Article Text

Abstract
Objective The Visceral Adiposity Index (VAI) is a marker of visceral fat accumulation and dysfunction. We aimed to investigate the association between VAI and incident colorectal cancer (CRC).
Design In this historical cohort study of 27 921 (16 434 men and 11 487 women) participants, we divided the participants into tertiles according to VAI. We calculated VAI: men, VAI = (waist circumference (WC)/(39.68+1.88 × body mass index (BMI))) × (triglycerides (TG)/1.03) × (1.31/high-density lipoprotein cholesterol (HDL)); women, VAI = (WC/(36.58+1.89 × BMI)) × (TG/0.81) × (1.52/HDL). We performed Cox proportional hazard models, adjusting for sex, age, smoking, alcohol consumption, exercise, haemoglobin A1c and systolic blood pressure.
Results During the median 4.4-year follow-up, 116 participants developed CRC. Compared with the lowest tertile, the HRs of incident CRC in the middle and the highest tertiles were 1.30 (95% CI 0.76 to 2.28, p=0.338) and 2.41 (1.50 to 4.02, p<0.001) in univariate analysis. Moreover, the HRs of incident CRC in the middle and the highest tertiles were 1.27 (0.73 to 2.23, p=0.396) and 1.98 (1.15 to 3.39, p=0.013) after adjusting for covariates.
Conclusions VAI can be a predictor of incident CRC. For early detection, we should encourage people with high VAI to undergo screening for CRC.
- colorectal cancer
- epidemiology
- obesity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known about this subject?
The Visceral Adiposity Index (VAI) is a marker of visceral fat accumulation and dysfunction. Visceral fat accumulation is related with incident colorectal cancer (CRC).
What are the new findings?
VAI can be a predictor of incident CRC.
How might it impact on clinical practice in the foreseeable future?
For early detection of incident CRC, we should encourage people with high VAI to undergo screening for CRC.
Introduction
Cancer is the leading cause of death in the world1 and colorectal cancer (CRC) is one of the most common cancers next to lung and breast cancer in the world. The most efficient strategies to reduce CRC incidence include identifying risk markers for CRC and performing a preventive colonoscopy in high-risk populations.
Metabolic syndrome, that is, obesity, impaired glucose tolerance, hypertension and dyslipidaemia, has been reported to be associated with risk of CRC by several studies.2–6 Particularly, it is well known that obesity and CRC were associated with each other.7–9 Furthermore, visceral fat accumulation, which is the central pathogenesis of obesity, plays a critical role in the pathogenesis of CRC.10 11
Visceral Adiposity Index (VAI) has been proposed as a reliable marker of visceral fat accumulation and dysfunction.12 In addition, VAI is reported to be associated with cytokines levels and can be a maker of chronic inflammation. Chronic inflammation has been reported to be involved in the development of diseases such as metabolic syndrome and cancer,13 14 and in fact, VAI has been proved a strong association with type 2 diabetes,15 chronic kidney disease16 and cardiovascular events.12 17 Thus, there is a possibility that VAI is associated with risk of incident CRC. However, no previous studies investigated this association. In this retrospective study, we investigated the impact of VAI on incident CRC.
Materials and methods
Study participants and study design
We investigated the impact of VAI on the risk of incident CRC in this population-based longitudinal study of a medical check-up programme at Asahi University Hospital (Gifu, Japan) which is called the NAfld in the Gifu Area, Longitudinal Analysis (NAGALA) study. This cohort investigation has been ongoing and aims to detect chronic diseases and their risk factors, and to promote public health. The detail of NAGALA study and medical examination programmes was expressed elsewhere.18 In this study, we selected the data of the individual who participated in this medical examination programme from 2003 to 2016 and received more than two times. The exclusion criteria were as follows: the participants whose data, including high-density lipoprotein (HDL) cholesterol and alcohol consumption, were missed and the participants who diagnosed with CRC at the first visit or with a history of CRC in the past. All of the participants in this study provided their informed consent to participate.
