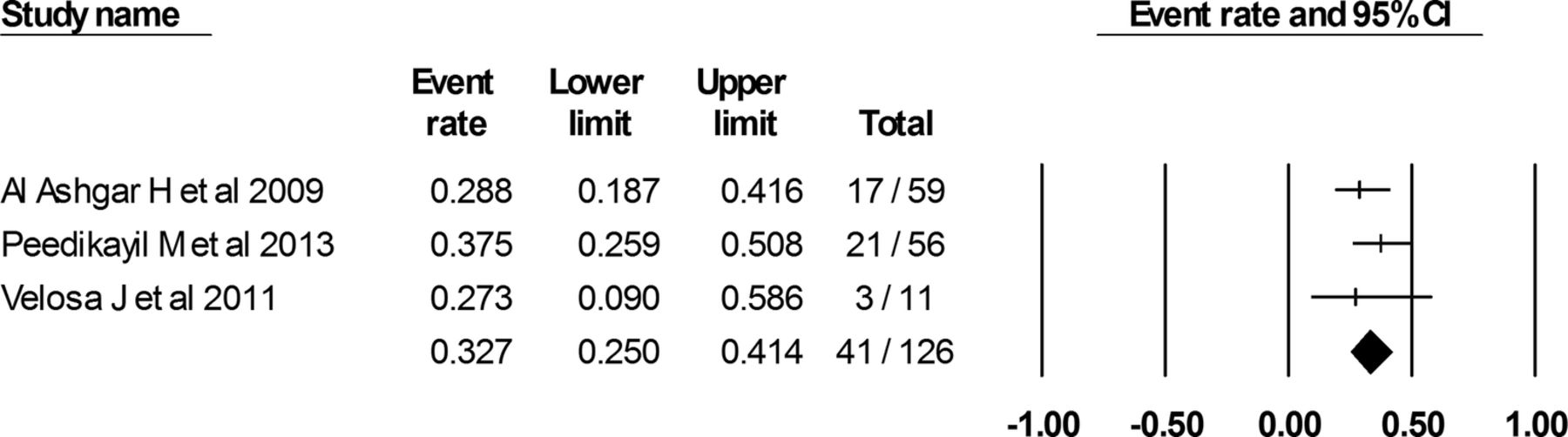
On basis of the three studies and a total of 126 patients with HCV-4 infection who received re-treatment with P/R, 41 achieved SVR, amounting to a pooled treatment success rate of 32.7% (CI 25.0% to 41.4%) (figure 2). Heterogeneity was not detected among these studies (Q-value=1.13, p=0.57, I2=0.00).

{kind=link}
{kind=link}
Pooled rate of sustained virological response.
One study13 noted that SVR was higher in patients who experienced previous treatment failure due to relapse (50%) versus the non-responders (23.1%).
Discussion
As expected, the rate of achieving SVR with another course of P/R in treatment-experienced patients with HCV-4 infection who had failed prior IFN-based therapy was greatly diminished compared with treatment-naïve individuals,3 despite being slightly better than that previously reported for mixed genotypes.15 ,16 Prior relapsers were significantly more likely to achieve SVR, consistent with published findings, and this is even demonstrated in the re-treatment of patients with newer DAA therapeutics.4 ,15 Such high probability of re-treatment failure with P/R in patients with HCV-4 infection supports the use of DAA for re-treatment even in resource-limited areas, and especially for individuals who were non-responders to the initial course of IFN-based therapy. Our finding supports current practice guidelines issued by the EASL and the AASLD, which recommend the incorporation of DAA in the re-treatment of patients with HCV-4 infection who have failed the previous P/R therapy.17 ,18
This study has several strengths. We performed an extensive literature search using two study databases, abstracts from four major liver conferences spanning 2 years, and reviewed articles’ bibliographies. No such comprehensive review on this topic has been published before. Despite the small number of studies included in analysis, the outcome lends evidence to the current EASL and AASLD recommendations even in resource-limited countries and regions.
A number of weaknesses also merit careful consideration, mostly stemming from paucity of available data. Despite our thorough review of literature, only three studies were identified and incorporated into the analysis. Only one of these studies reported baseline characteristics for the targeted patient population, preventing in-depth analysis of possible prognostic factors for SVR.12 The pooled estimate for the rate of re-treatment success with P/R between prior relapsers versus non-responders, which may vary significantly,13 could not be determined due to lack of primary data. Study patients were also heterogeneous with regard to types of IFN or use of RBV during prior therapies; nevertheless, pooled SVR was low even with inclusion of patients who may have had only standard IFN and without RBV. As with any comprehensive review, differences in the quality of studies and reporting exist, and patient populations differ across the included studies. Newer publications since the implementation of this meta-analysis are not considered.
In conclusion, the result of our meta-analysis identified a low probability of success with repeated P/R combination therapy in patients with HCV-4 infection with prior IFN-based therapy failure, supporting the use of DAAs when re-treatment is considered even in resource-limited regions.
References
Footnotes
Contributors BZ contributed in the study design, data collection, data analysis and interpretation, and in the drafting of the manuscript. NHN contributed in the study design, data analysis and interpretation, and in the drafting of the manuscript. BEY contributed in the study design, data collection and interpretation, and in the drafting of the manuscript. BY participated in the data collection. MHN contributed in the study concept and design, data analysis and interpretation, and in the critical revision of the manuscript. All the authors have critically reviewed the manuscript and approved its final version.
Funding This study was funded in part by the NIH National Center for Research Resources, TL1 training grants, 1TL1RR03197, to NHN and BZ.
Competing interests MHN has served as an advisory board member and has received research support from Gilead Sciences, Janssen Pharmaceuticals, and Roche Laboratories.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.