Article Text

Abstract
Objective Hepatocellular carcinoma (HCC) incidence in the UK trebled between 1997 and 2017. With increasing numbers requiring treatment, understanding the likely impact on healthcare budgets can inform service planning and commissioning. The aim of this analysis was to use existing registry data to describe the direct healthcare costs of current treatments for HCC and estimate the impact on National Health Service (NHS) budgets.
Design A retrospective data analysis based on the National Cancer Registration and Analysis Service cancer registry informed a decision-analytic model for England comparing patients by cirrhosis compensation status and those on palliative or curative treatment pathways. Potential cost drivers were investigated by undertaking a series of one-way sensitivity analyses.
Results Between 1 January 2010 and 31 December 2016, 15 684 patients were diagnosed with HCC. The median cost per patient over 2 years was £9065 (IQR: £1965 to £20 491), 66% did not receive active therapy. The cost of HCC treatment for England over 5 years was estimated to be £245 million.
Conclusion The National Cancer Registration Dataset and linked data sets have enabled a comprehensive analysis of the resource use and costs of secondary and tertiary healthcare for HCC, providing an overview of the economic impact to the NHS England of treating HCC.
- HEPATOCELLULAR CARCINOMA
- HEALTH ECONOMICS
- LIVER
- CANCER REGISTRIES
Data availability statement
Data are available upon reasonable request. The data in this study were collected and analyzed under the National Disease Registries Directions 2021, made in accordance with sections 254(1) and 254(6) of the 2012 Health and Social Care Act. This study uses data that has been provided by patients and collected by the NHS as part of their care and support. The data are collated, maintained and quality assured by the National Disease Registration Service, which is part of NHS Digital. https://digital.nhs.uk/ndrs/about/ncras.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Hepatocellular carcinoma is the most common type of primary liver cancer and incidence is increasing. Objective, quantifiable evidence on the cost of management of hepatocellular carcinoma could aid service planning and efficient allocation of resources.
WHAT THIS STUDY ADDS
This is the first comprehensive description of the costs of management of hepatocellular carcinoma to the National Health Service (NHS) in England based on a linked patient-level, population-based registry data set. Cost impact for secondary and tertiary healthcare for hepatocellular carcinoma over 5 years was estimated to be £245 million for England.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Given the cost impact of managing hepatocellular carcinoma, increased investment in health education and early diagnosis is likely to be beneficial not only to the NHS but also across society given the impacts on patient’s lives and their families.
Introduction
Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer.1 Incidence of HCC trebled between 1997 and 2017 (age-standardised incidence rate 1.8 to 5.5 per 100 000).2 Diagnosis of HCC usually happens at an advanced stage of cancer and/or liver disease, such that curative treatments are no longer options, and the majority do not live longer than 1 year after diagnosis.3 4 However, earlier diagnosis, when curative treatment can be offered, may be associated with increased 5-year survival of 50%–70%.4 5
The National Cancer Registration and Analysis Service (NCRAS) collates the population-based cancer registry for England with data collected on every primary tumour diagnosed in the National Health Service (NHS) from sources such as multidisciplinary team meetings, pathology reports, treatment records and hospital activity records.6 The Cancer Outcomes and Services Dataset (COSD) is the national standard for items to be reported by service providers in the NHS in England, specifying information on items such as waiting times, screening programmes and mortality data; the National Cancer Registration Dataset includes a subset of the COSD.6 7 Other datasets managed by NCRAS and linked to the National Cancer Registration Dataset are the National Radiotherapy Dataset and the Systemic Anti-Cancer Therapy Dataset (SACT).8 9 Mortality data are supplied by the Office of National Statistics10 and hospital episode statistics (HES) from NHS Digital.11
With limited budgets available within the NHS and increasing incidence of HCC, it is essential that investment in services is based on objective quantifiable evidence to provide efficient allocation of resources. Using existing data sources to provide insight into the cost impact of HCC will allow the NHS and other organisations to access up-to-date evidence to help plan and deliver services. The HCC-UK research group and NCRAS developed a programme of research based on these rich, population-based data. As part of this research, analyses were developed to quantify the impact of HCC to the NHS budget in England.
Aim of the study
The primary objective was to identify patient pathways from first diagnosis of HCC using routinely available data. The secondary objective was to describe the associated healthcare resource use and costs of the patient pathways to determine the economic burden to the NHS in England.
Methods
A retrospective descriptive data analysis of resource use was undertaken for patients aged ≥18 years and diagnosed with HCC in England, defined as International Classification of Diseases for Oncology (ICDO) code 8170 (HCC); or an ICD10 code C220 (liver cell carcinoma) and either an ICDO code 8000 (neoplasm, malignant), 8001 (Tumour cells, malignant) or 8010 (carcinoma, NOS), recorded in the National Cancer Registration Dataset between 2010 and 2016.