Data collection and measurements
We obtained the medical history and the data of smoking status, alcohol consumption and physical activity from all of the participants by a standardised self-administered questionnaire.18 We evaluated alcohol consumption by the questionnaire about the type and amount of alcohol consumption per week during the prior month, then estimated the mean ethanol intake per week. We categorised the participants into the following four groups: no or minimal alcohol consumer, <40 g/week; light, 40–140 g/week; moderate, 140–280 g/week; or heavy alcohol consumer, >280 g/week.19 The participants were categorised into three groups by smoking status: non-smoker, ex-smoker, or current smoker. The participants’ recreational and sports activities were also inquired in the questionnaire. We defined regular exercisers as participants who played any type of sports over one time per week regularly.20
VAI formulas
We calculated VAI using the formulas12: men, VAI = (waist circumference (WC)/(39.68+1.88 × body mass index (BMI))) × (triglycerides (TG)/1.03) × (1.31/HDL); women, VAI = (WC/(36.58+1.89 × BMI)) × (TG/0.81) × (1.52/HDL). Both TG and HDL levels are expressed in mmol/L.
Identification of cases of CRC
In this health check-up programme, faecal occult blood test was included. When the faecal occult test was positive and the presence of CRC was suspected, the participants were noticed and were encouraged to receive further examinations to diagnose it. We gathered the medical information regarding CRCs by a standardised letter from a hospital where a participant receives further examinations. Besides, we included participants who received further examinations for reasons other than occult blood test and were diagnosed as CRC. The gastroenterologist checked the gathered information and defined them as CRC. From 1 January 2004, we adopted the standardised letter. Then, we set the study period as 1 January 2004 to 31 December 2016. The primary endpoint in this study was set as incident CRC. In this study, we defined the day when participants were suggested as cancer at the health check-up centre as the onset day if participants were diagnosed as CRC.
Statistical analysis
The data were analysed with the JMP V.13.0 software (SAS), and p values < 0.05 were considered significant. We expressed values as mean (SD) or median (IQR) for continuous variables and number (%) for categorical variables. We evaluated the p values using one-way analysis of variance (ANOVA) for continuous variables and χ2 test for categorical variables, respectively. Moreover, the number of incident CRC was small; therefore, we categorised the participants into three groups according to tertiles of VAI: less than 0.58 (the lowest tertile), more than or equal to 0.58 and less than 1.15 (the middle tertile), more than or equal to 1.15 (the highest tertile). Categorical variables were compared among the groups by Pearson’s χ2 test, and continuous variables were compared by one-way ANOVA and Tukey honestly significant difference test, respectively. In addition, model assumptions were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria).
We used a Kaplan-Meier analysis to obtain a graphical presentation of time to incident CRC, and the log-rank test to evaluate differences among tertiles according to the VAI. We performed a Bonferroni correction and considered p values < 0.0083 significant in the log-rank test. Because a previous study used the VAI as tertiles,21 we divided the participants into tertiles.
Cox proportional hazard models were used to calculate adjusted HR and 95% CI for incident CRC according to three categories of VAI. We adjusted for sex, age, smoking status, alcohol consumption, exercise habit and systolic blood pressure (SBP). Proportional hazards could be assumed in all covariates (online supplementary table 1). Moreover, because there is a possibility that the individuals who have CRC lost their weight before diagnosis, a sensitivity analysis excluding the first year or two of follow-up was performed. Visceral fat levels and CRC incidence vary between men and women, and we also performed a sex-specific analysis.
