Article Text

Abstract
Objective The transjugular intrahepatic portosystemic shunt (TIPS) procedure is an important intervention for management of complications of portal hypertension. The objective of this study was to identify predictors of mortality from the TIPS procedure with a focus on race and ethnicity.
Design TIPS procedures from 2012 to 2014 in the National Inpatient Sample were identified. Weighting was applied to generate nationally representative results. In-hospital mortality was the primary outcome of interest. χ2 and Student’s t-tests were performed for categorical and continuous variables, respectively. Predictors of mortality following TIPS were assessed by survey-weighted logistic regression.
Results 17 175 (95% CI 16 254 to 18 096) TIPS cases were identified. Approximately 71% were non-Hispanic (NH) white, 6% were NH black, 16% were Hispanic and 7% were other. NH black patients undergoing TIPS had an in-hospital mortality rate of 20.1%, nearly double the in-hospital mortality of any other racial or ethnic group. NH black patients also had significantly longer median postprocedure and total lengths of stay (p=0.03 and p<0.001, respectively). The interaction of race by clinical indication was a significant predictor of in-hospital mortality (p<0.001). NH black patients had increased mortality compared with other racial/ethnic groups when presenting with bleeding oesophageal varices (OR 3.85, 95% CI 2.14 to 6.95).
Conclusion This cohort study presents important findings in end-stage liver disease care, with clear racial disparities in in-hospital outcomes following the TIPS procedure. Specifically, black patients had significantly higher in-hospital mortality and longer lengths of stay. Further research is needed to understand how we can better care for black patients with liver disease.
- portal hypertension
- chronic liver disease
- cirrhosis
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. Data for the years 2012–2014 were obtained from the National Inpatient Sample, a database constructed by the Agency for Healthcare Research and Quality (AHRQ) Healthcare Cost and Utilization Project (HCUP). This database is publicly available for purchase on the HCUP website.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
Recent studies have reported black race is an independent predictor of mortality following the transjugular intrahepatic portosystemic shunt (TIPS) procedure. Race was not the focus of these studies.
What are the new findings?
Among the 17 175 TIPS procedures identified, significant racial variation in in-hospital mortality existed, such that black patients had a 20% mortality rate, about twice the rate of all other racial groups.
How might it impact on clinical practice in the foreseeable future?
This study presents racial disparities in outcomes following TIPS. It contributes to a growing body of literature suggesting racial disparities in access to care and outcomes exist for patients with end-stage liver disease.
Introduction
Transjugular intrahepatic portosystemic shunt (TIPS) insertion plays an important role in the management of chronic liver disease and, specifically, complications of portal hypertension. The procedure achieves portal decompression through creation of a conduit between the hepatic and portal veins. Common indications for TIPS include bleeding oesophageal varices (EVB) and ascites refractory to conservative management.1–8 TIPS carries risk of significant morbidity including hepatic encephalopathy and early liver failure with resulting risk of mortality.9 10 Clinician judgement is therefore required to identify patients who can benefit from TIPS placement.
Recent studies have reported black race is an independent predictor of mortality following the TIPS procedure.11 12 Race was not the focus of these studies. Healthcare disparities have previously been reported in liver transplantation access, hepatocellular carcinoma management and management of gastrointestinal haemorrhage.13–16 The purpose of this study was to identify predictors of mortality from the TIPS procedure with a focus on race and ethnicity.
Materials and methods
This study was declared exempt by the Duke Health Institutional Review Board.
Data sources
Data for the years 2012–2014 were obtained from the National Inpatient Sample (NIS), a database constructed by the Agency for Healthcare Research and Quality Healthcare Cost and Utilization Project (HCUP).17 This database represents the largest public, all-payer, inpatient sample in the USA. With around 7 million hospitalisations per year, the NIS is a 20% stratified sample of discharges from US community hospitals, representing more than 97% of the US population.17
Study cohort
The cohort was limited to adult (age ≥18) TIPS procedure cases in the USA between 2012 and 2014. TIPS procedure cases were identified by International Classification of Diseases, Ninth Revision procedure code 39.1. Procedures with missing race/ethnicity information were removed from analysis (5.2%). There was no imputation for missing values.