The National Cancer Registration Dataset contains patient, tumour, treatment information and route to diagnosis and is a subset of the COSD, linking to treatment data including surgery, chemotherapy and radiotherapy. The National Cancer Registration Dataset is linked to HES, which records inpatient admissions, outpatient appointments and accident and emergency attendances. These data were used to describe the resource use at a patient level for secondary and tertiary care, primary care is not reported in these datasets.12 A NHS England perspective was taken for the analysis.13
Date of diagnosis was assigned in the registry using the European Network of Cancer Registries rules. This date can be reassigned within 3 months of the initial assignment if a higher priority event occurs, such as initial diagnosis by imaging and subsequent histological diagnosis, although this should not be later than the date of initial treatment.14 Therefore, resource use 90 days prior to diagnosis was captured to account for any HCC-related events in the lead up to registry date of diagnosis. All diagnosis codes were requested as part of the dataset including those related to the liver. Recognising that the majority of patients with HCC would have significant underlying liver damage and that the codes were not specific enough to separate resource use for HCC from that due to underlying cirrhosis, it was agreed with the HCC-UK research team that patients with HCC should be stratified by their cirrhosis status, defined using the algorithm developed by Driver et al.15 Patients were designated as having compensated cirrhosis, decompensated cirrhosis or non-cirrhotic or with unknown cirrhosis status.
Given that 2-year survival for people with HCC is less than 34%, a 2-year follow-up period (to 31 December 2018) was assumed sufficient to capture most HCC treatments.16 17 Survival time was calculated from date of diagnosis to death (event) or to the end of the 2-year follow-up period (censored alive) using Kaplan-Meier survival analysis. Median survival, SE and 95% CIs were calculated. Survival was stratified by cirrhosis status and the difference in survival between groups was tested using the Breslow (generalised Wilcoxon) test.
Healthcare costs
Using the relevant healthcare resource use group code, each resource item was costed (£ sterling) using the appropriate annual NHS Reference Costs, from 2010/2011 through to 2018/2019, and inflated to 2018/2019 costs.18–20 The SACT data for Sorafenib were incomplete; therefore, published literature was identified to inform the length of treatment and mean dose. A UK audit of Sorafenib reported the median treatment time as 3.6 months and mean daily dose of 590 mg.21 The cost for Sorafenib was calculated as £95.80 for 600 mg per day (£3 576.56, 112×200 mg tablets).22 As this cost was for 2020 prices, lower costs for Sorafenib were tested in a sensitivity analysis. The HES data correspond to the recipient patient only; with organ transplant, there are costs for the donor and transport of the liver. A targeted literature search of costs related to organ transplant identified a health technology assessment of lung transplant in the UK with detailed costs related to the organ recipient, donor and transport (online supplemental table 5).23 It has been assumed that costs are the same regardless of the organ donated as several organs may be retrieved during surgery.23
Supplemental material
Some medications for immunosuppressive therapy after liver transplant are high-cost drugs and are excluded from the Payment by Results tariff.24 A targeted literature search of immunosuppressive therapy for liver transplant identified a cost-utility analysis of tacrolimus.25 The reported doses of each medication related to liver transplant were cross-checked with the British National Formulary and the Electronic Medicines Compendium.22 26 Tacrolimus, ciclosporin and mycophenolate mofetil were all listed as high-cost drugs, medications not listed as high-cost drugs were assumed to be included in the HES costs (online supplemental tables 6–9). The starting doses immediately after transplant were tapered linearly over the following year to give a final dose maintained in subsequent years. Mean patient bodyweight was estimated at 77.2 kg (SD=16.2 kg) for calculation of mean daily dose.