Supplemental material
Results
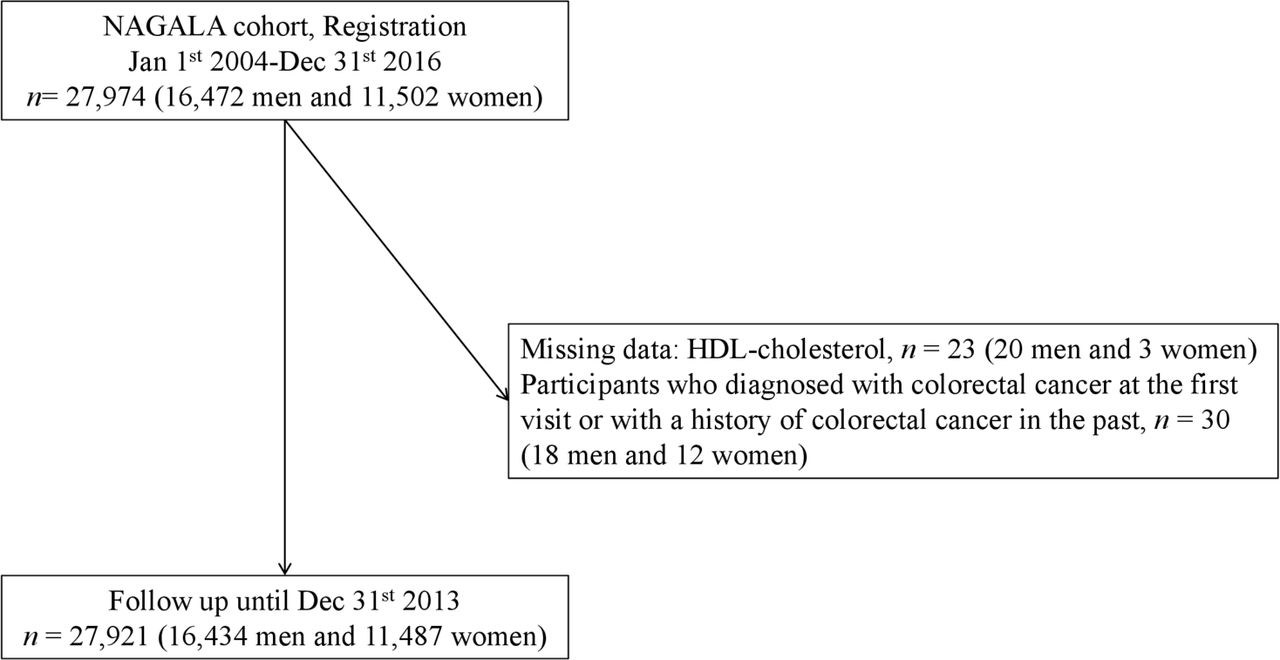
From 1 January 2004 to 31 December 2016, 27 974 (16 472 men and 11 502 women) participants were registered in NAGALA cohort. After we excluded 53 participates because of exclusion criteria, 27 921 (16 434 men and 11 487 women) participants were entered in this study (figure 1).

Study flow diagram for the registration of participants. HDL, high-density lipoprotein; NAGALA, NAfld in the Gifu Area, Longitudinal Analysis.
The baseline characteristics of the participants are summarised in tables 1 and 2.
Clinical characteristics of participants and participants in three groups based on tertile of Visceral Adiposity Index (VAI)
Cox proportional hazards for incident colorectal cancer
Mean age of participants was 45.7±10.1 years old and BMI was 22.6±3.3 kg/m². Age, BMI, WC, fasting plasma glucose, haemoglobin A1c, TG, total cholesterol, aspartic aminotransferase, alanine aminotransferase, γ-glutamyl transpeptidase, SBP and diastolic blood pressure of the highest tertile were the highest, followed in order by the middle and the lowest tertile. On the other hand, HDL cholesterol of the highest tertile was the lowest. Even after excluding the first year or two of follow-up, the tendency did not change (online supplementary table 2).
Supplemental material
During the median 4.4-year follow-up, 116 participants were diagnosed as CRC. The 4000 days’ cumulative incidence rates of CRC were 0.2% in the lowest tertile, 0.4% in the middle tertile and 0.6% in the highest tertile. Compared with the lowest tertile, the highest tertile showed a significantly higher risk of incident CRC (p<0.001; figure 2).