Baseline characteristics and outcomes
Statistical analyses were performed using SAS V.9.4 (SAS Institute). Descriptive statistics for patient characteristics, hospital characteristics and for outcomes were calculated by race/ethnic group. All descriptive statistics were weighted using weights provided by HCUP and were reported with 95% CIs. Global tests of significance were performed comparing baseline characteristics, in-hospital mortality, total and postprocedure length of stay (LOS), and discharge location across racial/ethnic groups. Pairwise testing was not performed. In-hospital mortality was the primary outcome of interest. Secondary outcomes were total and postprocedure LOS and discharge location. Clinical indication for each procedure was determined by a hierarchy of clinical severity adapted from Trivedi et al.12 For any procedure with multiple diagnoses listed, the recorded clinical indication was the higher severity diagnostic code. The adapted clinical severity hierarchy was as follows: EVB, gastrointestinal bleeding (GIB), Budd-Chiari syndrome (BCS), hepatic hydrothorax, ascites, portal vein thrombosis (PVT), portal hypertension (PoHTN) and other.12
Modelling predictors of mortality
To account for possible interactions between predictors of mortality and race we modelled the data using a survey-weighted logistic regression model. The outcome of interest was mortality, defined as in-hospital death. The full model included the following covariates: age, gender, race-ethnicity (non-Hispanic (NH) white, NH black, Hispanic, other), clinical indication (EVB, GIB, BCS, hepatic hydrothorax, ascites, PVT, PoHTN, other), hospital bed size (small/medium, large), payer (Medicare, Medicaid, private, other), admission type (elective, non-elective), postprocedure LOS and Elixhauser Comorbidity Score18; as well as the following interaction terms: age*race, gender*race, indication*race, hospital bed size*race, payer*race, admission type*race, postprocedure LOS*race and Elixhauser Comorbidity Score*race. Race/ethnicity was our covariate of interest (NH white, NH black, Hispanic, other). Postprocedure LOS was log-transformed using the natural logarithm in all analyses. Additionally, we included race/ethnicity interactions with each of the previously listed control variables. We first fit the full model (all main effects and all interactions terms) and used backwards selection at α=0.05 to remove each non-significant interaction term until we reached the final model. Main effects were not considered for the selection process.
Results
Population characteristics
There were 17 175 (95% CI 16 254 to 18 096) TIPS procedures from 2012 to 2014 after applying weighting. Approximately 71% were NH white, 6% NH black, 16% Hispanic and 7% other racial/ethnic groups. Population characteristics by race/ethnicity are presented in table 1. There were significant differences in gender distribution across racial/ethnic groups (p value =0.001), with the highest percentage of females (41%) in the other race group and the lowest percentage of females (29%) among Hispanics. There was a significant difference in average age among races/ethnicities (p value <0.01) ranging from an average age of 55 years among Hispanic patients to 57 years among NH Whites. NH whites had a higher percentage of elective procedures, while NH black and Hispanic patients had the lowest percentage of elective procedures (p value =0.009). Medicare was the most common payer among NH whites and Hispanics, while Medicaid was most common for NH black patients. Private insurance was the most common payer for the other race/ethnicities group (p value <0.001). Although there was variation in hospital size by race (p value <0.001), the majority of cases for all races and ethnicities occurred in large hospitals. The median LOS from admission until procedure ranged from 0.8 days for whites to between 1.3 and 1.4 days for all other races/ethnicities (p value <0.001).