To ensure that the resource and cost impact of HCC is presented as the impact at each point in time, discounting was not applied.13
Modelling
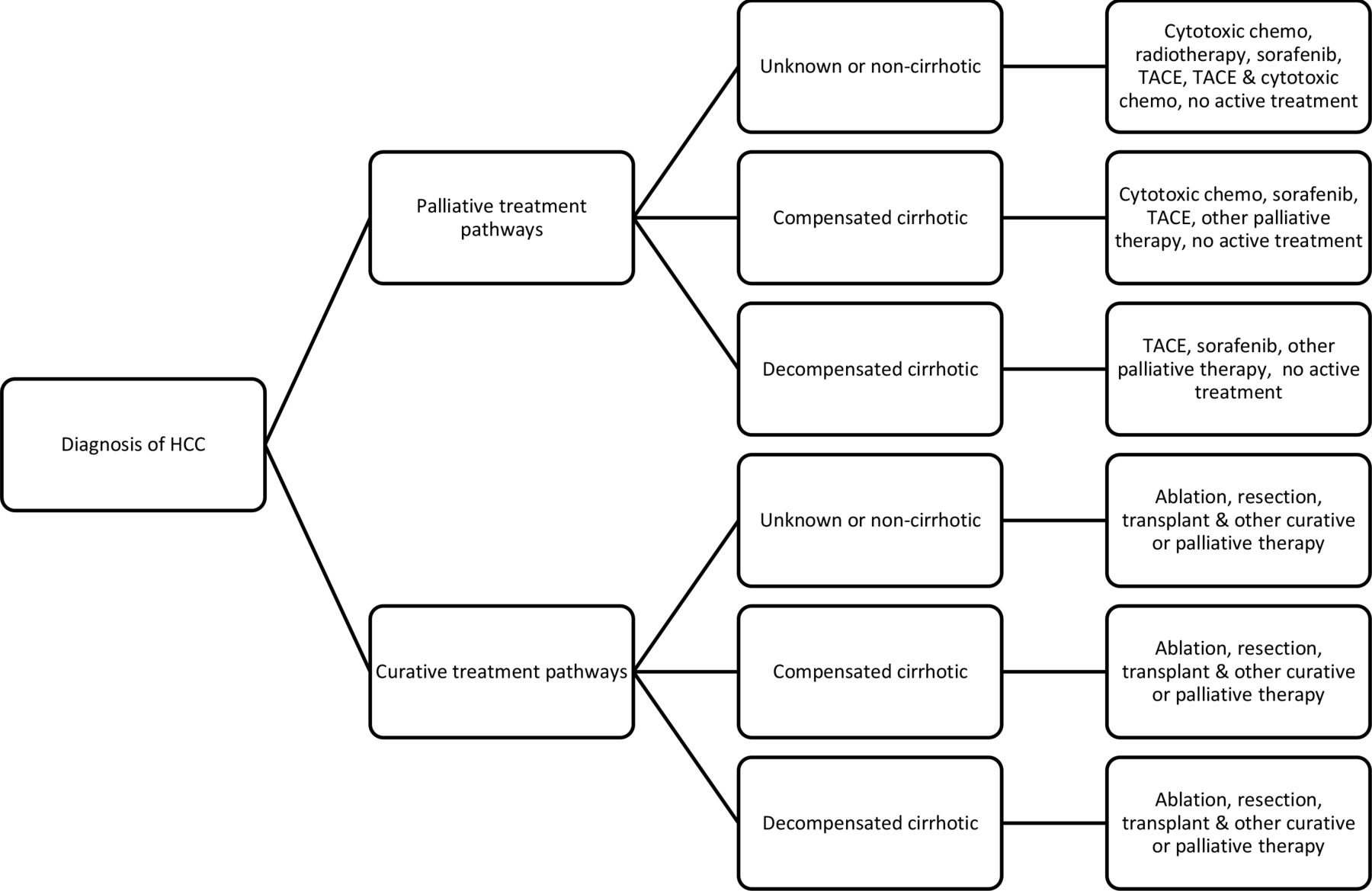
A decision-tree model was constructed using Microsoft Excel (V.365, 2020)(figure 1).27 For the base case, patients entered the model at the point of diagnosis of new HCC or the date of first HCC-related treatment, whichever came first. The period 90-days prior to diagnosis or first HCC treatment was included as a sensitivity analysis. Patients in receipt of ablation, liver resection or liver transplant at any point during follow-up were assumed to be receiving potentially curative treatment. If the patient did not receive any of the three curative treatments, they were assumed to be on a palliative care pathway. Patients were further stratified by their compensation status. The resource use and costs associated with each stage of the patient pathway were applied in the model.