{kind=link}
{kind=link}
Kaplan-Meier analysis of incident colorectal cancer (CRC). Log-rank tests were used to determine the association among the Visceral Adiposity Index tertiles. Bonferroni correction was performed to correct familiar error, and a p value <0.0083 was considered significant. Compared with the lowest tertile, the highest tertile showed a significantly higher risk of incident CRC (p<0.001), and the middle tertile did not (p=0.562). Compared with the middle tertile, the highest tertile did not show a significantly higher risk of incident CRC (p=0.122).
Compared with the lowest tertile, the HRs of incident CRC in the middle and highest tertile were 1.30 (95% CI 0.76 to 2.28, p=0.338) and 2.41 (1.50 to 4.02, p<0.001) in univariate analysis. Moreover, the HRs of incident CRC in the middle and highest tertile were 1.14 (0.65 to 1.99, p=0.646) and 1.78 (1.05 to 3.02, p=0.032) after adjusting for covariates (table 2). Even after excluding the first year or two of follow-up, the HR of incident CRC in the middle and highest tertile was 1.14 (95% CI 0.65 to 1.99, p=0.338) and 1.78 (1.05 to 3.02, p=0.032), compared with the lowest tertile after adjusting for covariates (online supplementary table 3). The highest VAI tertile showed a significant risk for incident CRC, compared with the lowest tertile (HR: 3.98, 95% CI 1.76 to 9.01, p<0.001) in women. The highest VAI tertile tended to be associated with a risk for incident CRC, compared with the lowest tertile in men (1.67, 0.92 to 3.24, p=0.091), although it did not reach statistically significance.
Supplemental material
Discussion
In this retrospective cohort study of over 27 000 Japanese participants, we investigated the impact of VAI on incident CRC. Our study revealed that the risk of incident CRC in the participants with the highest VAI group was significantly higher than those with the other VAI groups. VAI, calculated with BMI, HDL cholesterol, TG and WC, was originally proposed as a diagnostic tool for cardiovascular and cerebrovascular events,12 and some following studies demonstrated the association between high VAI score and incident cardiovascular disease,22 23 type 2 diabetes15 and hypertension.24 To our knowledge, the present study is the first investigation to clarify the impact of VAI on incident CRC.
Since VAI is associated with visceral fat accumulation and dysfunction,12 some potential explanations are proposed to support our findings. Several previous studies reported the association between visceral fat accumulation and CRC from the viewpoint of decreased adiponectin,10 25 26 increased adipocytokines including tumour necrosis factor −α and interleukin 6,27 28 ,29 insulin resistance8 11 and oxidative stress.
First, adiponectin is reported to be negatively associated with visceral fat accumulation.10 25 26 Sugiyama et al demonstrated that adiponectin inhibits the growth of CRC via AMPK/mTOR pathway.30 In addition, Moon et al reported that adiponectin administration suppressed tumour growth and angiogenesis in tumours by regulation of adenosine monophosphate-activated protein kinase (AMPK)/S6, STAT3/vascular endothelial growth factor (VEGF) and p21/p27/p53/cyclins signalling pathway.31 Therefore, adiponectin levels in the highest VAI group might be lower than those in the other groups and decreased antitumour effect due to low adiponectin levels might increase the incident CRC.
Second, adipocytokines were also reported to be related with the pathogenesis of CRC.27 28 Tumour necrosis factor-α and interleukin 6 were revealed to elevate in visceral fat obesity.32 33 Additionally, Gu et al34 reported that VAI is positively associated with the levels of tumour necrosis factor-α, interleukin 6 and C-reactive protein. In fact, C-reactive protein levels were positively associated with VAI in this study (r=0.190, p<0.001 by Spearman’s rank correlation coefficient). Inflammation of adipose tissue is caused by macrophage infiltration which is mediated by tumour necrosis factor-α and interleukin 6, and causes dysregulation of the secretion of adipocytokines, which leads to insulin resistance.35 36 Moreover, insulin resistance plays a key role in the pathogenesis of CRC.8 11 Insulin resistance induces hyperinsulinaemia and increases levels of insulin-like growth factors, which activates PI3K/Akt/mTOR/S6K signalling pathway in cancer.37 Moreover, several previous studies showed the association between increased VAI and reduced insulin sensitivity.15 38 Taken together, dysregulation of adipocytokines and insulin resistance in the highest VAI group reflecting visceral fat dysfunction may be associated with incident CRC.