Baseline population characteristics by race/ethnicity
Outcomes
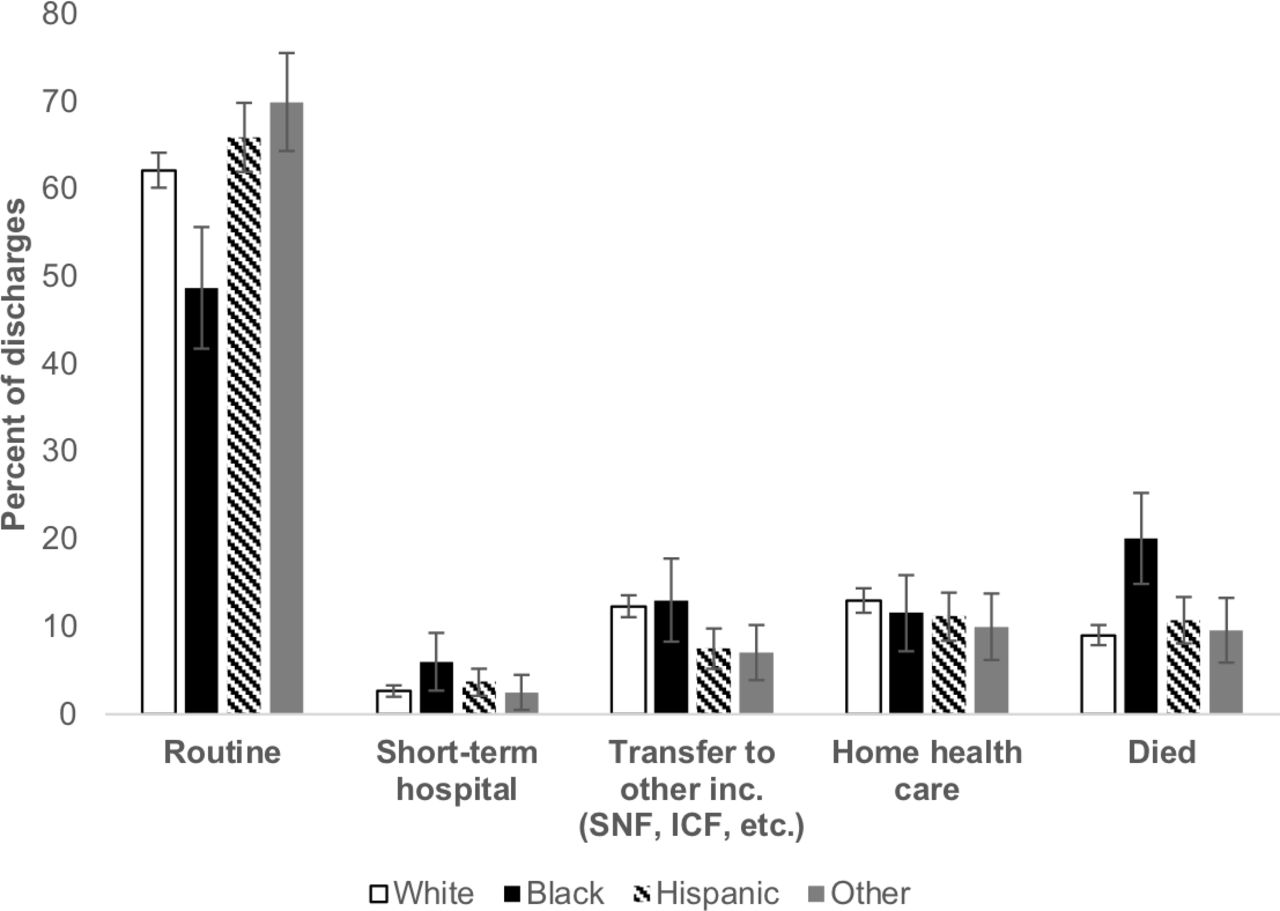
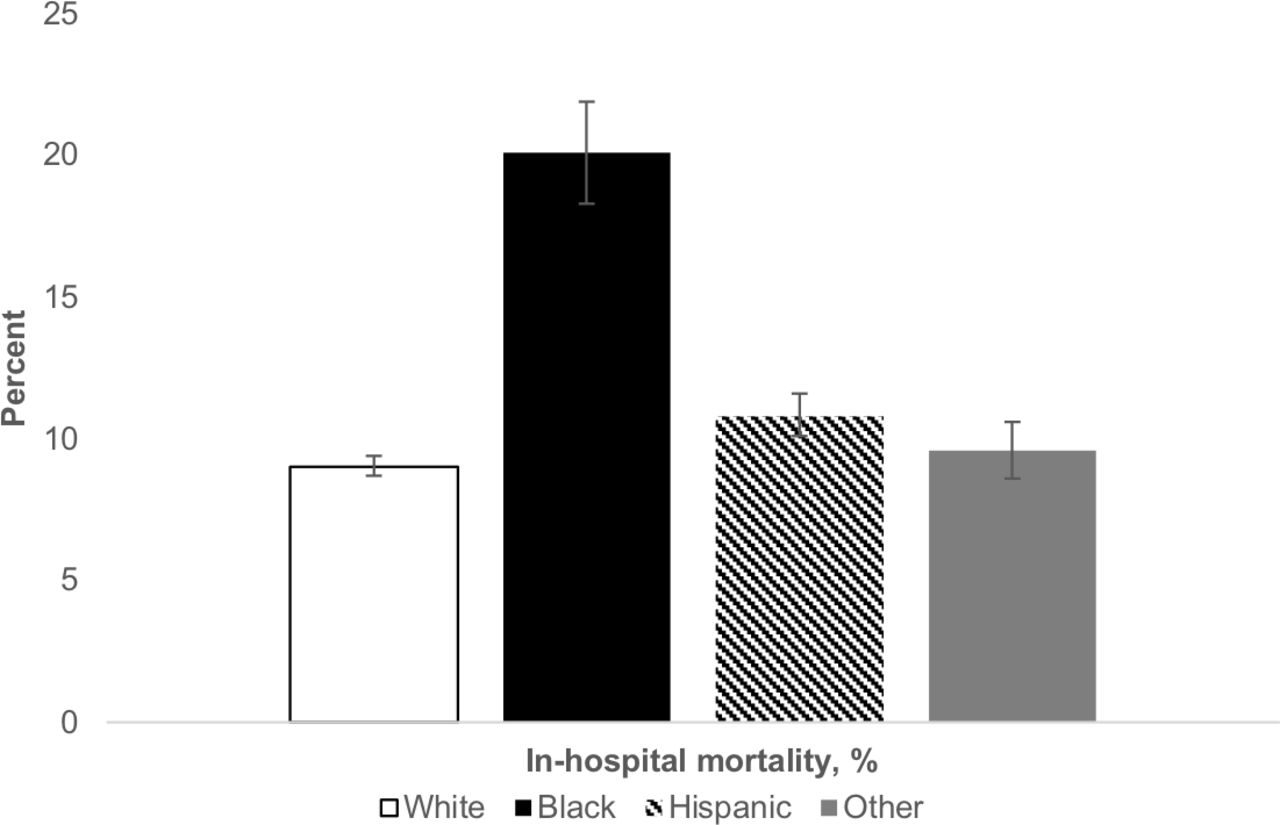
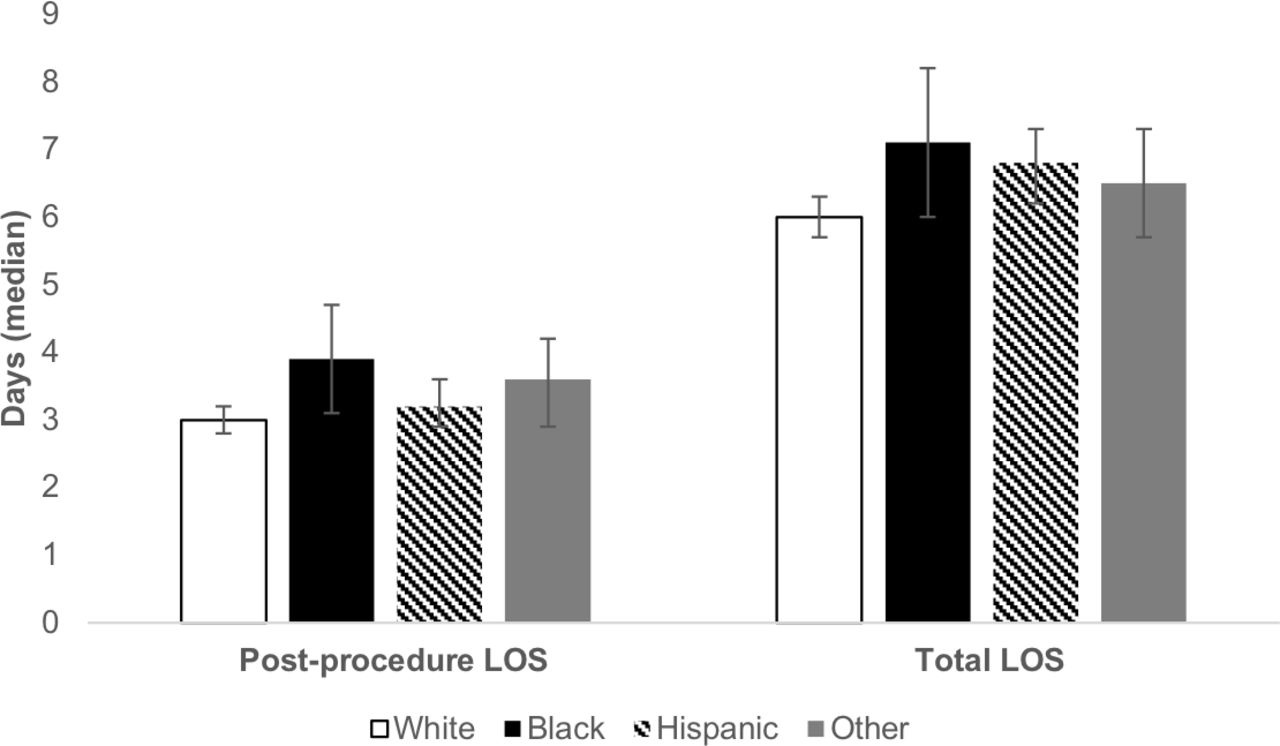
There was a significant difference in in-hospital mortality, such that NH black patients had a 20% mortality rate, about twice the rate of all other racial/ethnic groups which ranged from 9% to 10.8% (p value <0.001; figure 1). Among the secondary outcomes, there were significant differences in total and postprocedure LOS (p value <0.001 and p value =0.03, respectively; figure 2). NH black patients had the longest total and postprocedure median LOS. NH black patients were also nearly two times as likely to be discharged to a short-term hospital compared with all other racial groups (6% compared with 2.5%–3.7%; figure 3). About 50% of NH black patient discharges were considered routine compared with 60%–70% for all other racial groups. Due to low counts for discharged alive with destination unknown and discharged against medical advice, these categories were omitted per HCUP standards of reporting.