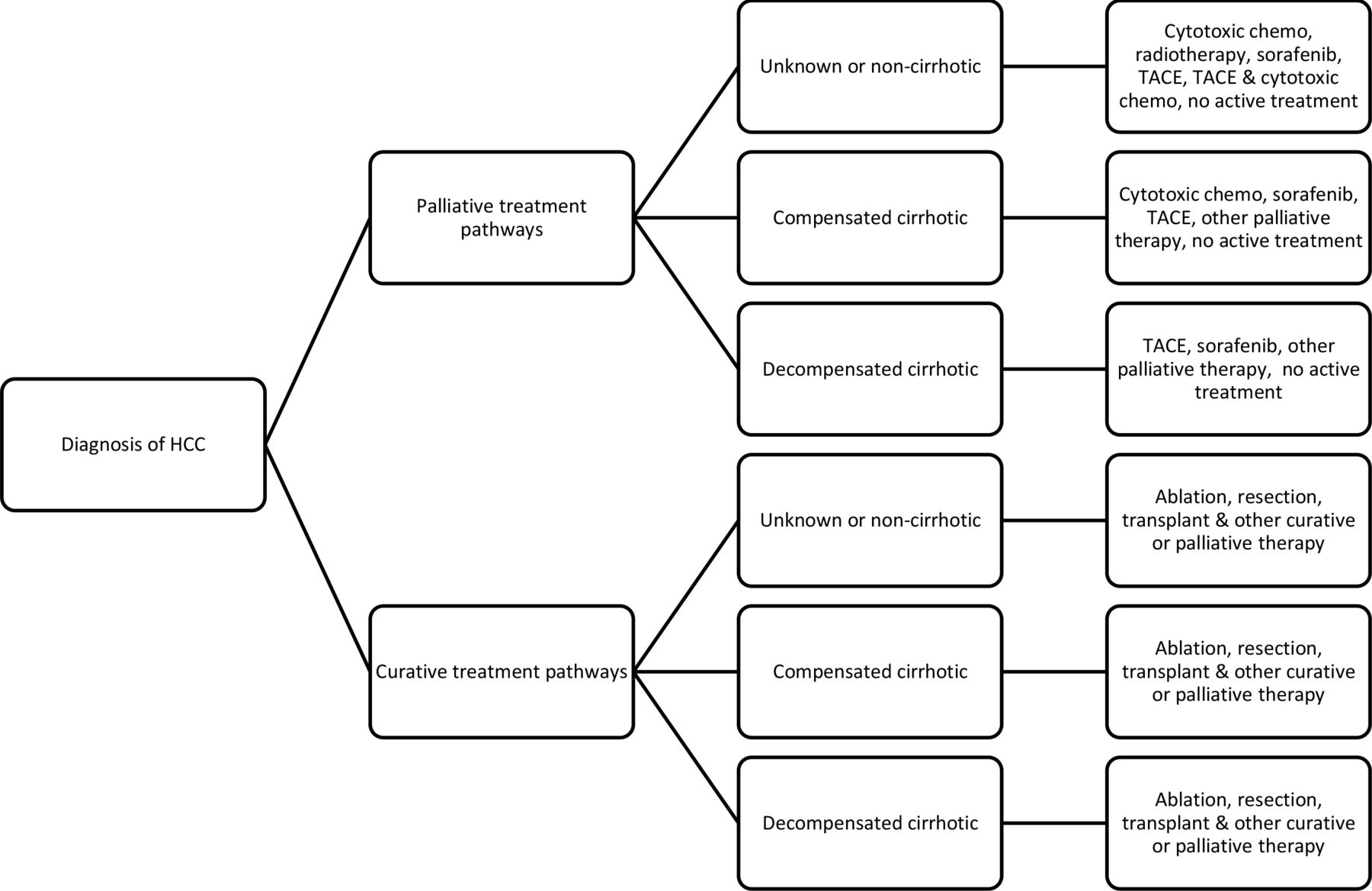
Schematic diagram of the economic impact model. TACE, Transarterial chemoembolisation.
All patient pathways, irrespective of patient numbers, were considered for first treatment. For subsequent treatments, if the number of patients in a pathway was less than 50, the pathways were combined to categories ‘other palliative’ and ‘other curative’ (online supplemental table 10). The probabilities of receiving treatments within each patient pathway were obtained from analysis of the main HCC dataset. The time horizon for the initial analysis was 2 years.
The base case population simulated the cohort of newly diagnosed patients in England in 2016, using the mean age standardised rate of 5.25 per 100 000 and the English population of 56 606 624 (n=2971).2 28 This method was used rather than the actual number of new diagnoses each year since it is generalisable and easily up scaled to the UK population using the incidence of HCC in the constituent countries.
To extrapolate to 5 years, it was assumed that any patients who were still alive at the end of their 2-year follow-up period were placed on best supportive care, represented by the average cost of all palliative treatments over the second year of treatment (costs in year 1 were substantially higher than year 2; therefore, year 2 costs would be more representative of future costs). The number of days to death was used to calculate mortality each year.
All statistical analyses were non-parametric, due to the skewed nature of the cost data. Kruskal-Wallis tests were used to compare median costs when there were more than two groups and Mann-Whitney tests were used when there were exactly two groups. Statistical analysis was undertaken using STATA V.16.29
Scenario analyses
A set of alternative scenarios were constructed based on the expert opinion of the steering group. A probabilistic sensitivity analysis (PSA) was undertaken. Random sampling of the distributions of costs over 1000 simulations was used to calculate CIs and to understand the joint uncertainty around parameter impacts. Costs were assumed to follow the Gamma distribution in accordance with good practice.30
Results
Descriptive data analysis
Between 1 January 2010 and 31 December 2016, 15 684 people were diagnosed with HCC in England. Around half (N=8004, 51.0%) were categorised as non-cirrhotic or unknown cirrhosis status. Of those categorised with cirrhosis (N=7680, 49.0%), more had compensated cirrhosis (N=4098; 26.1%) than decompensated (N=3582; 22.8%).