Lastly, the association between visceral fat adiposity and oxidative stress has been reported28 and the association between oxidative stress and pathogenesis of CRC via DNA damage and cancer progression has been demonstrated by many groups.39–42 Visceral fat accumulation might cause oxidative stress, which progress cancer growth. Furthermore, oxidative stress was reported to lead to insulin resistance by upregulation of genes involved in sterol regulatory element binding protein 1c-related fatty acid synthesis and peroxisome proliferator-activated receptor alpha-related fatty acid oxidation,43 44 which is different pathway from dysregulation of adipocytokines, and might induce cancer progression.
The strengths of our study include using the standardised questionnaire for lifestyle factors,45 and the relatively large population-based longitudinal research. Our study also has some limitations. First, we did not perform colonoscopy to all participants. In addition, the proportion of the participants who received further examinations out of the participants whose faecal occult tests were positive was approximately only 50%. Therefore, there was a possibility that the number of incident CRC was underestimated. However, CRC incidence available for all generations in Japan is 0.2%46; on the other hand, that in this study is 0.4%. Therefore, underestimation of incident CRC might be smaller than expected. Additionally, in this cohort, re-examination rate was 70 %; therefore, the possibility that the incidence of CRC is included in the follow-up loss cannot be ruled out. Second, we did not have the data of invasion depth or histopathological type of CRC. If we had the data, we could analyse from a different perspective. Third, we did not have the data of plasma insulin concentration to evaluate insulin resistance such as homeostasis model assessment insulin resistance, which might determine the relation between VAI and insulin resistance in the development of CRC more accurately. Fourth, we had a limited ability to examine different levels of physical activity on incident CRC. In addition, we did not have the data of diet. Dietary habits such as red meat, processed meat, fibre, calcium, vitamin D, were reported to be risk for incident CRC. If we can evaluate the frequency and intensity of exercise or dietary habit, more accurate analysis would be possible. If we can evaluate the frequency and intensity of exercise, more accurate analysis would be possible. Lastly, the generalisability of our study to non-Japanese populations is uncertain.
In conclusion, we have shown that VAI could be a predictor of incident CRC. For early detection of CRC, we should encourage people with high VAI to undergo screening for CRC.
Acknowledgments
The authors thank all of the staff members in the medical health check-up centre at Asahi University Hospital.
References
Footnotes
Contributors TO contributed to the data research and analyses and wrote the manuscript. YH originated and designed the study, analysed the data and reviewed the manuscript for intellectual content. MH contributed to data research and the manuscript organisation and reviewed and edited the manuscript. AO and TK contributed to originate the study, data research and contributed to the discussion. MF analysed the data and reviewed and edited the manuscript. MH is the guarantor of this work and, as such, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors were involved in the writing of the manuscript and approved the manuscript’s final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests YH received grants from Asahi Kasei Corporation outside the submitted work. MF received grants from AstraZeneca, Astellas Pharma, Nippon Boehringer Ingelheim Co., Daiichi Sankyo Co., Eli Lilly Japan K.K., Kyowa Hakko Kirin Co., Kissei Pharmaceutical Co., MSD K.K., Mitsubishi Tanabe Pharma Corp., Novo Nordisk Pharma, Sanwa Kagaku Kenkyusho Co., Sanofi K.K., Ono Pharmaceutical Co., and Takeda Pharmaceutical Co., outside the submitted work. The sponsors were not involved in the study design; in the collection, analysis, interpretation of data; in the writing of this manuscript; or in the decision to submit the article for publication. The authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article. The authors declare that although they are affiliated with a department that is supported financially by pharmaceutical company, the authors received no current funding for this study, and this does not alter their adherence to all the journal policies on sharing data and materials.
Patient consent for publication Not required.
Ethics approval The present study was approved by Asahi University Hospital’s Ethics Committee and was based on Declaration of Helsinki. Approval number is 2018-09-01.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.