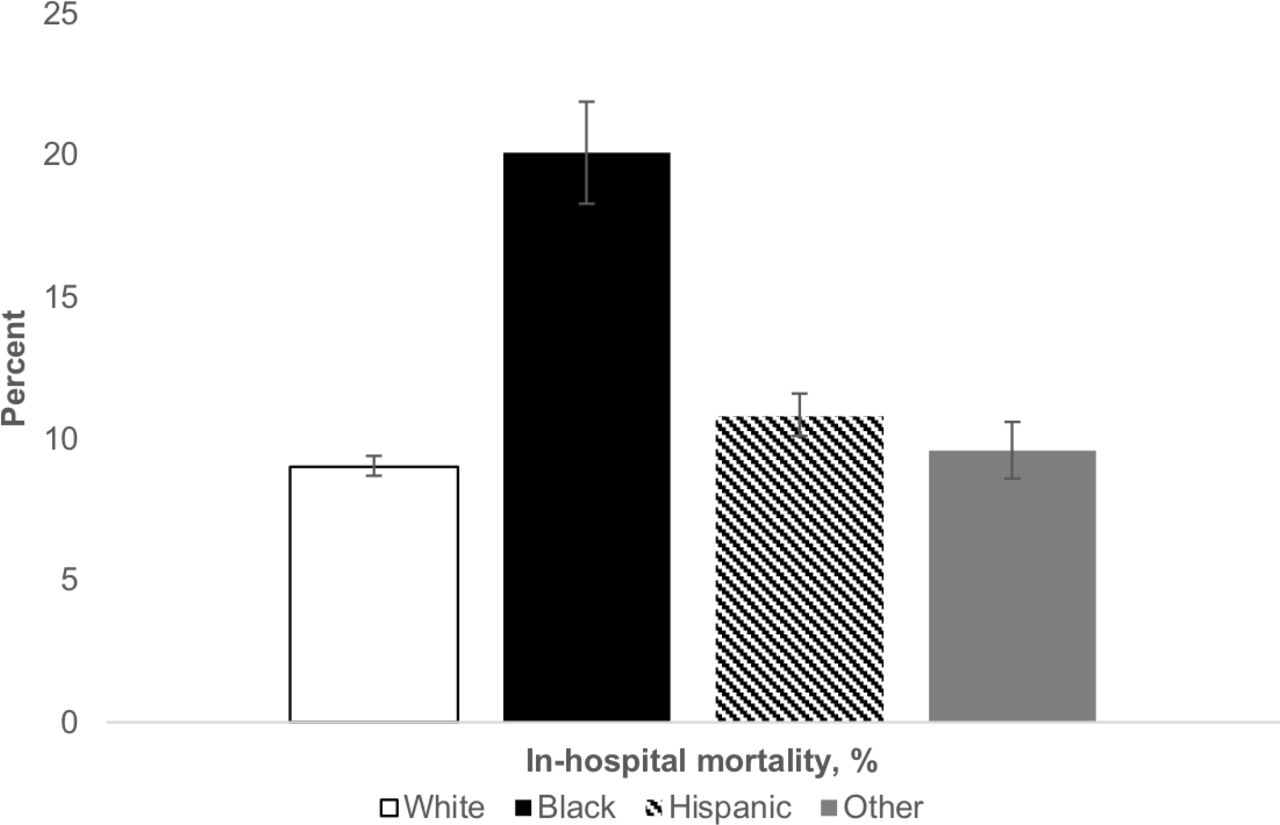
In-hospital mortality by race/ethnicity. Significant variation in in-hospital mortality between groups was observed (p<0.001).
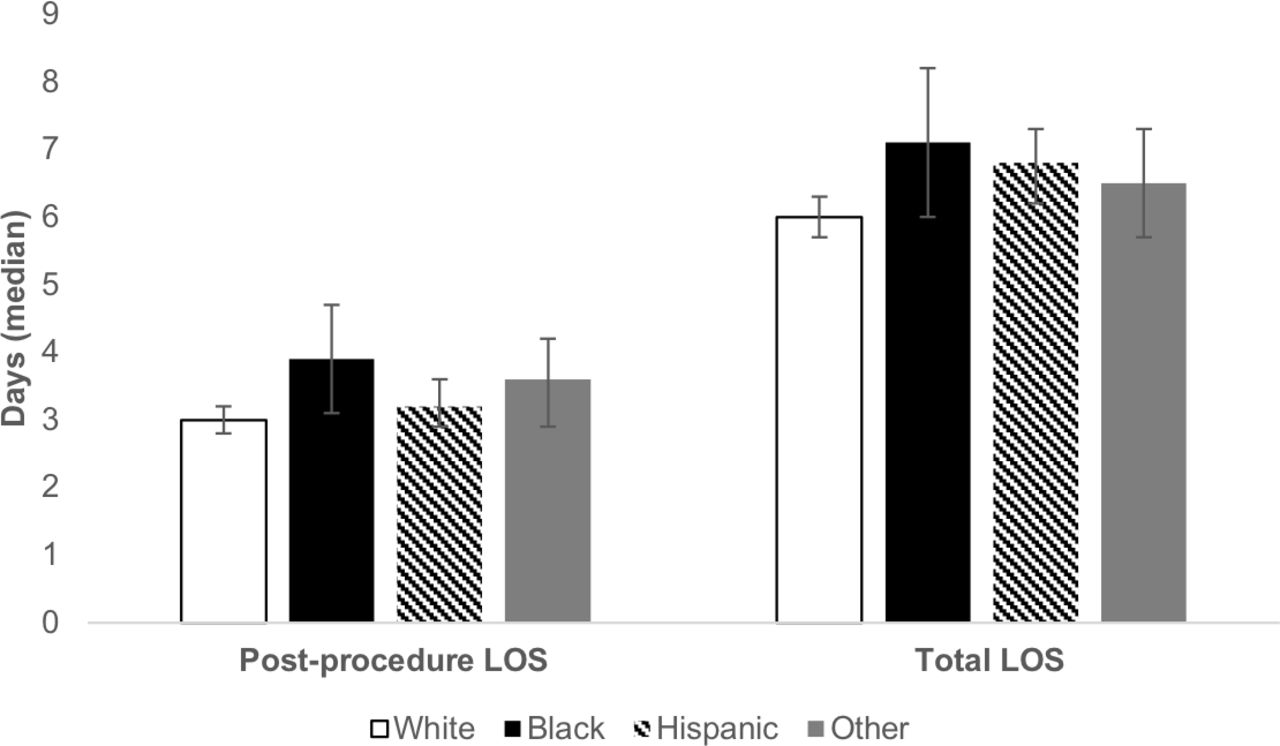
Postprocedure and total LOS by race/ethnicity. Significant variation between groups was present in both postprocedure and total LOS (p=0.03 and p<0.001, respectively). LOS, length of stay.
{kind=link}
{kind=link}
{kind=link}
Per cent of each race/ethnic group falling into the labelled discharge categories. A significant difference in the distribution of disposition at discharge was observed across these racial/ethnic groups (p<0.001). ICF, intermediate care facility; SNF, skilled nursing facility.
Predictors of mortality
After backwards selection, the final model included all of the main effect variables (age, gender, clinical indication, hospital bed size, payer, admission type, natural logarithm of days postprocedure, Elixhauser Score and race/ethnicity), which were not considered for selection, and a single interaction term, race by clinical indication. No other interaction terms from the full model remained in the final model. Indication for the procedure, admission type, Elixhauser Score, race/ethnicity and the interaction between race and indication were all significant predictors for the probability of mortality. The results of the model are displayed in table 2. Non-elective admission and increased comorbidity score both increased the odds of mortality. With regards to the interaction term race by clinical indication, NH black patients had significantly increased mortality compared with all other racial/ethnic groups when presenting with EVB or PVT. No other interaction variables were significant. Per standards of reporting, ORs for selected results are withheld from table 2 due to low counts.
OR estimates from survey-weighted logistic regression model
Discussion
In this nationally representative cohort study, we found in-hospital TIPS outcomes were far worse for NH black patients. NH blacks undergoing TIPS had significantly higher in-hospital mortality, longer LOS and lower rates of routine discharge compared with all other racial groups. When examined further, we saw that the interaction of race and clinical indication was significant, with NH black patients having markedly higher probability of in-hospital death when presenting with EVB. There are a number of likely explanations for this result. Previous studies have identified disparities in varix management.19 20 While rates of endoscopy for variceal haemorrhage are similar for whites and blacks, black patients are significantly more likely to undergo delayed endoscopy when presenting with EVB.19 Similarly, in our study, we found significant variation in pre-procedure LOS, with non-white patients generally having longer times from admission to TIPS. Timely variceal screening following the diagnosis of cirrhosis also occurs less often in the black population.20 Most likely, a combination of factors, including those listed, are contributing to the drastically worse outcomes following TIPS among black patients.