The most common primary cause for hospitalisation was related to liver cell carcinoma (C220) (online supplemental table 4). In the non-cirrhotic or unknown cirrhosis status group the primary cause of hospital admission was two times as likely to be for liver cell carcinoma than for other causes (C220 N=10 050 vs N=4881 for other ICD10 codes). In the compensated cirrhosis group, again there were more hospital admissions for liver cell carcinoma (C220 N=7621 vs N=4550 other ICD10 codes), but for the decompensated cirrhosis group, although liver cell carcinoma was the most common cause for hospital admissions, there were more admissions for other reasons (C220 N=3741 vs N=6459 other ICD10 codes).
In the first line of therapy, 73.4% of patients had no active treatment, increasing to 91.9% of patients by the third line of therapy in the palliative pathways. A maximum of three treatments were considered as so few patients were receiving active treatment by the third line of therapy.
Healthcare costs
When examined by cirrhosis compensation status, median costs were higher for compensated compared with decompensated £14 038 (IQR: £5607, £27 174) vs £7744 (IQR: £1057, £20 241) (table 1). In the remaining patients, with unknown cirrhosis status or no cirrhosis, the median was £7304 (IQR: £1259, £17 293). The median values were significantly different from each other (p<0.001) with all pairwise comparisons also significant (p<0.001).
Overall deterministic cost analysis model results (N=2971 based on HCC incidence in 2016)
Patients receiving palliative care (80%) had a median cost of £6466 over 2 years (IQR: £973, £16 275), but curative care had a far higher average cost of £21 560 over 2 years (IQR: £12 116, £41 149) (difference between groups, p<0.001) (table 1). Although most patients received no active treatment once diagnosed with HCC, they did incur costs, a median of £2999 for unknown or non-cirrhotic status, £4585 for compensated cirrhotic patients and £4135 for decompensated cirrhotic patients (table 2).
Summary statistics and pathway probabilities for all patients (n=15 684) (Transarterial chemoembolisation (TACE))
First-year costs were higher than second-year costs (£33 966 284 vs £10 514 299), this is to be expected as patient mortality was high, 61% of patients died before the second year of treatment (table 3).
Summary cumulative costs of HCC treatment for NHS England over 5 years