Interestingly, NH black patients also had disproportionately low representation in our study. The NIS is a nationally representative database with weighting designed to reflect the US population.17 Despite representing ~29% of the US cirrhotic population and ~10% of US cirrhotic admissions, under 6% of TIPS procedures in our study were performed for NH black patients.19 21 Earlier studies have also found lower rates of portosystemic shunt creation in the black population compared with other races/ethnicities, raising important concerns about equity of access to care in the end-stage liver disease (ESLD) population.19
Unfortunately, racial and ethnic disparities in ESLD care are not new to the literature. Access to adequate ESLD care in traditionally underserved populations has been of increasing concern in recent years. Studies have shown that black patients are less likely to receive transplant or treatment for hepatocellular carcinoma,15 22 and are referred to transplant centres at lower rates for their ESLD care.13
Our results also have prognostic value for clinicians. In addition to the race-related findings, our model found that those with higher comorbidity scores and those presenting non-electively are at higher probability of in-hospital death. Although not surprising, these factors should be considered when counselling patients and families prior to TIPS.
There are some notable weaknesses to this study. First, our model only addressed the primary outcome, in-hospital mortality. Risk stratification and prognostic counselling for TIPS should be all-encompassing and personalised to individual clinical scenarios, with both risks and benefits considered.4 23 24 In our study, other notable complications of the TIPS procedure, namely intractable hepatic encephalopathy, could not be measured. Our study also used a hierarchical approach for determining procedure indication. Although precedent exists for this method in earlier literature,12 it would be unreasonable to think that the true indication for all procedures matched that assigned by the hierarchy. Further, this study was conducted using administrative data. In addition to common coding and analysis issues within such datasets, conclusions from studies conducted using this database are limited by the absence of laboratory data. Future centre-based studies incorporating clinical data could provide clearer insight into the disparities observed. Finally, the dataset in this study is from the years 2012–2014. Given the lapse in time from data collection to present, there is a possibility that changes in TIPS utilisation over time could affect the current relevance of conclusions presented in this study. Although possible, the authors feel a change in utilisation is relatively unlikely. Multiple prior studies demonstrated that annual TIPS volume did not change significantly in the years preceding this study.11 12 Furthermore, if changes in TIPS utilisation have occurred, the trend is likely towards more aggressive use, which, if present, would be unlikely to correct racial disparities in access to and outcomes after TIPS, and may even amplify these disparities.
Altogether, this study presents important and concerning findings in ESLD care. There are clear disparities in outcomes following TIPS. Our research also contributes to a growing body of literature suggesting racial disparities in access to care exist for patients with ESLD. In the broader context of the American healthcare system, this finding sadly comes with little surprise. In June 2018, the American Medical Association declared they would establish a new entity to work to improve healthcare equity in the USA.25 Moving forward, it will be important to identify both cultural barriers to care and sociodemographic factors that may be augmenting this trend if we hope to improve liver disease care across all racial and ethnic groups.
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. Data for the years 2012–2014 were obtained from the National Inpatient Sample, a database constructed by the Agency for Healthcare Research and Quality (AHRQ) Healthcare Cost and Utilization Project (HCUP). This database is publicly available for purchase on the HCUP website.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All authors contributed meaningfully to this work. JHH: study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis; study supervision. AP: analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis. DN: analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis. CYK: analysis and interpretation of data; critical revision of the manuscript for important intellectual content. YAP: critical revision of the manuscript for important intellectual content. JMW: analysis and interpretation of data; critical revision of the manuscript for important intellectual content. AJM: study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; study supervision; responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests CYK has received consulting fees from Boston Scientific, BD, and Humacyte. YAP has received consulting fees from Intercept Pharmaceuticals. JMW has received research funding from Gilead, Sequana, Mirum Pharmaceuticals, and BMS. He has received consulting fees from Science 37, Gilead and Viral ED. AJM has received research funding from Abbvie, CymaBay, Gilead, Intercept, Novartis and Taiwan J. He has served on advisory boards for Abbvie, Gilead and Pilant. He has received consulting fees from Pfizer and High Tide.
Provenance and peer review Not commissioned; externally peer reviewed.