For 2971 patients diagnosed with HCC in 2016 the total cost to NHS England for 2 years of treatment was £44 480 583 (table 3). The cost impact to the NHS England for a 5-year period, including new diagnoses, of secondary and tertiary care was estimated to be £245 million (table 3).
Scenario results
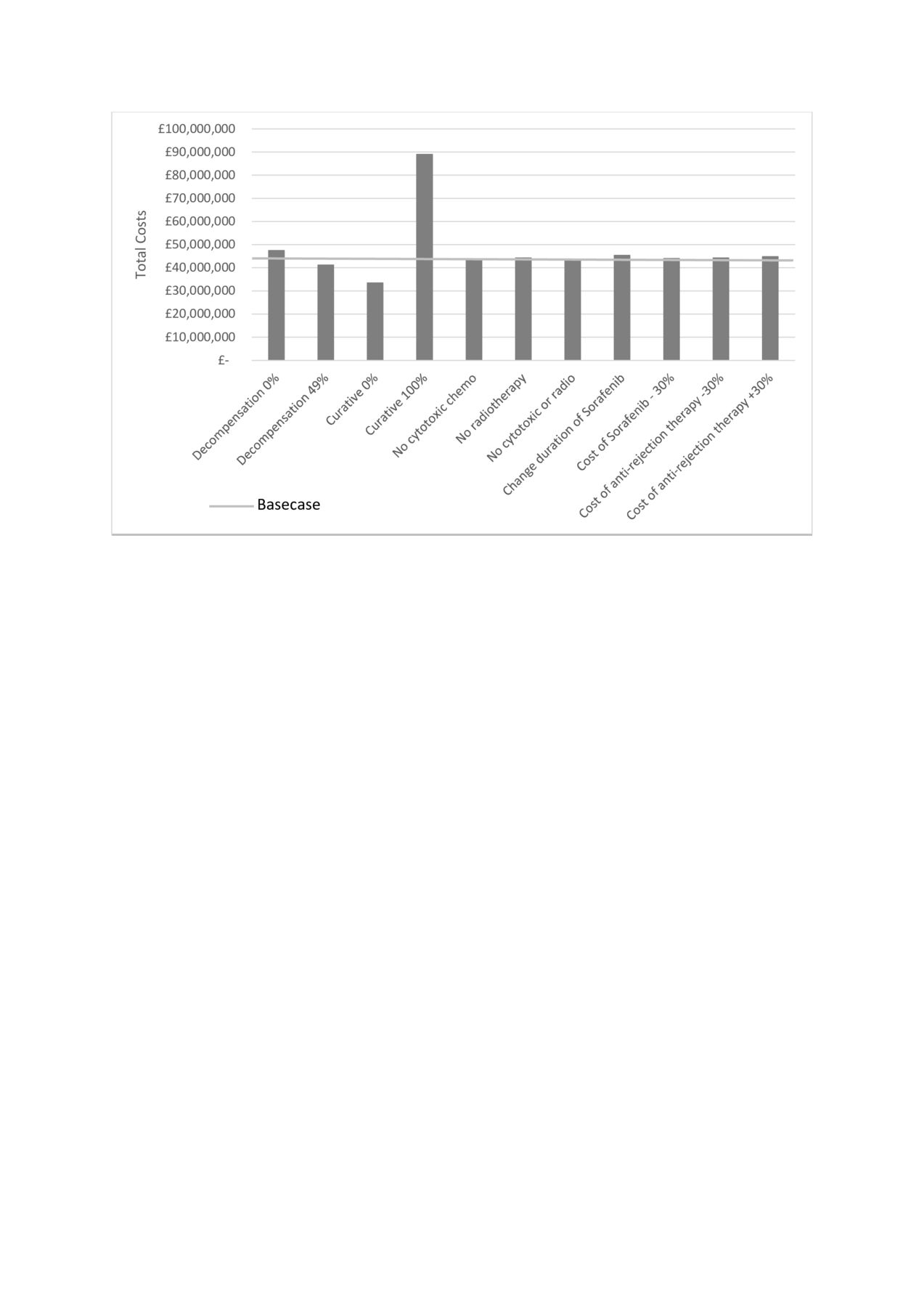
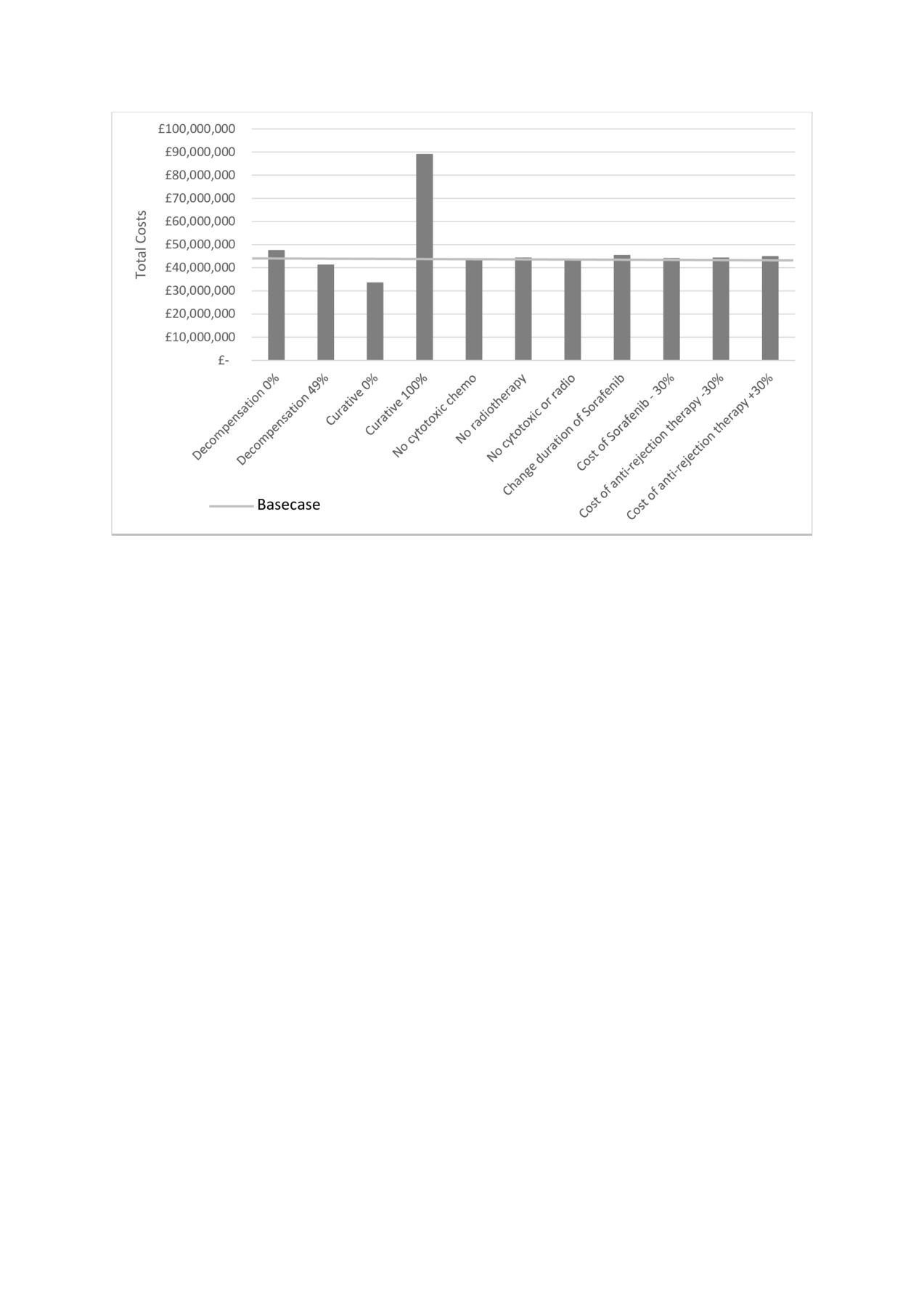
Figure 2 illustrates the total cost for all scenario analyses compared with the base case. The proportion of patients who receive treatment with palliative intent had the greatest influence, as they are the largest group. The percentage of patients with decompensated cirrhotic liver disease had limited impact on the total cost of treatment. Updating patient pathways with no cytotoxic chemotherapy or radiotherapy had a small effect on the total cost, as did changing the time that patients took Sorafenib, which may be more representative of current practice.
{kind=link}
{kind=link}
Total cost for HCC treatment for different scenarios, 2917 patients. HCC, hepatocellular carcinoma.
Probabilistic sensitivity analysis
A PSA was run on the cost data to capture the variability. The SD was taken to be 10% of the mean cost, this was done as the number of patients on each pathway was small and therefore the sample SD was not reliable. Over 1000 runs, the mean total cost of HCC over 2 years from diagnosis was £44 520 118 (95% CIs: £42 307 794, £46 732 443).
Survival analysis
Most patients with HCC (72.8%) died within 2 years of their diagnosis, median survival of 199 days post-diagnosis (95% CIs: 190, 208 days) (online supplemental figure 3). Cirrhotic status was significantly associated with survival, patients with compensated cirrhosis survived significantly longer than those with decompensated cirrhosis (439 days (95% CIs: 408, 470 days) vs 82 days (95% CIs: 75, 89 days), p<0.001)(online supplemental figure 3). Patients who were non-cirrhotic and with unknown cirrhosis status survived for a median of 188 days (95% CIs 177, 199 days).
Summary and discussion
This study used a large routine dataset to quantify the costs of management in secondary/tertiary settings of HCC to the NHS in England. The total cost for 2971 patients with HCC in the base case was £44 million for 2 years post-diagnosis. In patients who were non-cirrhotic or had unknown cirrhosis status (51%), the median cost per patient was £7304. The analysis showed that those with compensated cirrhosis incurred significantly greater healthcare costs than those with decompensated cirrhosis (£14 038 vs £7744 p<0.001). Compensated cirrhotic patients were more likely to receive potentially curative treatment at a higher cost (£21 560 vs £6466 over 2 years) than decompensated cirrhotic patients.
The UK biobank reported that late diagnosis of chronic liver disease was common, 79.1% to 86.9% of patients diagnosed with chronic liver disease in a population aged 40–69 years.31 Patients with decompensated cirrhosis had a significantly worse survival time than patients with compensated cirrhosis (82 days vs 439 days), indicative of the patient’s advanced disease progression and limited treatment options. Additionally, patients with decompensated cirrhosis had the highest costs in the 90-days pre-diagnosis.
Overall, the most common cause of hospital inpatient admissions given was HCC. For decompensated patients, the primary cause was associated with the underlying cirrhosis and liver conditions.
The 5-year results should be interpreted with appropriate caution as only secondary and tertiary costs are included, which is likely to underestimate the full cost of HCC. It was not possible to fully address the resource use and costs across the continuum of care for patients with HCC, for example, primary and community care setting. Productivity losses were considered but given the age of the patient population, it was assumed that a considerable proportion would be retired. It was assumed that all patients who survived beyond 2 years had palliative treatment alone; however, patients can wait a long time for curative treatments such as transplantation (maximum waiting time for liver transplant was 1558 days, 95th percentile was 697). High-cost drugs were costed based on dosages reported for liver transplantation, but dosages may be influenced by other medications taken concurrently. Where the number of patients receiving a specific treatment was less than 50, treatments were combined, the radiotherapy pathway included patients receiving selective internal radiation therapy (SIRT) as only 13 patients were identified. By grouping treatments together, there is a loss of information; however, it is difficult to draw conclusions from small numbers. Costs for these patients are likely to be underestimated; total price to reimburse SIRT in an NHS centre was reported to be £21 500 in 2016.32 Technology appraisal guidance recently published by National Institute of Health and Care Excellence (NICE) recommends SIRT for patients with advanced HCC.33 Other high-cost therapies have been approved by NICE since 2016; Regorafenib,34 Lenvatinib,35 and immunotherapy-based Atezolizumab with bevacizumab;36 therefore, future costs are likely to be different to the historical costs presented.
While routine data presents its own methodological and practical challenges, it may provide greater real-world relevance.37–39 A limitation of this study was that the cirrhosis status was unknown for 50% of the patients, due to not being recognised before a diagnosis of advanced HCC, or not having cirrhosis. A systematic review of discharge coding accuracy compared routinely collected data in England, Scotland and Wales with case notes or clinical registry data, reported overall median diagnostic accuracy of 80.3% (IQR: 63.3% - 94.1%), and median procedure accuracy of 84.2% (IQR: 68.7%- 88.7%).40 Improved reporting and accuracy of coding will improve the quality of data available.
In contrast to other malignancies staging in HCC can be difficult; at present, staging data are not recorded in a sufficient number of patients and these data would add value to future analyses. Given the difficulty in separating the resource use specifically for HCC from that for underlying liver damage, understanding the complexities of what happens ‘pre’ diagnosis of HCC is an area for further inquiry.
Conclusion
The budget implications for secondary and tertiary healthcare for HCC for 5 years were estimated to be £245 million for England. Increased investment in education to prevent liver damage and diagnose primary liver cancer at an earlier stage is likely to be beneficial not only to the NHS but also across society given the impacts on patient’s lives and their families.
Most patients currently receive palliative care, with best supportive care being the most common patient pathway and survival is poor. Given this, it will be important to understand the health outcomes (i.e., health-related quality of life and/or survival gains) relative to the costs across the full pathway of care for patients diagnosed with HCC. To our knowledge, this analysis represents the first comprehensive description of the costs of HCC to NHS England, using a linked patient-level, population-based registry dataset. This snapshot is a starting point for further questions of the impact of HCC to patients, NHS and society.
Data availability statement
Data are available upon reasonable request. The data in this study were collected and analyzed under the National Disease Registries Directions 2021, made in accordance with sections 254(1) and 254(6) of the 2012 Health and Social Care Act. This study uses data that has been provided by patients and collected by the NHS as part of their care and support. The data are collated, maintained and quality assured by the National Disease Registration Service, which is part of NHS Digital. https://digital.nhs.uk/ndrs/about/ncras.
Ethics statements
Patient consent for publication
Acknowledgments
On behalf of the HCC-UK/BASL/NCRAS Partnership Steering Group
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AskSCHE, @asksche
Contributors DF is the principal investigator of the study. All authors contributed to the design of the analysis. MJ and KC developed the model. RP analysed the data. All authors participated in the discussion and interpretation of results. KC drafted the manuscript. All authors critically revised the manuscript and approved the final version. KC is responsible for the overall content as guarantor.
Funding The programme of research was supported by the British Association for the Study of the Liver who received an unrestricted and unconditional award from BTG International Ltd. BTG did not have any input into the design, analysis, or interpretation of the data, writing of the manuscript, review of the manuscript, the decision to submit the manuscript or the writing of this statement.
Competing interests AM is the Elected Chair of HCC UK, a special interest group within the British Society for the Study of Liver Disease (BASL), this role is unpaid. AB was employed by BASL from 2017 to 2020. DF was the principal investigator of the grant from BASL for income received to Swansea University to conduct the work contained in this paper. KC, MJ and DF have received funding from Gilead pharmaceuticals for research work outside of the submitted work. DF has received funding from the European Organization for Research Treatment of Cancer Quality of Life Group, the Swansea Bay University Health Board, Moondance Cancer Initiative for research work outside of the submitted work. DF and KC provide health economics expertise to the All-Wales Medicines Strategy Group. DF is a member of the European Organisation for Research and Treatment of Cancer (EORTC) GI group, pancreatic and hepato-biliary task forces, and Health Economic Member of the New Medicines Group, All Wales Medicines Strategy Group, and a member of the EORTC Quality of Life Group. IR has served as a consultant for Roche. TC reported unrestricted educational grants from Sirtex, Bristol Myers Squibb, and Bayer; lecture fees from Dr Falk and Roche; serving on advisory boards for Bristol Myers Squibb, Sirtex, and Roche; co-writing an article with Bristol Myers Squibb; shares with AstraZeneca; and receiving a meeting pass from Roche to attend a scientific meeting.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.